Uluslararası Bildiriler
370 - Can the plasma aldosterone/potassium ratio predict primary aldosteronism in patients scheduled for confirmatory testing? - 2025
Uluslararası Bildiriler Joint Congress of ESPE and ESE 2025: Connecting Endocrinology Across the Life Course, 10 -13 May 2025, Copenhagen, Denmark, Endocrine Abstracts May 2025, Volume 110, P122
Introduction: Primary aldosteronism (PA) is a common cause of endocrine hypertension, yet there are some difficulties in diagnosing the disease. A single normal or low aldosterone/plasma renin activity (PRA) ratio (ARR) alone may not be sufficient to exclude the diagnosis of primary aldosteronism (PA) (3-5). The saline infusion test (SIT), a standard confirmatory test, has limitations such as contraindications, need for hospitalization and high cost (6). This study evaluates the potential of the plasma aldosterone/potassium (A/K) ratio in predicting PA.
Methods: Between 2019 and 2023, 118 patients admitted to our Endocrinology outpatient clinic who underwent SIT with a prediagnosis of PA due to hypertension, as well as hypokalemia and/or elevated ARR were retrospectively included in the study. Patients who were pregnant, <18 years of age, had adrenal surgery and used diuretics were excluded. Demographic data, laboratory and adrenal imaging results were evaluated retrospectively. Aldosterone and concurrent potassium levels at the time of admission were obtained and A/K ratio was calculated. The diagnosis of PA was made according to the results of SIT, captopril confirmation test if available, adrenalectomy results and clinical judgment of the multidisciplinary council (7). All parameters were compared between the groups of patients with and without PA.
Results: A total of 118 patients who underwent SIT were included in the study. PA was diagnosed in 57 patients based on clinical and laboratory results. Male sex ratio was higher in the PA group (52.6% vs. 23.0%; P=0.001) (Table 1). Patients with PA had higher aldosterone levels (P<0.001) and ARR (P<0.001), but lower potassium levels (P<0.001) and PRA (P=0.01). The A/K ratio was significantly higher in the PA group (P<0.001). ROC analysis showed that an A/K ratio cut-off of 5.4 could distinguish PA patients from non-PA patients [AUC (95% CI) =0.811 (0.733-0.890), P<0.001], with 73.7% sensitivity and 77.0% specificity (Default 1). When this cut-off point was applied to the group of patients with indetermine SIT results, sensitivity was 71.4% and specificity 77.8%. Univariate and multivariate analyses indicated that a high A/K ratio increased the likelihood of a PA diagnosis, with an A/K ratio above 5.4 associated with a 4.585-fold higher risk (95% CI: 1.181-17.799, P=0.028) (Table 2).
Conclusion: The A/K ratio may predict PA. It offers advantages such as no need for pretest potassium or hospitalization, making it a useful supplementary parameter for diagnosing PA, particularly in patients for whom confirmatory tests are unsuitable.
369 - Comparative analysis of ventricular repolarization in patients with type 1 diabetes vs. control and patients using insulin pump vs. multiple daily injections. - 2025
Uluslararası Bildiriler Joint Congress of ESPE and ESE 2025: Connecting Endocrinology Across the Life Course, 10 -13 May 2025, Copenhagen, Denmark, Endocrine Abstracts May 2025, Volume 110, P404
Objective: The frequency of cardiovascular mortality is increased in type-1 diabetes mellitus(T1DM). Both hyperglycemia and hypoglycemia increase the risk of cardiac complications. This study aimed to use the ECG parameters of ventricular repolarisation times to assess the risk of arrhythmogenesis in patients with T1DM.
Methods: Age, sex, age at diagnosis of T1DM, duration of T1DM, insulin-pump use status, duration of insulin-pump use, biological and diabetic age at insulin pump insertion, continuous glucose monitoring(CGM) status, carbohydrate counting status, diet compliance status, history of technical problems with insulin-pump, total insulin doses, presence of hypertension, history of diabetic foot, hyperlipidemia, stroke, coronary heart disease, symptomatic hypoglycemia at least once a week, diabetic foot, peripheral vascular disease, hospitalization for hypoglycemia, presence of diabetic neuropathy, presence and type of diabetic retinopathy, diabetic nephropathy status, hemoglobin A1c(HbA1c) value, creatinine, microalbuminuria status, and spot urine microalbumin/creatinine ratio levels were recorded. Electrocardiographic(standard 12-lead ECG)
parameters, parameters corresponding to ventricular repolarisation times, and used as indicators of arrhythmogenesis were collected. These were P-wave, QRSwave, T-wave, PR-interval, QT, QTmax, QTmin, QTc, QTcmax, QTcmin, QTdispersion, QTc-dispersion, Tp-e, JTc, Tp-e/QT, Tp-e/QTc, index of cardioelectrophysiological-balance(iCEB). Obtained parameters were evaluated between patients with T1DM and the control group. In addition, the patient group was divided according to the method of insulin therapy used(basal-bolus insulin therapy vs insulin-pump) and compared within themselves.
Results: 125 patients with T1DM and 50 controls were included in the study. 62 patients were on basal-bolus insulin therapy, and 63 were on insulin pump therapy. Patients who used insulin pumps had lower HbA1c than those who did not(8.45G1. 60 vs 9. 62G2. 01, P = 0. 001). The incidence of symptomatic hypoglycaemia was lower in the insulin pump group, but the history of hospitalisation due to hypoglycaemia was similar in both treatment groups. Pwave, QT, QTmax, QTmin, QTc, QTcmax, QTcmin, Tp-e, and JTc were longer in T1DM patients(p values=0. 024, 0. 012, 0.007, 0.001, <0.001, <0.001, 0.001, 0.001, and 0.004, respectively). QRS duration was significantly shorter, and JTc, iCEB, and iCEBc were significantly longer in insulin pump patients(p values=0. 045, 0.031, 0.019, and 0.005, respectively).
Conclusion: In conclusion, patients with T1DM have prolonged ventricular repolarisation time and may be predisposed to arrhythmias. This study also suggests that insulin pump therapy may provide better glycemic control and less hypoglycemia. However, when assessing the effect of this condition on the risk of arrhythmia, it is essential to consider the patient’s medical history and to remember that the risk of arrhythmia may persist despite improvements in the course of the disease.
368 - From CRH to the desmopressin era: a comparative study of stimulation tests in cushing’s disease. - 2025
Uluslararası Bildiriler Joint Congress of ESPE and ESE 2025: Connecting Endocrinology Across the Life Course, 10 -13 May 2025, Copenhagen, Denmark, Endocrine Abstracts May 2025, Volume 110, P960
Purpose: CRH-based dynamic tests can be used in the differential diagnosis of ACTHdependent Cushing’s syndrome(CS) and the differentiation of CS from nonneoplastic hypercortisolism. However, after the worldwide cessation of CRH production as of December 2022, desmopressin-mediated dynamic tests are recommended as an alternative. In this study, we aimed to compare the responses of ACTH-secreting pituitary adenomas to desmopressin and CRH stimuli.
Methods: Patients who underwent a CRH or desmopressin-stimulation test for CS between December 2019 and September 2024 and who were histopathologically diagnosed with CD postoperatively were included in the study. Patients’ age, sex, screening test results for CS, baseline ACTH and cortisol levels, peak ACTH and cortisol levels during the tests, the test minute at which peak values were reached, and the rates of peak increase in ACTH(%D ACTH) and cortisol(% D Cort) after stimulation were recorded.
Results: A total of 30 CD patients were included in the study. Of these, 18 had a CRHstimulation test, and 12 had a desmopressin-stimulation test. 27 patients were female(90%), and three were male(10%). The mean age was 44.70G14.44 years. The results of the patients’ baseline and screening tests for CS are shown in Table 1. The basal and peak ACTH and cortisol levels of the patients during the stimulation tests and the comparison between groups are shown in Table 2. No
statistically significant difference was found when comparing the distributions of peak ACTH minutes and peak cortisol minutes of the tests(P = 0.580 and P = 0.518, respectively).
Conclusion: CRH and desmopressin stimulate ACTH and subsequent cortisol secretion to different degrees. Diagnostic criteria for CRH stimulation are well established, whereas this experience is not yet available for desmopressin. However, using similar diagnostic criteria for these two tests seems doubtful regarding diagnostic adequacy. To use the desmopressin stimulation test more effectively, prospective studies with large patient groups should be performed.
367 - Parathyroid washout’s role in accurate adenoma localisation and diagnostic cut-offs. - 2025
Uluslararası Bildiriler Joint Congress of ESPE and ESE 2025: Connecting Endocrinology Across the Life Course, 10 -13 May 2025, Copenhagen, Denmark, Endocrine Abstracts May 2025, Volume 110, P290
Purpose: Accurate adenoma localisation is necessary for the application of minimally invasive surgery, which is preferred in the treatment of primary hyperparathyroidism. This study aimed to determine appropriate cut-off values for the parathormone-washout(PTH-WO) method.
Design: A total of 402 PTH-WO assays from 339 patients were included in the study. The diagnostic accuracy of the test was assessed by accepting as a positive result a PTHWOresult higher than the serum PTHlevel [PTH-WO/serumPTH(PTHratio)O1]. In addition, a cut-off value for the test was established by evaluating the PTH washout results obtained in comparison with postoperative histopathology. Undiluted test results were not included to obtain a clear numerical value in this evaluation. The results of parathyroid scintigraphy and fine needle aspiration biopsy(FNAB) were compared with postoperative histopathology.
Results: While 309(76. 86%) of the PTH-WO procedures were considered positive, 93(23.13%) were considered negative if the PTH ratio was O1. When these results were compared with the postoperative histopathology, the test’s sensitivity was 92. 51%, and the specificity was 100. 00%. In the analysis of the remaining 292 PTH-WO samples after excluding the undiluted ones, the sensitivity and specificity of the method were 92.3% and 94.1%, respectively, with a PTH ratio>0. 99.With a cutoff value of 99.5 ng/l for PTH-WO value, 93. 1% sensitivity and 94. 3% specificity were obtained. The sensitivities of parathyroid scintigraphy and FNAB were 53. 4% and 15. 3%, respectively.
Conclusion: The PTH-WO method is safe and cheap, with high sensitivity and specificity in localising parathyroid adenoma. In cases where radiological methods cannot achieve localisation with specified cut-off values, it has high diagnostic accuracy.

366 - Is the coexistence of acromegaly with primary empty sella syndrome rare? - 2025
Uluslararası Bildiriler Joint Congress of ESPE and ESE 2025: Connecting Endocrinology Across the Life Course, 10 -13 May 2025, Copenhagen, Denmark, Endocrine Abstracts May 2025, Volume 110, EP1224
Objective: The association between growth hormone (GH)- secreting pituitary adenomas and primary empty sella (ES) has been reported mostly in case reports and is thought to be rare. In this study aimed to evaluate the coexistence of primary ES in newly diagnosed acromegaly and to investigate the effect of the presence of ES on the clinical and laboratory parameters of acromegaly.
Methods: Fifty-two patients with GH-producing pituitary adenomas who were followed up in our clinic between February 2017 and June 2024 and whose pituitary magnetic resonance imaging (MRI) was available at the time of diagnosis were analyzed retrospectively. Pituitary magnetic resonance imaging (MRI), computed tomography (CT) imaging, and pituitary function tests were evaluated. ES was defined as the pituitary gland and adenoma occupying less than 50% of the sella turcica on midsagittal magnetic resonance (MR) imaging. Demographic data, pituitary adenoma size, hormonal profile and postoperative pathologies of the patients were examined.
Results: Of 52 patients with acromegaly due to GH-producing pituitary adenomas, 27 (51.9%) were female and 25 (48.1%) were male (age range 21-73 years). Empty sella was detected in 8 (15.4%) patients and 2 had complete and 6 had partial empty sella. No ectopic adenoma cases were found in acromegaly patients with empty sella. No significant difference was found in preoperative pituitary hormone levels in patients with and without ES. Postoperative GH and insulin-like growth factor 1 (IGF-1) levels decreased in all patients.
Conclusion: This study showed that newly diagnosed acromegaly and primary ES coexisted in 15.4%. Acromegaly and ES coexisted more frequently than expected. The pathophysiology of this coexistence may be due to soft and hard tissue changes and serebrospinal fluid pressure changes that develop with the paracrine effect of GH during abundant GH production. The association between GH-producing adenomas and ES is not rare, but the underlying mechanism is not yet clear and requires further study
365 - THE CASE OF SUBACUTE THYROIDITIS IN AN ELDERLY PATIENT MIMICKING MALIGNANCY - 2024
Uluslararası Bildiriler Endobridge 2024, P-56, ANTALYA, TÜRKIYE, 17-20 OCTOBER 2024
Introduction: Subacute thyroiditis is a self-limiting inflammatory thyroid disease characterized by fever, neck pain, and thyroid dysfunction. It typically appears following an upper respiratory tract viral infection. Most cases of subacute thyroiditis are diagnosed through clinical and laboratory testing. The thyroid gland is large, painful, and tender during thyroid examination. Blood tests typically reveal elevated levels of free T4 and free T3, as well as a significantly increased sedimentation rate and C-reactive protein (CRP). Ultrasonographic findings of subacute thyroiditis are well defined.
Clinical Case: A 68-year-old male was consulted by the anesthesia department before the endoscopy and colonoscopy procedure planned to screen for malignancy. He was very worried and afraid because of the possibility of cancer and was psychologically negatively affected. He presented with night sweats and 10 kg of weight loss in the last 6 weeks. He had no history of previous disease. When a detailed history was taken, he stated that he had severe pain in his neck before his complaints started and that it went away on its own after a few weeks. On examination, he had no fever, a heart rate of 90 beats per minute, and a blood pressure of 120/80 mmHg. Neck examination showed no thyromegaly or lymphadenopathy. The general and systemic examination was unremarkable. Laboratory investigations showed hemoglobin 12.2 g/dL, WBC 8380 (x109/L), erythrocyte sedimentation rate (ESR) 78 mm/hour, CRP 50.1 mg/L, thyroid stimulating hormone 0.08 mIU/L (N = 0.55 - 4.78 mIU/L), free t4 1.4 ng/dL (N = 0.89 - 1.76 ng/dL), free t3 4.34 ng/L (N = 2.3 - 4.2 ng/L), and negative anti-thyroid peroxidase and thyroid stimulating immunglobulin. Thyroid ultrasonography was suggestive for subacute thyroiditis. He was given NSAIDS. Since his free T4 and T3 levels were normal at follow-up, endocrinological approval was given for the planned procedures. It was recommended to have a beta blocker ready during the procedure if needed. No findings in favor of cancer were detected in the detailed examinations, and the weight loss was attributed to subacute thyroiditis.
Conclusion: When elderly patients have complaints of weight loss or fatigue, it is important to exclude thyrotoxicosis and make a diagnosis by performing the necessary examinations. Subacute thyroiditis may not be severe; it is easy to diagnose with careful history-taking and simple laboratory examinations, and clinicians should keep it in mind in the differential diagnosis of weight loss.
364 - A RARE CAUSE OF TACHYCARDIA IN A POSTPARTUM FEMALE PATIENT WITH HYPOTHYROIDISM: LEFT ATRIAL MYXOMA - 2024
Uluslararası Bildiriler Endobridge 2024,P-55, ANTALYA, TÜRKIYE, 17-20 OCTOBER 2024
Introduction: Primary heart tumors are uncommon with cardiac myxoma being the most frequently observed type. This tumor occurs in about 0.03% of the general population, typically appearing sporadically in adults. It can also be inherited as part of the Carney complex. While cardiac myxoma is biologically benign, it behaves functionally as a malignant tumor due to its potential to cause obstruction within the heart, embolization, and various systemic symptoms. Hashimoto’s thyroiditis (HT) is a chronic autoimmune condition characterized by lymphocytic inflammation of the thyroid gland.
Clinical Case: A 39-year-old female patient with a diagnosis of primary hypothyroidism visited our outpatient clinic 18 months postpartum. She had palpitations for the past 4 years, which had worsened over the last 2 years and were now severe enough to disturb her sleep. Additionally, she complained of hand tremors when hungry, severe headaches, extreme weakness, and drowsiness after meals. Her medical history included a diagnosis of HT 16 years ago and she was receiving levothyroxine 100 mcg daily. She has lost her mother due to a cerebrovascular event at age 45. On physical examination, her blood pressure was 120/80 mmHg, her heart rate was 88 beats per minute, she had rosacea on her face, and the rest of the examination was normal. Laboratory analysis was as follows: TSH: 1.2mU/L (0.55-4-78), fT3: 3.24ng/L(2.3-4.2), fT4: 1.26ng/dl(0.89-1.76), Hb: 12g/dL(12-15.6), ferritin: 6 microgram/L(10-291), anti thyroglobulin: 269.9IU/mL (<1.3), anti thyroid peroxidase: 389U/mL (<60), glucose: 86mg/dl(70-99). During follow-up, her levothyroxine dose was reduced due to tachycardia, and she was also treated for iron deficiency anemia. Although an echocardiogram was planned to investigate her tachycardia, she did not undergo the procedure. An echocardiogram of the patient revealed an ejection fraction of 60% and a 4.3x3.3cm, wellcircumscribed, round shaped mass in the left atrium. This mass, which was attached to the interatrial septum with a stalk and deviated the septum to the right, was consistent with a myxoma and contained areas of calcification. The patient underwent surgery for the left atrial mass, and the pathology results confirmed cardiac myxoma. In evaluations for Carney complex, cortisol was suppresse with the 1 mg dexamethasone suppression test, the glucose-growth hormone (GH) suppression test showed GH levels <0.05 μg/L, and a genetic test could not be performed.
Conclusion: Tachycardia in hypothyroid patients can occur as a side effect of levothyroxine treatment. Additionally, iron deficiency anemia can also lead to sinus tachycardia in these patients. However, if a patient presents with unusual symptoms, such as nocturnal tachycardia, it is crucial to consider the possibility of an underlying cardiac condition. When cardiac myxoma is identified, it is important to evaluate the patient for Carney Complex.
363 - PITUITARY STALK INTERRUPTION SYNDROME: A CASE REPORT - 2024
Uluslararası Bildiriler Endobridge 2024, P-53, ANTALYA, TÜRKIYE, 17-20 OCTOBER 2024
Introduction: Pituitary stalk interruption syndrome (PSIS) is a congenital abnormality of the pituitary gland responsible for GH deficiency or global pituitary insufficiency and is usually characterized by the triad of a very thin or interrupted pituitary stalk, an ectopic (or absent) posterior pituitary (EPP), and hypoplasia or aplasia of the anterior pituitary visible on magnetic resonance imaging (MRI). The etiology of this syndrome is not fully understood, and many theories, like perinatal injuries or defective organogenesis due to genetic or environmental factors during pregnancy, are proposed. In family cases of PSIS, rare mutations of HESX1, LH4, OTX3, SOX3 and PROKR2 may be the cause. In the majority of cases, no genetic cause is found. The symptoms and signs of this syndrome typically become apparent in the neonatal period and childhood. Sometimes symptoms can be overlooked, and diagnosis can be delayed.
Clinical Case: A 22-year-old male presented in our clinic with hypothyroidism and growth hormone deficiency. He had previously received growth hormone (GH) treatment for 6 years until he was 15 years old. He was receiving levothyroxine therapy for hypothyroidism. Complete blood count, serum electrolytes, erythrocyte sedimentation rate, urinalysis, and thyroid function tests were normal. Hormonal analysis showed FSH: 11.9 U/L (N = 1.4-18.1 U/L), LH: 4.1 U/L (N = 1.5-9.3 U/L), prolactin: 9.1 μg/L (N = 5.4-15.4 μg/L), ACTH: 24.5 pg/mL (N = <46), fasting morning cortisol: 17.2 μg/dL (N = 5.2-22.4 μg/dL), total testosterone: 4.03 μg/L (N = 1.64-7.53 μg/L), free testosterone: 6.39 pg/mL (N = 5.4-40 pg/mL), IGF-1: 114 μg/dL (N = 161-384 μg/dL). Brain MRI revealed slightly hypoplastic sella turcica and adenohypophysis measuring 4.2 mm in height, thin infundibulum, and ectopic posterior pituitary located posterior to the infundibulum in the suprasellar cistern. The diagnosis of pituitary stalk interruption syndrome is mainly based on its clinical manifestations, laboratory tests, and imaging examinations.
Conclusion: PSIS is a rare congenital malformation that presents with significant growth and developmental challenges in children. The symptoms can be disregarded, and the diagnosis will therefore be delayed. Early diagnosis and treatment are crucial for improving growth outcomes and overall quality of life. It must be considered in the presence of combined or isolated hypopituitarism. MRI is the imaging modality of choice for the diagnosis of this condition. Regular monitoring and supportive care are essential components of effective management for these patients.
362 - Calcium to magnesium ratio can be a new marker for predicting nephrolithiasis in patients with primary hyperparathyroidism. - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, OC10.3.
Purpose: In previous studies, magnesium (Mg) was found to be lower in cases with more severe primary hyperparathyroidism (PHPT) and higher calcium (Ca) levels. This study evaluated the relationship between serum Mg and serum Ca and phosphorus (P) levels in PHPT and their utility in discriminating osteoporosis and nephrolithiasis.
Methods Patients: who were followed up with PHPT between March 2019 and March 2023 were analyzed retrospectively. Biochemical data, renal ultrasonography results, dual-energy x-ray absorptiometry reports, and technetium 99m sestamibi parathyroid scintigraphy reports were obtained. MgxP, Mg/P, Ca/P, and corrected Ca (cCa)/P values were calculated. The relationships between biochemical parameters and clinical outcomes were evaluated statistically.
Results: A total of 543 patients were included in the study. For Ca/Mg, a cut-off value of 5.47 had a sensitivity of 74% and a specificity of 73% for the presence of nephrolithiasis. The cut-off value for cCa/Mg that can be used to predict nephrolithiasis was 5.24, with a sensitivity of 73.3% and a specificity of 73%. No statistically significant correlation existed between the Mg/P, MgxP, cCa/Mg, Ca/Mg values, and DEXA results.
Conclusion: Ca/Mg and cCa/Mg ratios especially seem more valuable in discriminating nephrolithiasis than the currently used 24-hour urine Ca measurement. Unlike urinary Ca measurements, they are cheaper, more practical, and more accessible.
361 - Crooke cell corticotrop adenoma: case series. - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, EP1201.
Crooke cell corticotroph adenomas are a rare subtype of corticotroph adenomas. It can be detected in less than 1% of all pituitary adenomas. They are usually noticed as invasive macroadenomas on preoperative imaging. They are expected to have a more aggressive course and more frequent recurrences during their clinical course. We present a case series of 11 patients who were followed up with Cushing’s Disease in our clinic and were diagnosed with Crooke cell adenoma after surgery. Nine patients were female(81.8%), and 2(18.2%) were male. The average age of the patients was 41.0(19.0-71.0) years. There were macroadenomas in 6 patients(54.5%) and microadenomas in 5 patients(45.5%). The average largest tumor diameter was 14.00 (4.50-35.00) mm. Pituitary adenoma invaded surrounding tissues in 3 patients(27.3%). Optic chiasm compression was observed in 2 patients(18.2%). Preoperative hypopituitarism was present in 6 patients(54.5%). In this group of patients, macroadenoma was detected in 5 patients, and microadenoma was detected in 1. The patients’ preoperative laboratory parameters and clinical findings are given in Table 1 and Table 2, respectively. A 1-milligram dexamethasone suppression test was performed in all patients in the preoperative period, and it was found to be high in all patients. 24- hour urinary cortisol was measured in 8 patients and was high in 5. In the postoperative period, two patients could not be evaluated for remission because they continued their follow-up in another center. Biochemical remission was achieved in 4 of the other nine patients(44.4%), and biochemical remission was not achieved in 5(55.6%). Postoperative follow-up periods of patients in biochemical remission have been 33, 39, 56, and 62 months; no recurrence was observed in any patient during this period.
Table 1. Laboratory parameters of patients with Crooke cell corticotroph adenoma
Test | n | Minimum | Maximum | Mean |
ACTH(<46 pg/ml) | 11 | 13,50 | 443,00 | 108,8455 |
Cortisol(5.2-2.4µg/dl) | 11 | 11,10 | 60,00 | 31,0273 |
1 mg dexamethasone suppression test(<1.8µg/dl) | 9 | 3,90 | 43,56 | 21,1956 |
24-hour urinary cortisol(3.5-45 µg/day) | 8 | 24,66 | 2279,63 | 547,9125 |
Midnight salivary cortisol(<0.69 µg/dl) | 4 | ,64 | 2,28 | 1,6100 |
Table 2. Clinical findings of patients with Crooke cell corticotroph adenoma
Clinical finding | Present | Absent |
Central Obesity | 9(81.8%) | 2(18.2%) |
Proximal myopathy | 3(27.3%) | 8(72.7%) |
Moon face | 4(36.4%) | 7(63.6%) |
Abdominal purple striae | 3(27.3%) | 8(72.7%) |
Buffalo hump | 6(54.5%) | 5(45.5%) |
Hirsutism | 5(62.5%) | 3(27.3%) |
type 2 Diabetes Mellitus | 5(45.5%) | 6(54.5%) |
Hypertension | 5(45.5%) | 6(54.5%) |
Hyperlipidemia | 6(54.5%) | 5(45.5%) |
Osteoporosis | 1(9.1%) | 10(90.9%) |
History of thrombosis | 1(9.1%) | 10(90.9%) |
Hypokalemia | 3(27.3%) | 8(72.7%) |
360 - A rare association of salt-wasting congenital adrenal hyperplasia and type 1 diabetes mellitus - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, EP1092.
The co-occurrence of congenital adrenal hyperplasia and type 1 diabetes mellitus (T1DM) is a rare phenomenon in existing literature. The primary cause of congenital adrenal hyperplasia (CAH) is often 21-hydroxylase deficiency (21OHD), a condition associated with the CYP21A2 gene located on chromosome 6p21.3 within the major human leukocyte antigen (HLA) histocompatibility locus. Various gene polymorphisms, particularly in HLADQalpha, DQbeta, and DR genes on chromosome 6p21.32, are known to influence the risk of type 1 diabetes. Although the genetic loci for T1DM and 21- OH CAH are close, these conditions typically manifest independently, we present a case involving a man in his 20s who visited the emergency department with symptoms such as nausea, vomiting, headache, fatigue, and excessive sleepiness. This individual had a history of both classic salt-wasting congenital adrenal hyperplasia and type 1 diabetes mellitus. Over the past decade, the patient had experienced recurrent hospitalizations for diabetic ketoacidosis, with recent complications arising from the malfunction of an insulin pump due to technical issues. Initial treatment included insulin infusion, intravenous hydration, and an increased hydrocortisone dose. Once acidosis resolved, the patient transitioned to basal-bolus therapy and resumed insulin pump use. Carb counting was introduced, and dietary adjustments were made. An abdominal computed tomography scan revealed bilaterally thickened adrenal glands, and scrotal ultrasound detected an adrenal rest tumor. The patient was discharged with oral hydrocortisone (30 mg once daily), oral fludrocortisone (0.2 mg once daily), and continued use of an insulin pump. Repeated ketoacidosis episodes were potentially linked to hydrocortisone use, prompting consideration of a connection between T1DM and 21OHD, necessitating further investigation through additional studies
359 - Radiation thyroiditis after radioactive iodine treatment - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, EP1043.
Radioactive iodine therapy (RAI) is a treatment method used to in cases of Graves’ disease(GD), toxic multinodular guatr and solitary toxic nodu¨le and residual tissue after thyroidectomy or in the treatment of metastases capable of capturing iodine. The biological basis of the treatment is the inhibition of follicle cell functions. Side effects such as thyroid swelling, radiation thyroiditis and sialadenitis are rare. Radiation thyroiditis tends to occur within two weeks after RAI administration and is generally asymptomatic in most patients. Approximately % 1-5 of patients with GD develop radiation thyroiditis after RAI treatment. Radiation causes ınflammation that develops as a result of exposure of a large residual tissue to a high radiation dose may cause tenderness in the thyroid tissue or neck, erythema and edema, pain when swallowing, rarely airway obstruction, and in some patients, a thyrotoxic state. Symptoms generally begin 1- 10 days after treatment. Pain and tenderness in the thyroid and neck area are mild and disappear within 3-7 days. There may be a temporary hyperthyroidism attack at this time. Mild symptoms are usually relieved with non-steroidal antiinflammatory drugs. In more severe cases, corticosteroid treatment (30 mg/day prednisone) provides rapid relief of symptoms. In case of thyroid storm, symptoms can be controlled with corticosteroids, if severe adrenergic symptoms are accompanied by beta blockers and if necessary antithyroid drugs. Here we will present a case of radiation tyroditis developing after Graves Diseaes(GD). A 71- year-old patient with a diagnosis of Graves’ disease was treated with 20 mcı radioactive iodine due to elevated liver function tests under antithyroid drug therapy. 1 week after radioactive iodine treatment, she was admitted to our outpatient clinic with complaints of pain in the throat and difficulty swallowing. Thyrotoxicosis was detected in the tests. Oral cavity looked natural and sensivity was detected in the neck area. No respiratory distress was detected. Newyl developed tracheal stenosis was detected on the cervical graphy. Color doppler pattern 3 and edema in the thyroid gland was detected on the ultrasonography. The patient ‘s complaıns were primarily evaluated as thyroiditis secondary to radıoactive iodine treatment. The patient was started on oral methylprednisolone sodıum succinate, non-steroidal anti-inflamatory and betablocker treatment. The patient’s complaints regressed under treatment. In conclusion, radiation thyroiditis is a complication of RAI for the treatment of GD and may cause morbidity. Radiation thyroiditis should be suspected as the etiology of patients presenting with neck pain and difficulty swallowing immediately after RAI
358 - Cushing’s vs pseudo-cushing’s: neutrophil-lymphocyte ratio assessment - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, EP1027.
Aim: In patients with papillary thyroid carcinoma (PTC), the incidence of subacute thyroiditis (SAT) is thought to be more frequent than estimated. The incidence of thyroid cancer is between 2.3% and 21.1% in Graves’ Disease (GD).
Case: A 31-year-old female patient applied with complaints of amenorrhea and hair loss in the 10th postpartum month. There was no history of COVID-19 infection, but Biontech vaccine were administered two years ago. Her family history revealed GD in her sister. On physical examination, blood pressure was 120/1 mm/Hg, pulse rate was 83 beats/min. Laboratory values were TSH:!0.1 mU/l (0.55-4.78), freeT4:2.1 ng/dl (0.89-1.76), freeT3:11.1 ng/l (2.3-4.2), antithyroglobulin:2.7 IU/ml (!13), antithyroidperoxidase: 10235 U/ml (!60), thyroid stimulating immunglobulin: 6.34 IU/l (0.1-0.55), TSH receptor antibody: 3.63 IU/l (!1.5). The patient refused thyroid scintigraphy because of breastfeeding. She admitted with severe pain over the right thyroid lobe the next day. There was tenderness in the right thyroid area and the body temperature was 37.58. Thyroid US revealed hypoechoic heterogeneous areas in the superior anterior and the inferior anterior regions of the right lobe, a 16x24x1 mm isoechoic nodule with areas of cystic degeneration in the superior region and a 22x38x1 mm conglomerated isoechoic nodule with areas of cystic degeneration in the inferior region of left lobe. In laboratory analysis, TSH:!0.1 mU/l, freeT4:2.1 ng/dl (0.89-1.76), freeT3:15.1 ng/l (2.3-4.2), sedimentation rate: 1 mm/hour(0-20), CRP:8.1 mg/l (0-5). Her pain regressed and CRP values returned to normal after one week with NSAID treatment. However, since thyrotoxicosis did not resolve (TSH:!0.1 mU/l (0.55- 4.78), free T4:3.05nd/dl(0.89-1.76), free T3: 18.1 ng/l (2.3-4.2), methimazole treatment was started. On the control thyroid US, heterogeneous hypoechoic areas have resolved. The thyroid FNAB cytology result of the dominant nodule in the left lobe was suspecious for follicular neoplasia and hurtle cell type. The patient underwent bilateral total thyroidectomy, and an infiltrative follicular subtype PTC 0.1 cm in diameter was observed in the right lobe in addition to hyperplastic colloidal nodules in non-tumor thyroid tissue.
Conclusion: SAT can be seen rarely in patients with PTC. In the literature, there are cases diagnosed with GD after SAT, cases of SAT concurrent with GD, and cases of concurrent GD and SAT after COVID-19 infection. Considering that the incidence of combinations of these three diseases is very rare, our patient is the first case in the literature with all three diagnoses
357 - Atypical subacute thyroiditis associated with papillary thyroid carcinoma in a case of Graves’ disease - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, EP960.
Aim: In patients with papillary thyroid carcinoma (PTC), the incidence of subacute thyroiditis (SAT) is thought to be more frequent than estimated. The incidence of thyroid cancer is between 2.3% and 21.1% in Graves’ Disease (GD).
Case: A 31-year-old female patient applied with complaints of amenorrhea and hair loss in the 10th postpartum month. There was no history of COVID-19 infection, but Biontech vaccine were administered two years ago. Her family history revealed GD in her sister. On physical examination, blood pressure was 120/1 mm/Hg, pulse rate was 83 beats/min. Laboratory values were TSH:!0.1 mU/l (0.55-4.78), freeT4:2.1 ng/dl (0.89-1.76), freeT3:11.1 ng/l (2.3-4.2), antithyroglobulin:2.7 IU/ml (!13), antithyroidperoxidase: 10235 U/ml (!60), thyroid stimulating immunglobulin: 6.34 IU/l (0.1-0.55), TSH receptor antibody: 3.63 IU/l (!1.5). The patient refused thyroid scintigraphy because of breastfeeding. She admitted with severe pain over the right thyroid lobe the next day. There was tenderness in the right thyroid area and the body temperature was 37.58. Thyroid US revealed hypoechoic heterogeneous areas in the superior anterior and the inferior anterior regions of the right lobe, a 16x24x1 mm isoechoic nodule with areas of cystic degeneration in the superior region and a 22x38x1 mm conglomerated isoechoic nodule with areas of cystic degeneration in the inferior region of left lobe. In laboratory analysis, TSH:!0.1 mU/l, freeT4:2.1 ng/dl (0.89-1.76), freeT3:15.1 ng/l (2.3-4.2), sedimentation rate: 1 mm/hour(0-20), CRP:8.1 mg/l (0-5). Her pain regressed and CRP values returned to normal after one week with NSAID treatment. However, since thyrotoxicosis did not resolve (TSH:!0.1 mU/l (0.55- 4.78), free T4:3.05nd/dl(0.89-1.76), free T3: 18.1 ng/l (2.3-4.2), methimazole treatment was started. On the control thyroid US, heterogeneous hypoechoic areas have resolved. The thyroid FNAB cytology result of the dominant nodule in the left lobe was suspecious for follicular neoplasia and hurtle cell type. The patient underwent bilateral total thyroidectomy, and an infiltrative follicular subtype PTC 0.1 cm in diameter was observed in the right lobe in addition to hyperplastic colloidal nodules in non-tumor thyroid tissue.
Conclusion: SAT can be seen rarely in patients with PTC. In the literature, there are cases diagnosed with GD after SAT, cases of SAT concurrent with GD, and cases of concurrent GD and SAT after COVID-19 infection. Considering that the incidence of combinations of these three diseases is very rare, our patient is the first case in the literature with all three diagnoses
356 - Silent gonadotroph adenomas and platelet dynamics - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, EP885.
Objective: Gonadotroph adenomas are the most common subtype of pituitary adenomas. Rarely, clinical findings may occur due to the secretion of high amounts of biologically active gonadotropins. It may affect platelet activity if there is an excessive increase in the release of estrogen and testosterone or if it is used in pharmacological doses. In this study, we aimed to investigate whether platelet activity indices and coagulation parameters were affected in silent gonadotroph adenomas.
Methods: Patients who operated for a pituitary adenoma in our center between March 2019 and July 2023 were recruited for the study. Presence of thromboembolic disease history, preoperative and postoperative (after the first month) follicle-stimulating hormone (FSH), luteinizing hormone (LH), total testosterone, free testosterone, estradiol (E2), platelet count, mean platelet volume (MPV), platelet distribution width (PDW), international normalized ratio (INR) and activated partial thromboplastin time (aPTT) levels of the patients were recorded.
Results: 25 female patients and 32 male patients were included in the study. We found no statistically significant difference between FSH, LH, testosterone, and E2 levels in both genders’ preoperative and postoperative periods. No statistically significant difference was observed in MPV, PDW, INR, and aPTT in both genders. None of the patients in the study had a history of thromboembolic events. No thromboembolic event was observed in any patient within the first year of the postoperative period.
Conclusion: Silent gonadotroph adenomas do not affect platelet activity in male and female patients
355 - Medullary thyroid carcinoma presenting with carcinoid syndrome: a case report - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, EP825.
Introduction: Medullary thyroid cancer (MTC) is characterized by elevated calcitonin levels, stemming from genetic factors or occurring sporadically. Carcinoid syndrome involves symptoms triggered by substances released by tumors, such as hormones and amines. This case report details a patient who developed carcinoid syndrome linked to medullary thyroid cancer.
Case: A 77-year-old male presented with flushing, diarrhea, and dizziness. No other health issues or medication use were reported, except for flushing and hypotension during a hemorrhoid operation a year ago. While routine tests showed normal results, neck CT revealed calcified nodules in the thyroid and pathological lymph nodes. Calcitonin was elevated at 11312 pg/ml, CEA at 126 ng/ml. Thyroid ultrasound displayed a 19.1!21!35.9 mm calcified nodule with pathological cervical lymph nodes. Ga-68-DOTA-PET confirmed thyroid and cervical involvement. Fine needle aspiration biopsy confirmed medullary carcinoma. Catecholamine and 5-HIAA levels were normal. Chromogranin was normal. Surgery was planned for MTC, involving bilateral total thyroidectomy and lymph node dissection. Sandostatin infusion was initiated for carsinoid symptoms 24 hours before surgery, continuing intraoperatively and 48 hours postoperatively, gradually decreasing over a week. Postoperatively, calcitonin was 639 pg/ml, CEA 110 ng/ml on day one. Three months later, similar symptoms recurred, with calcitonin at 2600 pg/ml . Re-operation confirmed MTC, with a 5 cm retrosternal mass in the right lobe. Postoperatively, calcitonin decreased to 312 pg/ml . Two months later, a patient with similar complaints had a calcitonin level of 261 pg/ml, and residual tissue? was observed in the right lobe on thyroid ultrasonography. A spherical lymph node with the largest size of 10 cm was identified in the right level IV. Biopsy results were non-diognastic, and calcitonin washouts results of 4.9 pg/ml and 15.2 pg/ml, respectively. Due to ongoing symptoms, the patient was readmitted with a preliminary diagnosis of carcinoid syndrome, and short-acting sandostatin was initiated. After the post-operative follow-up Ga-68 DOTA-PET, as regression and the absence of new metastases were observed, tyrosine kinase inhibitors were not considered. The patient was discharged with lanreotide 120 mg/month, and no attacks were observed following the treatment.
Conclusion: MTC can manifest with flushing in carcinoid syndrome. When diagnosing flushing, consider MTC, pheochromocytoma, pancreatic tumors, hyperthyroidism, and male hypogonadism. Treating carcinoid syndrome involves addressing the underlying disease, and also sandostatin relieves symptoms in these patients. Keep MTC in mind when patients present with flushing or carcinoid syndrome.
354 - A case of graves with recurrence after mepolizumab treatment - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, EP623.
Introduction: Targeted therapies and monoclonal antibodies are known to trigger thyroid autoimmunity. No case of autoimmune thyroid disease with mepolizumab, an anti-IL-5 monoclonal antibody, is reported in the literature. In this case report, we present a case of Graves’ disease that recurred after Mepolizumab treatment.
Case: A 74-year-old male patient was referred to the endocrinology outpatient clinic upon detection of hyperthyroidism on 11/2021. The patient, who had known aortic valve replacement, allergic asthma, and benign prostatic hyperplasia, was using warfarin 1!5 mg, atorvastatin 1!20 mg, inhaler salmeterol, 1!5 mg levocetirizine and 1!8 mg silodesin. In the patient’s examinations, TSH !0.008 mU/l, free T4:3.94 ng/dl, free T3:11.99 ng/l, anti-tg:2.4 IU/ml, and TSH receptor antibody (TRAB):6.77 IU/l (!1.5 IU). /l) was seen. On electrocardiography, his pulse was 98 beats/minute, and his rhythm was normal sinus rhythm. While no nodule was detected in the patient’s thyroid ultrasonography, bilateral parenchymal heterogeneous and sparse patchy hypoechoic areas were observed. Color flow doppler pattern was observed as 2 in thyroid doppler. The patient, who had no history of recent contrast exposure or amiodarone use, was evaluated as having Graves’ disease, and methimazole 3x5 mg and propranolol 2x20 mg were started. No signs of ophthalmopathy were detected in the eye examination performed at the time of diagnosis. After one month, propranolol was discontinued, and methimazole dosage was adjusted, and periodic checks were scheduled. On 05/2023, in the 19th month of treatment, while receiving methimazole 1!2.5 mg treatment, TSH was measured:2.4 mU/l, free T4:1.04 ng/dl, free T3:3.62 ng/l, thyroid stimulating immunoglobulin was 0.52 IU/l (0.1- 0.55 IU/l). The treatment was discontinued at this point. In the follow-ups performed one month and two months later, it was observed that the patient was euthyroid. On 07/2023, as the patient’s complaints about allergic asthma increased, the pulmonologist started Mepolizumab to be administered 100 mg subcutaneously once a month. On 09/2023, after the patient received two doses of mepolizumab, TSH:0.02 mU/l, free T4:1.86, and free T3:4.68 ng/l were observed in the controls performed in our outpatient clinic, and the patient was started on methimazole 1!5 mg again. The patient, who was evaluated as having a relapse of Graves disease, was assessed in a multidisciplinary council, and radioactive iodine treatment was planned.
Conclusion: Thyroid autoimmunity may be triggered after Mepolizumab, an anti-IL-5 monoclonal antibody. Patients receiving this treatment should also be followed in this respect.
353 - Evaluation of dry eye parameters and vitamin E levels in patients with papillary thyroid carcinoma - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, EP508.
Aim: Dry eye syndrome(DES) is a common finding in patients with thyroid orbitopathy. There are few studies on DES in patients with papillary thyroid cancer (PTC). Retinal pathology may develop in case of vitamin E deficiency, which has antioxidant, anti-inflammatory and anti-apoptotic properties.
Materials and Methods: In our study, 29 patients who received radioactive iodine (RAI) treatment (Group 1) and 22 patients who did not receive RAI treatment (Group 2) with a diagnosis of PTC were included. 26 healthy individuals without PTC were determined as the control group (Group 3). Exclusion criteria were diabetes mellitus, rheumatologic diseases, keratoconus, glaucoma, history of contact lens use, previous eye surgery. Ocular surface disease index, meibomian gland secretion quality, lid margin score, noninvasive tear breakup time were evauated with sirius device and meibomagraphy in all patients. Thyrotropin (TSH), free thyroxine, free triiodothyronine, and vitamin E levels were measured.
Results: TSH levels were significantly lower in Group 1 and 2 compared to Group 3 (P!0.001, P!0.001, respectively). There was no significant difference between the groups in terms of vitamin E levels (PZ0.599). The proportion of those with normal noninvasive tear breakup time (O17) was similar in Group 1, Group 2 and Group 3 (30.8%, 27.3%, and 44.6%, respectively, PZ0.145). The proportion of those with an upper lid margin score of R1 was significantly higher in Group 1 and Group 2 than in the control group (64.9%, 56.8% and 17.9%; respectively, PZ0.025). Lower meibomian gland expressivity was O1 in 34.5% of the patients in Group 1, 22.7% in Group 2, and 7.1% in Group 3 (PZ0.002). The proportion of patients with lower meibomiagraphy values of R1 was significantly higher in Group 1 and Group 2 compared to the control group (61.1%, 52.5%, and 29.5%, respectively, PZ0.007). There was no significant difference between the groups in terms of lower lid margin score, Oxford values, upper meibomian gland expressibility, and upper meibomiagraphy grades (PZ0.485, PZ0.064, PZ0.256 and PZ0.069, respectively). OSDI (survey questioning eye-related irritation symptoms) values were 6.25 in Group 1 and 8.12 in Group 2 and were significantly higher than the control group (2.27) (PZ0.034).
Conclusion: Meibomian gland dysfunction is observed in patients with PTC who received and did not receive RAI. This may be related to TSH suppression. It is important to question these patients for a dry eye because it might affect their daily living activities
352 - The correlation between the presence of histopathologically different subtypes and aggressive behavior and recurrence in patients with papillary thyroid carcinoma - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, EP507.
Aim: Papillary thyroid cancer (PTC) accounts for 85% of thyroid cancers. Classical PTC has a 10 year survival rate of over 95%. Although the histopathological diagnosis of thyroid tumors, which started in the 1950s, has improved significantly in the last few decades, the effect of aggressive subtypes on survival has not been fully clarified. In our study, we investigated the effect of aggressive cytologic subtypes on behavior and prognosis in patients followed up with a diagnosis of PTC.
Method: Our retrospective study included 484 patients who underwent bilateral total thyroidectomy and were diagnosed with PTC. There were 11 patients with aggressive subtype (columnar cell, tall cell, diffuse sclerosing, solid, hobnail PTC), 382 patients with nonaggressive subtype (papillary, follicular PTC), and 91 patients with mixed subtype. 36 month follow-up results were analyzed. Demographicall findings, imaging and laboratory results, histopathological features (tumor diameter, capsule invasion, vascular invasion, extrathyroidal invasion, lymphatic invasion, distant metastasis), radioactive iodine (RAI) treatment were noted from the records. Dynamic risk scoring (excellent response, biochemical incomplete response, structural incomplete response, indeterminate response) was performed.
Results: The mean age at diagnosis was lower in the aggressive subtypes (44.36G10.63) than in the nonaggressive and mixed subtypes (46.14G12.82 and 47.71G13.24, respectively) (PZ0.501). Tumor size was significantly larger in the aggressive subtypes (1.83G2.27 cm) than in the nonaggressive and mixed subtypes (1.21G 1.1 cm and 1.60G1.1 cm, respectively) (PZ0.019). According to the American Thyroid Association (ATA) risk classification, the proportions of those identified as intermediate and high risk were higher in the aggressive and mixed subtypes (72.7% and 68.1%, respectively) than in the nonaggressive subtypes (23.9%) and the difference was statistically significant (P!0.001). Remission, persistence, recurrence and metastasis rates during follow-up did not differ significantly between groups (PZ0.926, PZ0.903, PZ0.776 and PZ0.920, respectively). There was no significant difference in treatment responses according to dynamic risk scoring after initial treatment 6-12 months, 12-18 months, 18-24 months, 24- 36 months (PZ0.931, PZ0.961, PZ0.892, PZ0.698, respectively).
Conclusion: In our study, we found that tumor size was larger in the aggressive subtype, and those with intermediate and high risk, according to the ATA risk classification, were more common in the aggressive and mixed subtypes. In patients with PTC, aggressive and mixed subtypes in the initial treatment phase may create differences in approach, and further studies are needed.
351 - A case of levothyroxine malabsorption corrected with vitamin c - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, EP362.
Introduction: Malabsorption of levothyroxine is an important clinical problem. Changes in gastric pH due to various medical conditions might cause challenges in maintaning normal TSH values. Case: A forty-nine years old female who has been followed up with a diagnosis of primary hypothyroidism for 12 years admitted to our outpatient clinic with a complaint of unachievement of euthyroidism despite increasing the levothyroxine dose up to 200 mg. He did not have any other chronic disease and was not using any other medication. In laboratory examination, free T3 was 1.14 ng/l (2.3 - 4.2), free T4 was 0.32 ng/dl (0.89 - 1.76) and TSH was 129 mU/l (0.55 - 4.78). Thyroid autoantibodies were markedly high (antithyroglobulin O1000 IU/ml and antithyroid peroxidase antibody O13000 U/ml) and thyroglobulin was !0.20 mg/l Tthyroid ultrasonography showed heterogeneous parenchyma with widespread patchy hypoechoic areas and thin-thick fibrous bands. Free T4 was was measured just before and after the administration of oral levothyroxine 200 mg. Basal, first hour and second hour free T4 were 0.23 ng/dl, 0.29 ng/dl and 0.29 ng/dl, respectively. A malabsorption test was performed with 500 mg levothyroxine. Accordingly, free T4 was 0.40 ng/dl at basal state, 0.41 ng/dl in the first hour, 0.50 ng/dl in the second hour and 0.47 ng/dl in the fourth hour. Thus, free T4 level increased by a maximum of 25%. The patient’s celiac and anti-pariatel cell antibodies were negative. Helicobacter Pylori antigen tested in the stool was detected positive. The patient’s upper gastrointestinal endoscopy revealed antral gastritis and colonoscopy revealed Grade 1 internal hemorrhoids, He was given 1000 mg/day vitamin C. At the third day of vitamin C, serial free T4 levels were measured after ingestion of 250 mg levothyroxine. While basal TSH was 112 mU/l and free T4 was 0.5 ng/dl, free T4 increased to 0.71 ng/dl at the first, 0.80 ng/dl at the second and 0.80 ng/dl at the fourth hour. A maximum increase of 60% in free T4 value was detected.
Conclusion: There are publications in the literature showing that vitamin C corrects abnormalities in serum free T4, T3 and TSH in patients with hypothyroidism and gastrointestinal pathology. Although the mechanism was not explained clearly, it was suggested that decreasing pH via vitamin C might increase the absorption of the drug. Co-administration of vitamin C with L-T4 may be useful in the treatment of patients with high TSH values despite high doses of L-T4.
350 - Insulin autoimmune syndrome due to alpha lipoic acid: a case report - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, EP84.
Insulin autoimmune syndrome is a condition characterized by production of autoantibodies against insulin. Drugs are one of the ethiological factors, especially when they contain the sulfydryl group such as methimazole and alpha lipoic acid. Herein we present a case report of insulin autoimmune syndrome due to alpha lipoic acid. A 77 year-old female patient presented to emergency department with syncope because of hypoglycemia. She was diagnosed with type 2 diabetes mellitus a year ago. Metformin and gliclazide was prescribed. During her follow-up, she had complaints of neuropathy, so alpha lipoic acid was added to her treatment. She also had autoimmune thyroid disease but didnot need for levothyroxine replacement. When she was questioned it was learned that she hadnot been taking metformin and gliclazide aproximately for 2 weeks, but she continued to take alpha lipoic acid. During a hypoglycemic episode insulin and c-peptide levels were examined and was compatible with hyperinsulinemic hypoglycemia. Anti-insulin antibody titer was high. She was considered to have insulin autoimmune syndrome due to alpha lipoic acid. Alpha lipoic acid was stopped, afterwards hypoglycemia was ceased, anti-insulin antibody titer decreased accordingly. There are several case reports of insulin autoimmune syndrome presented in literature due to intake of alpha lipoic acid. All of the cases had autoantibodies against insulin at presentation, cessation of hypoglycemia and deacrease of anti-insulin antibody titer after discontinuation of alpha lipoic acid. There are certain HLA allels which causes predisposition to this syndrome. Also these patients have higher incidance of other autoimmune diseases. If a patient who takes a drug containing sulfydryl group and has any of the autoimmune diseases presents with hyperinsulinemic hypoglycemia, insulin autoimmune syndrome must be considered.
349 - A rare cause of bone pain: Fibrodysplasia ossificans progressiva - 2024
Uluslararası Bildiriler 26th European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden, Endocrine Abstracts May 2024, Vol 99, P246.
Introduction: Fibrodysplasia ossificans progressiva (FOP), also known as stone man disease, is a rare connective tissue disorder with a prevalence of 1 in 2 million. It is caused by a mutation in ACVR1 gene, usually sporadic and sometimes with autosomal dominant (AD) inheritance. These patients are normal at birth except for the short great toes and hallux valgus. Over time soft tissues such as ligaments, skeletal muscles or tendons ossify. Diaphragm, tongue, extraocular and cardiac muscles are spared.
Clinical case: A 32-year-old female with severe bone pain and hip contracture applied to our clinic. In her history, at age 8 she was admitted to hospital due to lump on her back. The biopsy result of the lesion was reported as fibrotic fat tissue and she was discharged. Two years later at age 10 she was admitted to hospital again due to protrusion and pain in the area where the biopsy was taken. The second biopsy taken from the left thoracic wall was reported as heterotopic endochondral ossification. Further examination of the case for FOP was recommended. Genetic testing could not be done due to the family’s financial difficulties. Over the years, painful swellings continued to develop in various regions. When the patient’s daughter was 5 years old, the same painful swellings began to occur. This time genetic testing was done on both. Mutation was detected positive for ACVR1 gene for both. (NM_001105.5, c.617GOA (p.R206H) (p.Arg206Pro) (Heterozygote)). During our examination, many painful ossification areas were detected in different regions such as the back, dorsum of foot and chest wall. In addition, contracture of the left hip joint occurred in external rotation and abduction. She also had short big toes and hallux valgus. No abnormalities were detected in laboratory tests. In plain radiographs, pseudoexostoses were seen in various parts such as left sided thoracic wall, left iliopsoas muscle and adductor magnus muscle. Also, monophalangic great toes were noted (Figure 1). Since there was no treatment to prevent the progression of the disease, we administered ibuprofen for symptomatic treatment and glucocorticoid to use during painful flare-ups.
Conclusion: FOP is a rare disease that reduces quality and duration of life. Where heterotopic ossification is detected clinically or radiologically, FOP should be kept in mind. Since it can be inherited AD, genetic testing and counseling should be provided in case of clinical suspicion
348 - A Pituitary Neoplasm with an Aggressive Course: Silent Corticotroph Adenoma - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, EP818
Patient is a 43 years old female without any known additional disease. A pituitary mass was seen in the cranial MRI taken due to the complaint of forgetfulness. Pituitary MRI of the patient revealed a ’large intrasellar mass of 3.2x3x2.3 cm, which expanded the sella and pressed the optic chiasm’. The patient didn’t describe any symptoms other than forgetfulness. She didn’t have galactorrhea, cushingoid or acromegaloid appearance. Patients laboratuary evaluation can be seen in Table 1. The patient was started on levothyroxine for central hypothyroidism and it was thought that the patient had a non-functional pituitary adenoma. In the follow-up of the patient who underwent transsphenoidal surgery, no hypopituitarism or central diabetes insipidus was detected. In the immunohistochemical and histological examination of the patient’s surgical material:’Tumor cells showed diffuse staining with ACTH. GH, PRL, TSH, FSH, LH are negative. The Ki-67 proliferation index was 3-4%.’These findings, patient’s pre-operative examinations and clinically situation were evaluated and it was determined that the patient had a ’silent corticotroph adenoma’. The patient had no complaints in the post-operative first month. Her anterior pituitary hormones were observed(Table 2). Due to the tendency of silent corticotroph adenomas to progress aggressively, pituitary MRI control was planned at the postop 3rd month. Silent corticotroph adenomas constitutes 4.8-6.8% of all pituitary adenomas and 19% of non-functioning pituitary adenomas. It has a highly aggressive and invasive course. It often recurs after treatment and is resistant to treatment. In the studies,0.5 mg DST performed with a cut-off value of 3.0µg/dl in the screening of Cushing’s syndrome. That has been shown to have higher sensitivity and specificity than the classical 1 milligram DST. In our case, both screening tests were applied.
Table 1 Biochemistry and pre-operative anterior pituitary hormone examination results
Glucose | 83mg/dl | TSH(0,55-4,78 mU/l) | 0,90mU/l |
ACTH(<46pg/mL) | 17,3 µg/dl | Free T4(0,89-1,76 ng/dl) | 0,75ng/dl |
Cortisol(5.2-22.4 µg/dl) | 16,6 µg/dl | Free T3(2,3-4,2 ng/l) | 2,20ng/l |
FSH(post-menopausal 23-116.3U/l) | 9,0U/l | IGF-1(65-200 µg/l) | 133 µg/l |
LH(post- menopausal 15,9-54 U/l) | 2,1U/l | Growth Hormone(0,05- 8 µg/l) | 1,4 µg/l |
Estradiol (post- menopausal< 32,2ng/l) | 27,0ng/l | Sodium(132-146mEq/l) | 141mEq/l |
Diluted Prolactin(2,8- 29,2 µg/l) | 28,57 µg/l | Potassium(3,5- 5,5mEq/l) | 4,1mEq/l |
1 milligram DST(< 1,8µg/dl) | 1,6µg/dl | Urinary density(1003- 1030) | 1022 |
Table 2 Biochemistry and anterior pituitary hormone test results in post-operative first month
Urinary density(1003- 1030) | 1014 | TSH(0,55-4,78mU/l) | 2,60mU/l |
ACTH(<46pg/mL) | 49,6 µg/dl | Free T4(0,89- 1,76ng/dl) | 0,98ng/dl |
Cortizol(5.2-22.4µg/dl) | 25,3µg/dl | Free T3(2,3-4,2ng/l) | 2,35ng/l |
FSH(post-menopausal 23-116.3U/l) | 7,1U/l | IGF-1(65-200µg/l) | 150µg/l |
LH(post- menopausal 15,9-54U/l) | 1,6U/l | Growth Hormone (0,05- 8µg/l) | 0,7µg/l |
Estradiol(post- menopausal< 32,2 ng/l) | 25,0ng/l | Sodium(132-146mEq/l) | 141mEq/l |
Prolactin(post- menopausal 1,8-20,3mg/l) | 34,1µg/l | Potassium(3,5- 5,5mEq/l) | 3,8mEq/l |
1 milligram DST(< 1,8µg/dl) | 1,04µg/dl | ||
0,5 milligram DST(< 3µg/dl) | 0,90µg/dl |
347 - A Rare Pituitary Pathology: Patient With Crooke Cell Corticotroph Adenoma - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, EP816
Background: Micro vascular complications are the major outcome of Type 2 Diabetes Mellitus progression, which reduces the quality of life and increases diabetic morbidity & mortality. As the incidence of type 2 diabetes is growing day by day; our search for its aetiology and pathogenesis is also ever growing to predict its risk factors and early screening for better care and prevention of its complications. Many studies have tried to link susceptibility of type 2 diabetes with ABO blood group though results have been inconsistent. The present study aims to analyse association of micro vascular complication with different blood groups if any.
Methods: The study included the paitents with diabetes who were hospitalized and followed up in our clinic form Dec. 2019 to April 2022. Information such as age, sex, and family history of diabetes was scanned from medical records. The blood group was determined by standard serological methods. Screening of microvascular complications done by appropriate clinical examinations and laboratory investigations.
Results: There was 348 patients with type 2 diabetes in this study, the average age of the patients was 59.3±12.8, male to female ratio was 142(40.8%)/204 (59.8%) respectively. 246 (70.68%) patients had one or the other complications. Diabetic nephropathy, rethinopathy and neuropathy ratio was 31.3%, 35.20% ve %52.0% respectively. None of the type of micro vascular complication was found to be significantly associated with different blood groups. In addition we found that Rh (K) group had significantly low Diabetic nephropathy, rethinopathy compare to Rh (C) group (P=0.044 ve P 0.041).
Conclusions: Although we didn’t finde a relationship between ABO blood group and diabetic microvascular complications, Rh (C) was found to be a risk factor for developing nephropathy and retinopathy.
346 - Association of ABO blood groups with diabetic microvascular complications - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, EP543
Background: Micro vascular complications are the major outcome of Type 2 Diabetes Mellitus progression, which reduces the quality of life and increases diabetic morbidity & mortality. As the incidence of type 2 diabetes is growing day by day; our search for its aetiology and pathogenesis is also ever growing to predict its risk factors and early screening for better care and prevention of its complications. Many studies have tried to link susceptibility of type 2 diabetes with ABO blood group though results have been inconsistent. The present study aims to analyse association of micro vascular complication with different blood groups if any.
Methods: The study included the patients with diabetes who were hospitalized and followed up in our clinic form Dec. 2019 to April 2022. Information such as age, sex, and family history of diabetes was scanned from medical records. The blood group was determined by standard serological methods. Screening of microvascular complications done by appropriate clinical examinations and laboratory investigations.
Results: There was 348 patients with type 2 diabetes in this study, the average age of the patients was 59.3±12.8, male to female ratio was 142(40.8%)/204 (59.8%) respectively. 246 (70.68%) patients had one or the other complications. Diabetic nephropathy, rethinopathy and neuropathy ratio was 31.3%, 35.20% ve %52.0% respectively. None of the type of micro vascular complication was found to be significantly associated with different blood groups. In addition we found that Rh (K) group had significantly low Diabetic nephropathy, rethinopathy compare to Rh (C) group (P=0.044 ve P 0.041).
Conclusions: Although we didn’t finde a relationship between ABO blood group and diabetic microvascular complications, Rh (C) was found to be a risk factor for developing nephropathy and retinopathy.
345 - Metformin-Associated Lactic Acidosis: A Case Report - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, EP341
Introduction: Metformin is widely used as the first-line therapy for patients with type 2 diabetes,
and its most common adverse effects are gastrointestinal. Metformin-associated lactic acidosis (MALA) is a rare but serious adverse effect in patients with type 2 diabetes or patients who attempt suicide with metformin overdose. Here, we report the case of a 22-year-old woman who developed severe lactic acidosis after high-dose metformin was taken for a suicide attempt.
Case: A 22-year-old woman with anxiety disorder and depression developed lifethreatening lactic acidosis after taking high doses of metformin to attempt suicide. The patient received approximately 30 g of metformin. She applied to the emergency department with slurred speech and nausea. In her initial laboratory findings, arterial blood gas pH was 7.41, bicarbonate 14 mmol/l, anion gap 13 mmol/l, lactate 7.5 mmol/l, and creatinine of 1.44 mg/dl. Then she deteriorated and arterial blood gas pH became 6.96, bicarbonate 5.8 mmol/l, anion gap 33 mmol/l, lactate 23.9 mmol/l, and creatinine of 1.99 mg/dl. Renal replacement therapy was initiated. After one dialysis session, her severe acidemia resolved over time. She was discharged from the hospital without any complications. A Naranjo assessment score of 9 was obtained, indicating a probable relationship between the patient’s lactic acidosis and her use of the suspect drug.
Conclusion: MALA is a well-known and life-threatening complication of metformin. Vomiting and diarrhea are the first signs of MALA. Even if severe lactic acidosis may not be apparent at first as in our case clinicians should be aware that lactic acidosis may develop. Severe lactic acidosis can be treated with renal replacement therapy because metformin is dialysable.
344 - Ultrasonographic features of thyroid nodules and thyroid gland in obese patients - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, EP270
Objective: Thyroid nodules are one of themost common thyroid diseases. Ultrasonography is an
reliable and the most commonly used imaging method in the evaluation of thyroid nodules with a high sensitivity (Sn) and specificity (Sp). The prevelance of obesity, especially severe obesity, is increasing at an alarming rate in the worldwide. Although obesity and thyroid disorders are related to each other, the pathological relationship between those is not clear. Several studies have revealed that thyroid nodules are associated with adiposity which is assessed by body mass index (BMI). In this study we aimed to evaluate the morphological structure of the thyroid gland and thyroid nodules in obese patients according to the degree of the obesity.
Methods: 273 patients with BMI>30 kg/m2 and applied to our endocrinology outpatient clinic between 2019 and 2022 years for obesity or any other reason and also requested thyroid ultrasonography and thyroid function tests were analyzed retrospectively. The demographic data of the patients (sex, age), thyroid function tests, thyroid ultrasonography features (thyroid gland size, volume, parenchyma structure, and, if any, nodule and nodule features) and also if there is thyroid nodule cytology, were evaluated. According the body mass index patients were divided as
class I (BMI;30-34.9 kg/m2), class II (BMI; 35-39.9 kg/m2) or class III (BMI;R40 kg/m2) obesity.
Results: Total of the 273 patients, 53 (19.4%) were male, 220 (80.6%) were female. 19 (7%) , 60 (22%), and 194 (71%) of the 273 patients had class I, II, and class III obesity, respectively. Ultrasonographically, the thyroid parenchyma was heterogeneous in 221 (92.9%) of the patients. But there was no statistically significant thyroid gland heterogeneity between the groups. Anti thyroglobulin antibody positivity was significantly higher in class III obese patients (P=0.047), but no significant difference was found in antiTPO antibody positivity and thyroid function tests between obesity classes. Also there was no significant difference between obesity classes and thyroid nodule features including; echogenicity, structure, halo sign, border regularity, presence of calcification and also thyroid nodule cytology.
Conclusıon: Although we could not found a relationship between obesity classes and thyroid function tests and nodule features, most of the obese patients had parenchymal heterogeneity. Considering the increasing incidence of obesity and frequency of thyroid nodules, thyroid ultrasonography will be useful in obese patients.
343 - Comparison of biochemical values in asymptomatic and symptomatic urolithiasis - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, EP185
Background: Primary Hyperparathyroidism (PHPT) is a common endocrine disorder that is characterized by hypercalcaemia and elevated or inappropriately normal serum levels of parathyroid hormone. Most often, the presentation of PHPT is asymptomatic. PHPT can manifest with osteoporosis and hypercalciuria as well as with vertebral fractures and nephrolithiasis, both of which can be asymptomatic. Our aim in this study; to determine the frequency of kidney stones in patients operated for primary hyperparathyroidism and to compare the biochemical values of symptomatic and asymptomatic patients with kidney stones.
Methods: It was planned to include patients who had undergone parathyroidectomy, who applied to Ankara Yıldırım Beyazıt University Atatu¨rk Training and Research Hospital between December 2006 and January 2019 and to Ankara City Hospital Endocrinology and Metabolic Diseases Clinic between February 2019 and November 2021.
Results: Of 886 patients who were operated for primary hyperparathyroidism, 15.9% (n:141) were male. 189 (%21.3) patients had symptoms at the time of diagnosis. Diffuse body pain (37%), flank pain (22.2%), fatigue (11.6%), dyspepsia (6.9%), polyuria and polydipsia (4.2%) were the most common symptoms. Of the patients, 45.6% (n:388) had osteoporosis, 24.6% (n:253) had osteopenia, and 30.3% (n:257) kidney stones. Urinary symptoms were present in 133 (16.5%) patients. Genetic analysis was performed on 83 patients. 7.2% of the patients who underwent genetic analysis were men-1. The mean age of the patients was 53.6± 11.9 (18-85) years. The mean preoperative total calcium of the patients was 11.1±1.1 (6.3-18.6) mg/dl. The mean preoperative phosphorus was 2.6±0.7 (0.7-9.0) mg/dl. The mean preoperative 24-hour urinary calcium of the patients was 380.5±198.2 (24-1438) mg/24-hour. The mean preoperative 24-hour urine phosphorus was 797.9±350.4 (30.2-3798) g/24 hour. 257 patients with kidney stones were divided into two groups according to urinary symptoms. 70.2% (n:92) of 131 patients with urinary symptoms and 82.7% (n:91) of 110 patients without urinary symptoms were women. The proportion of women was significantly higher in the group without urinary symptoms (P:0.035). The median age was significantly higher in the group without urinary symptoms compared to urinary symptoms group (54.7 years vs 51.5 years, P:0.039). osteoporosis rate, total calcium value, phosphorus value, parathormone value, 24-hour urinary calcium and 24-hour urine phosphorus value were similar for the two groups.
Conclusion: Patients with symptomatic nephrolithiasis were younger and more male dominated.
342 - Pheochromocytoma associated with von Hippel-lindau disease - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, EP116
Von Hippel-Lindau (VHL) syndrome is a pathological condition that causes various clinical symptoms and is difficult to diagnose. The most common pathological lesions are hemangioblastomas of the central nervous system, retinal angiomas, renal clear cell carcinomas, and pheochromocytomas. Here we report a case of likely to be VHL due to his family history.
Case: A 33-year-old male suffering from hypertension and a history of hemangioblastoma operated in 2019. The patient had an endoscopic examination after developing nausea, vomiting and weight loss. His endoscopic biopsies include grade 2 neuroendocrine tumors (NET). The patient refer to endocrinologist. The father of the patient died at age of 40 due to brain tumor and his brather was operated due to retinal and cerebral hemangioblastoma (in 2013) since that date the familyhad been followed up in the department of neurosurgery with suspicion of VHL. His plasma free metanephrines and urinary metanephrines was high and a computer tomography scan, MIBG and MRI scan of the abdomen showed a solid mass in the lower pole of the lenf kidney at 2.5X2 cm, pancreatic cysts and right adrenal mass at 36X40 laparascopic adrenalectomy and parsiel nefrectomy was performed. The Pathological examination revealed renal cell carcinoma and pheochromocytomas with a low PASS score. The contro plasma free metanephrines and urinary metanephrines were withen normal range.
Conclution: Since pheochromocytomas can have low activity, the classical symptoms may be missing. The absence of symptoms can make it difficult to diagnose pheochromocytoma and Even if we couldn’t perform the genetic examination there is a strong association between pheochromocytoma and VHL syndrome, and pheochromocytoma is an important feature in the clinical classification of VHL syndrome. The family history of retinal or central nervous system hemangioblastoma (Hb) exists, only one Hb or visceral lesion (renal tumours, pancreatic cysts or tumours, pheochromocytoma, papillary cystadenomas of the epididymis) is required to make the diagnosis of VHL and Due to the risk of pheochromocytoma, the radyologıc sxanning and biochemical tests shoud performed.
341 - Nivolumab-induced hypothyroidism: a case report - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, P795
Introduction: Immune checkpoint inhibitors are relatively new and promising treatments for a variety of solid tumors. Nivolumab is an anti-cancer monoclonal antibody that inhibits anti-programmed death-1 (PD1) and modulates T-cell response. It has been shown to significantly improve survival in many types of cancer, but clinical studies have also reported an increased risk of developing immune-related adverse events. In particular, immune-related adverse events may be related to the endocrine system. It has been reported that approximately 8% of patients treated with PD-1 inhibitors demonstrate hypothyroidism. We present a case of thyroid dysfunction caused by nivolumab.
Case: A 64-year-old male patient was treated with nivolumab for 10 months for tonsillar squamous cell carcinoma. He had no history of thyroid disease. Laboratory studies performed before the administration of nivolumab revealed normal thyroid function with normal levels of anti-thyroid peroxidase and antithyroglobulin antibodies. 9 months after starting treatment, the patient’s thyroid
stimulating hormone (TSH) levels suddenly increased to 57.70 mU/l (normal range 0.55-4.78 mU/l). Free T3 level was 1.65 pg/l (normal range 2.3 - 4.2 pg/l) and free T4 level was 0.24 ng/dl (normal range 0.89-1.76 ng/dl). We suspected nivolumab-induced hypothyroidism in the absence of other possible causes and started thyroid hormone replacement. The patient was followed as euthyroid with L-thyroxine 100 mg/day.
Conclusions: Immunotherapy has demonstrated significant clinical efficacy in many types of cancer. Immune checkpoint inhibitors aim to stimulate the immune system against cancer cells but should not be considered independent of some side effects. Thyroid dysfunction should be considered as a possible immune-related adverse event. Therefore, it is important to evaluate thyroid dysfunction at baseline and before the administration of each dose of nivolumab.
340 - Rapidly-Growing Thyroid Mass: is the Diagnosis Always Anaplastic Cancer? - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, P777
A 87 year old woman admitted with complaints of hoarseness and a palpable mass which she noticed 1 week ago. She had hypothyroidism for 25 years. On examination, there was a hard and fixed palpable 4x4 cm mass on the right side of the neck. In laboratory evaluation, thyroid function tests were normal, thyroid auto-antibodies were positive, calcitonin was normal, C-reactive protein was 224 mg/l and liver and kidney function tests were normal. Thyroid ultrasonography revealed a 27.5x51.1x61.0mm isoechoic nodule containing macrocalcifications and areas of cystic degeneration completely filling the right lobe. Fine needle aspiration biopsy(FNAB) of the nodule was reported as atypia of undetermined significance. In the second FNAB;there were atypical cells with spindle cytoplasm, isolated spindle cells described in fibrin in the cell block with necrosis. The specimen was evaluated as suspicious for malignancy. Lymphoid malignancies were ruled out with flow cytometric analysis. The patient was hospitalized with a prediagnosis of anaplastic thyroid cancer. Neck MRI detected a 9.0x6.5x6.5 cm centrally necrotized mass surrounding right common carotid artery. In 18-FDG-PET-CT scanning, uptake of the lesion was significantly increased and there were multiple metastatic nodules in the lung. A tru-cut biopsy was performed. ‘In cytopathologic evaluation, neoplastic infiltration consisting of fascicular shapes was observed within a fibrous stroma. Spindle cells arranged in ‘herringbone pattern was observed. A large number of mitotic figures drew attention. In the immunohistochemical study, no staining was detected with TTF-1, CD34, PAX-8, CK-7, p63, SMA, desmin, FL-1, S100, synaptophysin and calcitonin. Staining with vimentin was detected. The Ki-67 proliferation index was 90%. BRAF mutation was negative.’ A primary malignant fibrosarcoma of thyroid gland was considered. Because of the advanced age and poor general performance of the patient; chemotherapy and surgery were not considered. 10 sessions of radiotherapy was started. Malignant mesenchymal tumors of thyroid gland comprise 0.3% of all malignant thyroid tumours(1). Fibrosarcomas consist 9.2% of primary malignant mesenchymal tumors of thyroid(2). Although the initial diagnosis that comes to mind in a hard, fixed and rapidly-growing thyroid cancer is anaplastic cancer, malignant mesenchymal tumors like fibrosarcoma should also be considered in differential diagnosis.
References
1. Bula G, Waler J, Niemiec A, Trompeta J, Steplewska K, Gawrychowski J. Unusual malignant thyroid tumours�"a clinical study of 20 cases. Acta Chirurgica Belgica 2008; 108: 702-07.
2. Surov A, Gottschling S, Wienke A, Meyer HJ, Spielmann RP, Dralle H. Primary thyroid sarcoma: a systematic review. Anticancer research. 2015;35(10):5185-91
339 - Does timing of repeat fine needle aspiration biopsy in thyroid nodules alter the adequate or AUS/FLUS cytology result? - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, P773
Aim: To determine whether early repeat fine needle aspiration biopsy(FNAB) has an effect on adequate or atypia of undetermined significance/follicular lesion of undetermined significance(AUS/FLUS) cytology rates in thyroid nodules with inadequate or AUS/FLUS in the first FNAB.
Method: Nodules of patients who underwent repeat biopsy due to insufficient or AUS/FLUS cytology between 2019-2022 were included. Demographic data of the patients and ultrasonographic, cytological and histopathological results of the nodules were recorded. Additionally, the time between the two biopsies was noted. In nodules with two FNAB results, the first was called initial, and the second was called rebiopsy. In nodules with more than two FNAB results, the time between each consecutive results was evaluated separately, and for these nodules, again first result was called initial and the second was called rebiopsy for each biopsy period of the nodule. Seven different paired groups were formed according to the time between two consecutive biopsies;before and after 1 month,45 days,2 months,3 months,6 months,9 months,12 months. The groups were compared in terms of adequate or AUS/FLUS cytological results.
Results: 972 nodules of 546 patients who underwent FNAB at least twice were included. The mean age of the patients was 51±12, and the female sex ratio was 79.1% (n=432). FNAB was performed 2 times for 573,3 times for 310, 4 times for 73, 5 times for 13 and 6 times for 3 of the nodules. A total of 2984 cytology results were evaluated. Accordingly,1026 (68.8%) of the initial biopsies were inadequate and 466 (31.2%) were AUS/FLUS. Rebiopsy results are shown in the table. There were no differences in adequate or AUS/FLUS rebiopsy results according to the different time interval groups(P>0.05 for all). When 1026 samples with inadequate initial FNAB were considered as a separate group, to perform rebiopsy before or after any time interval had no effect on adequate or AUS/FLUS results. Similar results were obtained when a subgroup was created for samples with initial AUS/FLUS cytology(P>0.05 for all). Also, there was no cut-off time for an adequate or AUS/FLUS rebiopsy result.
Conclusions: In patients with inadequate or AUS/FLUS initial biopsy, the rate of adequate or AUS/FLUS cytology results at rebiopsy did not vary with the timing of repeat biopsy. As recommended in the ATA guideline, there is no need to wait 3 months for a repeat biopsy. In patients with suspicious nodules in terms of malignancy, biopsy might be repeated before 1 month.
Table 1 Comparison of the parameters after patients with polycystic ovary syndrome excluded
Rebiopsy | Initial Biopsy | p | ||
Inadequate | AUS/FLUS | Total | <0.001 | |
Nondiagnostic | 393(38.3%) | 168(36.1%) | 561(37.6%) | |
Benign | 458(44.6%) | 148(31.8%) | 606(40.6%) | |
AUS/FLUS | 171(16.7%) | 135(29.0%) | 306(20.5%) | |
FN/SFN | 0(0.0%) | 4(0.9%) | 4(0.3%) | |
SFM | 1(0.1%) | 4(0.9%) | 5(0.3%) | |
Malignant | 3(0.3%) | 7(1.5%) | 10(0.7%) | |
Total | 1026 | 466 | 1492 |
338 - Predictive factors for sufficient cytological result after first nondiagnostic thyroid fine-needle aspiration biopsy result - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, P772
Aim: To determine whether there is any factor that can predict sufficient results in second thyroid fine-needle aspiration biopsy (FNAB) after first nondiagnostic cytological result.
Materials and method: Nodules with non-diagnostic result after first FNAB were included and separated into two groups as sufficient (Group-1) and insufficient (Group-2) second FNAB.
Results: Second FNAB was performed on 643 nodules of 443 patients with initial nondiagnostic cytology. The result was diagnostic in 437(68.0%) nodules (Group1) while it was again nondiagnostic in 206 (32.0%) (Group-2). Thyroid autoantibody positivity were similar in groups. Cystic/mixed structure and heterogeneous echogenity were more frequent in Group-2 (P=0.020 and P=0.011, respectively). Solid structure and isoechoic appearence were more frequent in Group-1 (P=0.003 and P=0.020, respectively). Border regularity, micro/macrocalcification, taller-than-wide shape, presence of halo were comparable in two groups (P>0.05). There were also no significant differences in terms of nodule dimensions, volume and rate of subcentimeter nodule between two groups(P>0.05). In multivariate analysis, likelihood of sufficient cytology was 1.943 times higher in isoechoic nodules in comparison to heterogeneous nodules (95 CI:1.253-2.977, P=0.003), whereas the effect of nodule structure on sufficient result became insignificant (P=0.432). Sufficient results group were cytologically distributed as 299 (68.4%) benign, 131 (30.0%) AUS/FLUS, 2 (0.5%) FN/SFN, 1 (0.2%) SFM and 4 (0.9%) malignant. 35 patients in Group-1 and 20 patients in Group-2 underwent thyroidectomy. Malignant histopathology was observed in 12/60(20%) nodules in Group-1 and in 3/37(8.1%) nodules in Group-2 (P=0.116)(Table).
Conclusions: Heterogeneous echogenity and cystic/mixt structure were more frequent in insufficient group, but after multivariate analysis, only isoechoic texture was determined to predict sufficient cytological result in rebiopsy. Second biopsy should be done to all nondiagnostic nodules because of comparable malignant histopathology results.
Sufficient result after nondiagnostic biopsy (n=437, 68.0%) | Insufficient result after nondiagnostic biopsy (n=206, 32.0%) | p | |
AntiTPO positivity (n=606) | 85 (20.6%) | 28 (14.5%) | 0.074 |
Anti-TG positivity (n=600) | 89 (21.8%) | 33 (17.3%) | 0.204 |
Subcentimeter nodule | 35 (8.0%) | 18 (8.8%) | 0.747 |
Taller-than-wider | 51 (11.7%) | 15 (7.3%) | 0.085 |
Irregular border (n=304) | 188 (89.5%) | 77 (81.9%) | 0.067 |
Echogenity (n=587) | 0.005 | ||
Isoechoic | 314 (77.3%) | 118 (64.5%) | 0.001 |
Hypoechoic | 26 (6.4%) | 18 (9.8%) | 0.143 |
Heterogenous | 66 (16.3%) | 47 (25.7%) | 0.0071 |
Nodule texture | 0.038 | ||
solid | 404 (92.4%) | 180 (87.4%) | |
cystic/mixt | 33 (7.6%) | 26 (12.6%) | |
Microcalcification | 26 (5.9%) | 8 (3.9%) | 0.275 |
Macrocalcification | 36 (8.2%) | 21 (10.2%) | 0.415 |
Presence of halo | 72 (16.5%) | 26 (12.6%) | 0.204 |
Histopathology, malignant (n=97) | 12 (20.0%) | 3 (8.1%) | 0.116 |
Nodule Dimensions (mm, median (IQR)) | |||
Anteroposterior | 8.8 (7.0-12.6) | 9.1 (6.8-12.8) | 0.780 |
Lateral | 11.9 (9.5-16.2) | 11.8 (9.3-16.6) | 0.948 |
Longitudinal | 13.1 (10.9-19.4) | 13.6 (10.7-19.1) | 0.804 |
Nodule Volume (cm3, median (IQR)) | 0.71 (0.39-2.03) | 0.69 (0.37-1.91 | 0.993 |
IQR:interquartile range
337 - Selective Arterial Calcium Stimulation Test In Two Cases With Occult Insulinoma - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, P396
Introduction: Insulinoma is a rare neuroendocrine tumor that is difficult to diagnose due to its obscure location. Conventional radiographic methods have low sensitivity and are inadequate to detect insulinoma. Selective arterial calcium stimulation test (SACST) is 95-100% sensitive in the diagnosis of insulinomas. Here, we presented two cases of insulinoma that could not be located by radiographic methods and evaluated them with SACST.
Case 1: A 48-year- old woman who had dizziness was referred to our endocrine clinic with a suspicion of insulinoma. A 72-hour fasting test was performed to establish a diagnosis of endogenous hyperinsulinemia. After 19 h hypoglycemic symptoms emerged and fasting serum glucose (FSG) was 27 mg/dl, insulin 6,5 mU/l, and C-peptide 2 mg/l. MRI of the abdomen, Galium-68 Dotatate scintigraphy, and endoscopic ultrasonography (EUS) failed to detect the tumor. SACST was performed to localize the tumor. Calcium injection of the gastroduodenal artery caused a more than 11-fold increase in hepatic insulin above baseline indicating a lesion in the head region of the pancreas. Intraoperative ultrasonography of the pancreas revealed a 1 cm nodular lesion in the head. Proximal pancreatectomy was performed. Histopathological findings were consistent with well-differentiated neuroendocrine tumor showing positive staining with synaptophysin and chromogranin. After surgery, the patient was free of all previous symptoms.
Case 2: A 67-year- old woman was admitted to the clinic due to dizziness and diaphoresis. She applied to the emergency department once with a loss of consciousness. There was a weight gain of 4-5 kg during this period. After 12 h of the 72-hour fasting test, hypoglycemic symptoms emerged, and FSG was 36 mg/dl, insulin 6,9 mU/l, and C-peptide 1,7 mg/l. MRI of the abdomen, Galium-68 Dotatate scintigraphy, and EUS failed to demonstrate the tumor. SACST was performed and calcium injection of the splenic artery caused a more than 9-fold increase in hepatic insulin above baseline which was suggestive of an insulinoma lesion in the tail of the pancreas. Intraoperative ultrasonography of the pancreas revealed a 1 cm nodular lesion in the tail. Distal pancreatectomy was performed. No hypoglycemia has occurred since the surgery.
Conclusions: The localization of insulinoma is critical for curative surgery and might be problematic. Because of the low sensitivity of non-invasive imaging procedures in tumors smaller than 2 cm, invasive methods can be used for the localization like in our cases.
336 - How well are guidelines followed in the follow-up of hypoparathyroid patients? - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, P586
Background: Hypoparathyroidism (HypoPT) is a rare condition that is characterized by hypocalcemia and hyperphosphatemia due to low or inappropriately normal serum levels of parathyroid hormone (PTH) for at least 6 months. The long-term complications of hypoparathyroidism indicate the necessity of screening them. In the follow-up of these patients according to hypoparathyroidism guidelines is recommended; calcium, phosphorus, albumin, magnesium, creatinine, and eGFR levels should be checked annually or more frequently than clinical status. A 24-hour urine calcium excretion is recommended once a year. Renal imaging is recommended in patients with elevated creatinine or high urinary calcium excretion, or patients suggesting renal stones. For basal ganglia calcification, brain MRI or CT is advised. A yearly eye examination is recommended for cataracts. In our study, in the long-term follow-up of hypoparathyroidism patients, it was examined whether the guidelines were followed.
Methods: Between February 2019 and September 2021, patients aged ≥18 years with hypoparathyroidism who were followed by the routine scheduled monitoring visit at the outpatient clinic of the endocrine and had their data retrospectively documented. Comorbidities, imaging, and hormonal tests and results of these patients were evaluated.
Results: Among the 264 patients, the mean age was 49.34±12.98 (22-91). 211 (79.9%) of the participants were female. All patients’ had blood biochemistry tests. Of the patients, 3% had eye examinations, 9.8% had brain imaging, 18.6% had renal imaging, 11 % had 24 h urinary Ca results. Cataract was observed in 2 (0.8%), basal ganglia calcification was observed in 4 patients (1.5%). Nephrocalcinosis or nephrolithiasis was observed in 2 patients (0.8%). Hypercalciuria was defined as a 24 h urine calcium excretion >300 mg/24 h and was observed in 8 of participants with hypoparathyroidism. (Table 1)
Table 1 Hypoparathyroidism complications screening
| Total (n=264) |
Eye secreening | 8 (3) |
Normal | 5 (1.9) |
Cataract | 2 (0.8) |
Glaucoma | 1 (0.3) |
Brain imaging | 26 (9.8) |
Normal | 22 (8.3) |
Calcification | 4 (1.5) |
Renal imaging | 49 (18.6) |
Normal | 47 (17.8) |
Renal stone | 2 (0.8) |
24 h Urinary Ca | 29 (11) |
24 h Urine Ca normal (<300 mg/24 h) | 21 |
24 h Urine Ca elevated(>300 mg/24 h) | 8 |
335 - Graves’ Disease in A Patient with Thyroid Hormone Resistance - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, P485
Introduction: While Graves’ disease is a common cause of thyrotoxicosis, tyroid hormone resistance (THR) is a rare cause of high thyroid hormones. Coexistence of Graves’ disease and THR which can cause quite a lot of difficulties in diagnosis and treatment was reported very rarely in the literature. Here, we report a patient with THR and Graves’ disease in whom remission was achieved with medical therapy.
Case: A 38-year-old woman applied to our clinic with sweating and palpitation. Familial history revealed THR in her sister. Her body temperature was 37.2°C, heart rate was 120 beats/minute, respiratory rate was 18 breaths/minute and blood pressure was 120/70 mmHg. In laboratory examinations, thyroid stimulating hormone (TSH) was 0.018 mU/l (0.55-4.78 mU/l), free T4 was 2.64 ng/dl (0.89- 1.7 ng/dl), free T3 was 9.05 ng/l (2.3-4.2 ng/l), anti-thyroglobulin and anti-thyroid peroxidase were negative, TSH receptor antibody (TRAB) was positive. Thyroid ultrasonography revealed chronic thyroiditis and technetium 99m scintigraphy showed heterogeneous activity. When laboratory results were examined retrospectively, we saw that in previous 3 years, her TSH, free T4 and free T3 ranged between 0.84-1.75 mU/l, 1.87-2.12 ng/dl and 4.77-5.86 ng/l, respectively. Thus, the patient had the lowest TSH value and highest free thyroid hormones in her life when she applied. With the current laboratory results and imaging findings, Graves’ disease was diagnosed. Methimazole and propranolol treatment was started. Methimazole was switched to propylthiouracil due to the development of skin rash. Owing to family history and her previous thyroid hormone profile, THRB gene mutation analysis was requested from the patient. Heterozygous c.1001T>C mutation was detected. Under treatment, her symptoms resolved, TSH returned to normal, free T3 and T4 were followed as close to the upper limit or slightly elevated. The patient’s propylthiouracil medication therapy was discontinued after 18 months. At the time of discontinuation her TSH was 0.96 mU/l, free T3 was 6.05 ng/l, free T4 was 1.98 ng/dl, TRAB was negative. At the last visit, 2 years had passed since drug discontinuation and her serum TSH was 0.51 mU/l, free T3 was 4.86 ng/l and free T4 was 1,50 ng/dl.
Discussion: Treatment with anti-thyroid drugs remains the primary choice for Graves’ hyperthyroidism complicated by THR. The optimal treatment is to normalize TSH while keeping free thyroid hormones slightly higher than the upper limit. Iodine therapy and surgery are not generally recommended, since they may induce severe hypothyroidism
334 - Evaluation of Breast Calcification, Calcification Characteristics and BI-RADS (Breast Imaging-Reporting and Data System) Categories in Patients with Primary Hyperparathyroidism - 2023
Uluslararası Bildiriler 25th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, P302
Aim: It is hypotethically thought that increased frequency of breast cancer in patients with primary hyperparathyroidism (PHPT)may be due to the fact that calcium accumulation in the breast may be higher in patients with PHPT giving rise to more breast-related examinations. Although there are many studies or case reports showing calcification in many organs and tissues, in PHPT, there is not any study investigating breast calcification in these patients in the literature. We aimed to determine the frequency and features of breast calcification and distribution of BIRADS scores in patients with PHPT.
Method: Female patients ≥40 years old with PHPT and and age-matched healthy women were included. Demographical, antropometric and laboratory findings were noted. Mammography was performed in all patients and controls. Calcification types and BIRADS scores were recorded. Clustered microcalcification, ductal calcification, linear thin or segmental calcification were considered suspicious calcification. Skin calcification, scattered, punctate, vascular calcification and macrocalcification were termed as benign calcification. Two groups were compared in terms of demographical, laboratory findings, presence of calcification, calcification types and BI-RADS in mammography. Patients were divided in two groups according to the duration of PHPT as less or more than 48 months.
Results: Sixty-one patients and 75 control were enrolled. While age distribution was similar(57.0±7.9 vs 55±7.5, P=0.153), body mass index was higher in patient group (32.4±6.7 vs 29.2±6.2 kg/m2 , P=0.005). Median duration of PHPT was 46 (1-85) months. BI-RADS score was comparable and the most frequent score was BIRADS-0. Presence of breast calcification and calcification types were not different in two groups. Demographical, laboratory and mammographic findings are summarized in table. Presence of calcification was similar in PHPT patients with disease duration of less and more than 48 months. There was not any cut-off for disease duration that can predict presence of calcification. Of the 3 patients (all was with PHPT) who underwent excisional breast biopsy, one resulted in invasive breast ca, one as atypical ductal hyperplasia, and the other as benign.
Conclusion: Female patients with PHPT did not have an increased incidence of breast calcification compared to healthy women, suggesting that calcification is not responsible for the increased incidence of breast cancer in these patients. Distribution of BI-RADS scores was also not affected by the presence of PHPT.
PHPT (n=61, 44.9%) | Control (n=75, 55.1%) | p | |
Age | 57.0±7.9 | 55±7.5 | 0.153 |
BI-RADS | |||
0 | 48 (77.7%) | 58 (77.3%) | 0.603 |
1 | 2 (3.3% ) | 4 (5.3%) | |
2 | 9 (14.8%) | 12 (16.0%) | |
3 | 1 (1.6%) | 0 (0.0%) | |
4A | 1 (1.6%) | 0 (0.0%) | |
4B | 0 (0.0%) | 0 (0.0%) | |
4C | 0 (0.0%) | 1 (1.3%) | |
Breast calcification | 33 (54.1%) | 42 (56.0%) | 0.739 |
Benign calcification | 30 (49.2%) | 40 (53.3%) | |
Suspicious calcification | 3 (4.9%) | 2 (2.7%) | |
No calcification | 28 (45.9%) | 33 (44.0%) | |
|
333 - The Relationship Between Autonomic Cortisol Secretion and Metabolic Diseases in Cases with Adrenal Incidentaloma - 2023
Uluslararası Bildiriler 5th European Congress of Endocrinology, 13-16 May 2023, Istanbul, Turkey, Endocrine Abstracts May 2023, Vol 90, P562
Background: Adrenal incidentalomas (AI) are lesions discovered incidentally on imaging without clinical symptoms or examination findings. AI can produce hormones in 5-30% of cases. Autonomic cortisol secretion (ACS) is the most common of these. Although ACS is asymptomatic, it increases the risk of metabolic disorders.
Methods: Patients aged ≥18 years with adrenal adenoma and upper abdominal MRI who presented and were examined in the endocrinology outpatient clinic, had their data retrospectively documented. Comorbidities, examinations and hormonal tests and results of these patients were evaluated. Those who failed dexamethasone suppression tests (cortisol >1.8 g/dl) and did not have Cushing’s syndrome were classified as ACS.
Results: Among the 465 patients, 311 (66.9%) were women with a mean age of 54.8±10.2 (18-82). Of the patients, 31.4% had diabetes mellitus (DM), 53.8% had hypertension (HT), 30.8% had hyperlipidemia (HL), 11.8% had coronary artery disease (CAD), 1.3% had heart failure (HF) and. Hormone testing revealed that 31 (6.6%) of the patients had primary aldosteronism, 7 (1.5%) had pheochromocytoma, and 75 (16.1%) had ACS. Patients with and without ACS were compared for the presence of other additional diseases and adenoma size (Table-1). DM, HT and HL were higher in the ACS group (P<0.05, for each). Adenoma size was larger in the ACS group (P<0.05). Although the gender distribution was similar in both groups (P>0.05), the OCS patient was older (P=0.006).
Conclusion: Individuals with large adenomas are more likely to have ACS. Large adrenal adenomas should be monitored for ACS and associated cardiometabolic risks, as well as necessary treatments.
Table 1. Comparison of patient characteristics with and without autonomic cortisol secretion
Autonomic cortisol secretion | Yes n=75 | No n=390 | p |
Sex, Woman/Man | 56/19 | 255/135 | 0.11 |
Age (years), mean | 57.8±10.8 | 54.2±9.9 | 0.006 |
Size of adenoma (mm), median (min-max) | 25 (10-54) | 18 (10-60) | <0.001 |
T2DM % | 41.3 | 29.5 | 0.04 |
HT % | 69.3 | 50.8 | 0.003 |
HL % | 41.3 | 28.7 | 0.03 |
CAD % | 18.7 | 10.5 | 0. 04 |
HF % | 2.7 | 1 | 0.25 |
Osteoporosis % | 31.8 | 35 | 0.95 |
T2DM type 2 diabetes mellitus, HT hypertension, HL hyperlipidemia, CAD coronary artery disease, HF heart failure
332 - Persistent Mullerian duct syndrome: An atypical clinical presentation - 2022
Uluslararası Bildiriler Endobridge 2022, 20-23 October 2022, Antalya, Turkey.
Background: Persistent Müllerian duct syndrome(PMDS) is a rare sexual development disorder characterized by a normal male phenotype.Müllerian structures cannot regress due to the absence of anti-müllerian hormone(AMH) or resistance to AMH receptor. In addition to male internal genitalia, female reproductive organs, including the uterus, uterine tubes, and upper 1/3 of the vagina are also detected. We will present a patient with PMDS who presented with bilateral cryptorchidism.
Case: A 31-year-old single man was referred to our clinic because of bilateral undescended testes and a rudimentary uterus detected during the evaluation of the lower abdominal pain.
On physical examination, his body mass index(BMI) was 21.2. His arm span was 170 cm, and his upper-lower segment ratio was 0.96. Beard, axilla, and pubic hair development were normal; however, testes were not in the scrotum bilaterally.His karyotype analysis was 46XY.
His prenatal, natal, and postnatal histories were not remarkable. His parents were not consanguineous; the younger brother had a history of undescended testis operation at age one.
In laboratory examination, blood glucose, renal and liver functions were normal. Androstenedione, DHEAS, total and free testosterone, FSH, LH, total-hCG, AFP were normal. AMH>9µg/L. In the spermiogram, no sperm was observed.
A rudimentary uterus and proximal vagina were observed in the abdominal computed tomography (CT). Symmetric solid masses measuring 55x40 mm compatible with bilateral undescended testis were detected in the ovarian lodges. The mass extended to the inguinal canal on the left and the scrotum on the right. In association with these masses, there were also tubular structures with the biggest diameter of 16 mm on the right and 13 mm on the left. Prostate sizes were normal. Seminal vesicles were not observed.
PMDS was considered owing to 46 XY karyotypes, normal testosterone level, normal sexual development, external genitalia findings, accompanying Mullerian structures, and a high level of AMH. AMH gene mutation was not detected. However, AMH receptor type 2(AMHR2) gene mutation could not be studied. Bilateral undescended testicles, uterus, uterine tubes, and the tubular structures in the abdomen were excised. Classical type seminoma with lymphovascular invasion was detected in the right-side tubular structure. Tumor-negative testicular tissue was frozen for possible fertility in the future.
The patient received one cycle of Carboplatin. No metastasis was detected in the post-operative PET-CT scan. In post-operative evaluation, FSH, LH levels were high, total and free testosterone levels were low. AMH < 0.01 µg/L.The patient was started on testosterone replacement therapy.
Conclusion: PMDS is a rare cause of male pseudohermaphroditism. Malignant degeneration and infertility are two critical points in terms of treatment. Early diagnosis with increased awareness is essential in preserving fertility and preventing malignant degeneration.
331 - The relationship between free thyroid hormones and diabetic retinopathy in euthyroid patients with type 2 diabetes mellitus - 2022
Uluslararası Bildiriler 24th European Congress of Endocrinology, 21-24 May 2022, Milan, Italy, Endocrine Abstracts (2022), Vol 81, EP1188
Introduction:
The prevalence of diabetes mellitus (DM) continues to increase worldwide. Diabetic retinopathy (DRP) is one of the most common complications of Type 2 DM. Recently, the effect of thyroid hormones on diabetic microvascular complications has gained much attention. This relationship is explained by the important effects of thyroid hormones on endothelial function. There are studies
investigating the relationship between TSH and diabetic nephropathy and DRP. There are very few studies evaluating free thyroid hormone levels. In this study, it was aimed to investigate the relationship between free thyroid hormone levels and DRP in euthyroid patients with type 2 DM.
Method:
In this study, the biochemical records of patients with Type 2 DM who had euthyroid status and evaluated for retinopathy, applied to the endocrinology and ophtalmology clinics of our hospital between January 2018 and August 2018. Demographic data of the patients and characteristics that may be associated with diabetic retinopathy were evaluated. Whether the patients had DRP and, if any, retinopathy levels were recorded. It was evaluated whether there was a difference in free thyroid hormone levels between the groups with and without DRP.
Results:
A total of 171 patients, 106 men and 65 women, were included in the study.Mean age was 57.19 ±10.81 years. DRP was not present in 127 patients (74.2%), nevertheless 36 patients (21%) had nonproliferative DRP and 8 patients (4.6%) had proliferative DRP. There was no difference between the groups in terms of age, gender, hypertension, cardiovascular disease, fasting plasma glucose, serum creatinine, lipid levels and microalbuminuria. The duration of diabetes was longer
in the nonproliferative DRP group (P=0.026). HbA1c levels were higher in the proliferative DRP group (P=0.05). No significant difference was found in terms of TSH levels and free thyroid hormone levels in all three groups.
Conclusion:
In our study, the relationship between free thyroid hormone levels and DRP in euthyroid type 2 DM patients was investigated. Diabetes duration and Hba1c levels were found to be risk factors in DRP similar to the literature. When the groups with and without DRP were compared, no difference was found in TSH and free T4 and free T3 levels.
330 - A patient with acromegalic heart disease - 2022
Uluslararası Bildiriler 24th European Congress of Endocrinology, 21-24 May 2022, Milan, Italy, Endocrine Abstracts (2022), Vol 81, P770
A 36 years of old patient was admitted to the intensive care unit of cardiology when he experienced palpitations and orthopnea. The patient’s complaints started about 2 years ago as syncope and sudden shortness of breath. Thorax CT showed pleural effusion and increased cardiothoracic index. Findings on ECHO were : Ejection fraction 35%, severe mitral regurgitation and global hypokinesia. Coronary angiogram showed a fibrocalcific plaque noted in in the distal LAD. The patient was started on Furossemide, spironolactone, isosorbide mononitrate. Despite the treatment, the patient’s complaints gradually increased and over the course of the next 24 months, the patient was repeatedly hospitalised due to heart failure, and his medication was adjusted several times. Two years later, the patient was admitted to our center with the diagnosis of acute heart failure. A decrease in ejection fraction was detected in the new echocardiography (%10), and no further clinical improvement was seen, the decision was then taken to initiate treatment with levosimendan and noroadrenaline. Dilated cardiomyopathy was observed with cardiac MRI. He was consulted to the endocrine department because of suspected acromegaly. When he was evaluated, he complained of shortness of breath, arthralgia and increasing shoe size. Physical examination was positive for acral growth, nose widening, and prognathism. GH and IGF-1 levels were increased at diagnosis (table 1), the baseline and peak GH concentrations were 8.74 and 34.4 ng/ml during 75-g OGTT, showing paradoxical increases in GH (table 2). Pituitary MRI showed a non-invasive, intrasellar, macroadenoma (fig1). The diagnosis made was: Acromegaly due to growth hormone secreting pituitary macroadenoma leading to dilated cardiomyopathy. His family history was negative, but due to his young age and aggressive clinical course, the patient was screened for AIP gene mutation; a germline AIP mutation was not identified. TSS was scheduled, and primary medical treatment with sandostatin lar 20 to improve the patient’s condition. However, the patient developed cardiogenic shock and unfortunately before surgery and before assessment of response to therapy.
Table 1
Hba1c (%) | 6.4 |
P (mg/dl) (2.4-5.1) | 5.3 |
Cortisol (µg/dl) | 10.6 |
ACTH (pg/ml) (Sabah 07:00-09:00 <46) | 50.2 |
Testosterone (ng/dl) (164-783) | 130 |
FSH (mIU/ml) | 6.4 |
LH (mIU/ml) | 5.6 |
PRL (ng/ml) | 17.7 |
GH (ng/ml) (0.05-3) | 25 |
IGF-1 (ng/ml) (75-212) | 359 |
Table 2
Minute | 0. | 30. | 60. | 90. | 120. |
Glucose | 80 | 112 | 162 | 198 | 173 |
GH | 8,74 | 10,4 | 34,4 | 20,9 | 14,3 |

329 - Parathormone washout in cytology of Suspicious for Follicular Neoplasm - 2022
Uluslararası Bildiriler 24th European Congress of Endocrinology, 21-24 May 2022, Milan, Italy, Endocrine Abstracts (2022), Vol 81, P515
Introduction:
The risk of malignancy in thyroid nodules is reported by the Bethesda system by performing fine needle aspiration biopsy (FNAB). Atypia of undetermined significance (AUS) or follicular lesion of undetermined significance (FLUS) (Bethesda 3) and suspicious for a follicular neoplasm (Bethesda 4) create uncertainty about treatment and follow-up. Molecular tests, ultrasonographic features of the nodules, and calcitonin level help us for this uncertainty. Here, we will present a patient whose FNAB cytology was Bethesda 3 and Bethesda 4.
Case:
A 53-year-old female patient was admitted to our outpatient clinic after detecting a thyroid in neck ultrasound. She had familial Mediterranean fever, osteoporosis, and renal transplantation (5 years ago). In addition, the patient stated that she had been operated on the parathyroid gland while she was receiving dialysis treatment. There was no document related to parathyroid surgery. In laboratory tests, thyroid function tests, calcitonin, calcium levels were normal. 25-OH vitamin D, parathormone level, creatinine, eGFR were 14 ng/ml, 152 pg/ml, 1.51 mg/dl, 39 ml/minute respectively. Secondary hyperparathyroidism due to vitamin D deficiency was considered. On thyroid ultrasound, a hypoechoic nodule that containing cystic degeneration areas was observed adjacent to inferior carotid artery in the right lobe. The dimensions of nodule were 9.7x11.4x13.7 mm. FNAB was reported as Bethesda 3. The second FNAB cytology was also reported as Bethesda 4.Molecular testing could not be performed in our hospital. The microscopy of FNAB revealed “some of the cells were small, round, monotonous nuclei with pale cyanophilic cytoplasm with unclear borders”.No uptake suggestive of parathyroid lesion was observed in parathyroid scintigraphy. Third FNAB cytology was nondiagnostic; Parathormone washout was 525 pg/ml. Due to the high suspicion of parathyroid lesion, fourth FNAB and diluted PTH washout were performed. Fourth FNAB cytology was Bethesda 3, diluted parathormone level was 103871 pg/ml. The lesion was evaluated as intrathyroidal lesion (adenoma or parathyroid seeding due to surgery). Follow-up was planned for the patient.
Conclusion:
In parathyroid lesions evaluated as thyroid nodules, FNAB cytology and microscopy give us an idea in terms of intrathyroidal parathyroid lesion. Parathyroid scintigraphy also does not always show uptake. In this situation, PTH washout can be done. If the ultrason features, FNAB microscopy and PTH washout are inconsistent, diluted PTH washout may provide accurate results due to possible hook effect. In addition, intrathyroidal parathyroid seeding should also be kept in mind in patients who have undergone parathyroid surgery for tertiary hyperparathyroidism.
328 - Superior vena cava syndrome associated with graves’ disease - 2022
Uluslararası Bildiriler 24th European Congress of Endocrinology, 21-24 May 2022, Milan, Italy, Endocrine Abstracts (2022), Vol 81, P514
Introduction:
Goiter means that the thyroid gland is larger than the normal size for the patient’s age and gender. Some of the causes of goiter are iodine deficiency, thyroid nodules, Graves’ disease (GD). Goiter, hyperthyroidism, ophthalmopathy and dermopathy can be seen in GD. Compression symptoms due to goiter (dyspnea, dysphagia, superior vena cava syndrome) are also seen. Here, we will present a case of GD with superior vena cava syndrome.
Case:
A 50-year-old male patient, who had been using methimazole for 6 years due to hyperthyroidism, applied to our outpatient clinic with swelling in the neck. The patient was taking methimazole 10 mg/day. On physical examination, he had goiter, bilateral venous collaterals in the neck, and inactive Graves’ ophthalmopathy. Pemberton’s sign was positive. In laboratory tests, TSH, fT4, fT3, antiTPO, antiTG, TSH receptor antibody were: <0.008 mU/l, 1.01 ng/dl, 10.6 ng/l,>13000 U/l (<60 negative), 724 IU/ml (<1.3 negative), 34.3 U/l (≤1 negative), respectively. In the thyroid ultrasound, the dimensions of the right lobe were 33.9x33.4x73.4 mm, the dimensions of the left lobe were 35.3x50x78.5 mm, the dimension of the isthmus was 20 mm, no thyroid nodule was observed. The thyroid gland showed retrosternal extension. Thyroid scintigraphy was consistent with GD. Computed tomography of the neck and thorax was performed to evaluate the differential diagnosis and cervical region: The dimensions of both thyroid lobes have increased considerably, extending to the paraesophageal, paratracheal, and intrathoracic retrosternal areas, and significant extrinsic compression of the larynx and esophagus was observed. In addition, bilateral subclavian veins were pressed by the thyroid gland, and diffuse dilated venous structures were observed in the skin-subcutaneous part of the anterior of the thyroid. Varicose dilated veins were observed in the anterior mediastinum. (Secondary to subclavian vein compression?). No pathological finding was detected in the lung parenchyma. Bilateral total thyroidectomy was performed. Its pathology was reported as diffuse toxic hyperplasic thyroid gland. Venous collaterals in the neck of the patient disappeared in the postoperative period. Clinical improvement was observed.
Conclusion:
The most common cause of hyperthyroidism is GD. Compression symptoms due to diffuse hyperplasia of the thyroid gland may be seen. In particular, the retrosternal extending goiter may cause superior vena cava syndrome by compressing the vascular structures. The most common cause of superior vena cava syndrome is malignancy. GD should also be considered in the differential diagnosis of superior vena cava syndrome. Improvement in this situation is expected with thyroidectomy.
327 - Adrenal incidentaloma, single center clinical experience - 2022
Uluslararası Bildiriler 24th European Congress of Endocrinology, 21-24 May 2022, Milan, Italy, Endocrine Abstracts (2022), Vol 81, P504
Backgorund:
Adrenal incidentalomas (AI) are lesions discovered incidentally on imaging without clinical symptoms or examination findings. AI can produce hormones in 5-30% of cases. Autonomic cortisol secretion (ACS) is the most common of these. Although ACS is asymptomatic, it increases the risk of metabolic disorders.
Methods:
Patients aged <18 years with adrenal adenoma and upper abdominal MRI who presented and were examined in the endocrinology outpatient clinic, had their data retrospectively documented. Comorbidities, examinations and hormonal tests and results of these patients were evaluated. Those who failed dexamethasone suppression tests (cortisol>1.8 g/dl) and did not have Cushing’s syndrome were classified as ACS.
Results:
Among the 223 patients, 138 (61.9%) were women with a median age of 56 (18-80). Of the patients, 26.9% had diabetes mellitus (DM), 54.3% had hypertension (HT), 17.9% had hyperlipidemia (HL), 12.1% had coronary artery disease (CAD), 1.3% had heart failure (HF). Hormone testing revealed that 6 (2.6%) of the patients had primary aldosteronism, 5 (2.2%) had pheochromocytoma, and 35 (15.6%) had ACS. Patients with and without ACS were compared for the presence of other additional diseases and adenoma size (Table-1). DM, HT and HL were higher in the ACS group (P<0.05, for each). Adenoma size was larger in the ACS group (P<0.05). Both groups had comparable age and sex distribution (P>0.05).
Conclusion:
Individuals with large adenomas are more likely to have ACS. Large adrenal adenomas should be monitored for ACS and associated cardiometabolic risks, as well as necessary treatments.
Table 1. Comparison of patient characteristics with and without autonomic cortisol secretion
Autonomic cortisol secretion | Yes | No | p |
Sex, Woman/Man | 2.18 | 1.54 | 0.45 |
Age (years), median (min-max) | 59 (36-80) | 55 (18-74) | 0.071 |
Size of adenoma (mm) | 25 (10-54) | 18 (10-60) | 0.001 |
T2DM | 17 (48.6%) | 43 (22.9%) | 0.002 |
HT | 25 (71.4%) | 96 (51.1%) | 0.028 |
HL | 13 (37.1%) | 27 (14.4%) | 0.003 |
CAD | 7 (20%) | 20 (10.6%) | 0.154 |
HF | 1 (2.9%) | 2 (1.1%) | 0.402 |
Osteoporosis or osteopenia | 6 (30%) | 13 (56.5%) | 0.125 |
T2DM type 2 diabetes mellitus, HT hypertension, HL hyperlipidemia, CAD coronary artery disease, HF heart failure
326 - Calcitonin washout in the diagnosis of medullary thyroid cancer - 2022
Uluslararası Bildiriler 24th European Congress of Endocrinology, 21-24 May 2022, Milan, Italy, Endocrine Abstracts (2022), Vol 81, RC14.5
Background:
Medullary thyroid cancers (MTC) originate from parafollicular C cells and constitute 3-5% of all thyroid cancers. Calcitonin (CT) measurement is useful in the diagnosis of MTC. The sensitivity and specificity of CT are low in the measurement alone, and the sensitivity and specificity increase when used with pentagastrin and calcium stimulation tests. However, the difficulty of accessing pentagastrin, the uncertainty of the cut-off value in calcium stimulation tests, the differences in calcitonin assay and the costs complicate the use of serum CT and stimulation tests in the diagnosis. For this reason, guidelines do not offer opposing or supportive recommendations about the routine measurement of CT in patients with thyroid nodules. In this study, we aimed to investigate the contribution of CT washout of the nodule (WO) to routine CT measurement for MTC diagnosis.
Methods:
In our clinic for the last three years, calcitonin values have been routinely measured in patients with nodular thyroid disease. CT-WO is performed for the nodules of patients whose calcitonin values are still above the laboratory cutoff levels in repeated measurements after excluding confounding factors. CT-WO was implemented after the thyroid fine-needle aspiration biopsy specimen was spread on a slide. The remaining material was washed with 1 mL of saline, and then the CT level was measured. In this study, the results of 33 patients who were operated on will be presented.
Results:
Papillary thyroid cancer (PTC) was found in 12 (36.4%), MTC in 14 (42.4%) and benign pathology in 7 (21.2%) of the patients. CT washout was performed on 69 nodules of these patients before surgery. According to the pathology reports, eleven of these nodules were PTC, 13 were MTC, and 45 were benign. PTC and MTC were detected incidentally in two separate patients. In patients with MTC, serum CT and CT-WO values were significantly higher than the other two pathology groups (P=0.001). ROC analysis was performed for serum CT value, and the level 29.9 determined MTC with 100% sensitivity and 90% specificity (AUC=0.975 (0.932-1), P<0.001). Also, ROC analysis was performed for the CT-WO values of the nodules, and level 413.5 determined MTC with 100%
sensitivity and 86% specificity (AUC=0.987 (0.965-1), P<0.001). The median MTC diameter in the thyroidectomy specimens was 1 cm (0.6-5.5). Micro MTC was detected in 8 (61.5%) of the patients.
Conclusion:
CT-WO appears to be useful in diagnosing MTC early and accurately.
325 - Can early postoperative hypocalcemia be predicted preoperatively in patients operated with minimally invasive technique for primary hyperparathyroidism? - 2022
Uluslararası Bildiriler 24th European Congress of Endocrinology, 21-24 May 2022, Milan, Italy, Endocrine Abstracts (2022), Vol 81, RC14.3
Aim:
Postoperative hypocalcemia is seen in 26-42% patients after parathyroidectomy. There are quite a lot of studies investigating preoperative factors that might be used to predict postoperative hypocalcemia in thyroidectomized patients, however there are less studies in parathyroidectomized patients.In this study, our aim was to determine whether any preoperative clinical, laboratory or ultrasonographical feature anticipate hypocalcemia in parathyroidectomized patients due to primary hyperparathyroidism (PHPT).
Material and Methods:
All patients operated for PHPT between 2019-2022 were retrospectively evaluated.Patients undergoing minimally invasive parathyroidectomy were enrolled.Demographic, clinical, ultrasonography and histopathology results were noted and compared in patients with and without hypocalcemia (Group-1 and Group-2,respectively) within two days after surgery.
Results:
Of 179 parathyroidectomized patients, 93 were operated with minimally invasive procedure. Postoperative hypocalcemia was observed in 21 (22.6%) patients. Group-1 was younger compared to Group-2 (P=0.036).Gender distribution and presence of osteoporosis were comparable.Nephrolithiasis was less prevalant in Group 1 (P=0.046).Preoperative levels of corrected calcium, phosphorus, magnesium, parathyroid hormone, alkaline phosphatase, 25 OH vitamin D were similar in two groups. Fractional excretion of calcium (FECa) was lower in group-1 (P=0.048).The optimal cut-off level of FECa that was predictive for postoperative hypoprathyroidism was 0.0216 with a sensitivity of 61.9% and specificity of 54.9% (AUC 0.643±0.062, P=0.048).Ultrasonographic and histopathologic diameters and volumes of parathyroid lesions were not different in both groups (p>0.05 for all).Histopathological diagnosis was parathyroid adenoma in 76 (64.5%) patients, parathyroid hyperplasia in 9 (9.7%) patients, and cell-rich parathyroid gland in 8 (8.6%) patients.The distribution of the histopathological results were similar in two groups(P=0.750).
Conclusions:
Younger patients, patients with lower FECa and without nephrolithiasis undergoing minimally invasive parathyroidectomy for PHPT might require closer follow-up for the development of postoperative hypocalcemia. FECa lower than 0.0216 might help to predict occurrence of postoperative hypocalcemia.
| Group-1 (Patients with postoperative hypocalcemia) (n=21, 22.6%) | Group-2 (Patients without postoperative hypocalcemia) (n=72, 77.4%) | p |
| n(%),[median (Q1-Q3)] | n(%),[median (Q1-Q3)] |
|
Age (year) | 45.4±11.8 | 51.9±12.4 | 0.036 |
Gender (women) | 18 (85.7) | 53 (73.6) | 0.251 |
Corrected calcium (N:8.7-10.4 mg/dl) | 10.5 (10.2-10.7) | 10.7 (10.3-11.4) | 0.127 |
Phosphorus (N:2.4-5.1 mg/dl) | 2.9±0.6 | 2.7±4.6 | 0.055 |
Magnesium (1.3-2.7 mg/dl) (n=83) | 2.1±0.1 | 2.0±0.2 | 0.091 |
Alkaline phosphatase (42-98 U/l) (n=91) | 103 (95-128) | 113 (86-144) | 0.950 |
Parathyroid hormone (18.4-80.1 ng/ml) | 188,5 (147.0-210.0) | 191.0 (140.5-281.8) | 0.443 |
25 OH Vitamin D3 (25-80 ng/ml) (n=92) | 19.8 (11.2-23.5) | 16.0 (11.0-22.0) | 0.466 |
Fractional excretion of calcium | 0.0213 (0.0146-0.0229 | 0.0225 (0.0177-0.0279) | 0.048 |
Presence of nephrolithiasis | 4 (19.0) | 31 (43.1) | 0.046 |
Presence of osteoporosis | 10 (47.6) | 26 (36.1) | 0.279 |
Number of removed parathyroid lesions | 1 (1-2) | 1 (1-3) | 0.212 |
324 - The effect of multiple passes to the same thyroid nodule in the fine needle aspiration biopsy session on obtaining adequate and/or the AUS/FLUS cytological result - 2022
Uluslararası Bildiriler 24th European Congress of Endocrinology, 21-24 May 2022, Milan, Italy, Endocrine Abstracts (2022), Vol 81, OC14.5
Aim:
To determine whether multiple fine needle passes to the same thyroid nodule in the fine needle aspiration biopsy (FNA) session affect sufficient and/or atypia of undetermined significance/follicular lesion of undetermined significance (AUS/-FLUS) cytological result.
Materials and Methods:
Ultrasonography (US) and cyto-histopathology results of the nodules of patients who were diagnosed with thyroid nodules and underwent FNA between May-August 2021 were retrospectively analyzed. The nodules were divided into two groups according to the number of needle passes performed in the same FNA session as those with one pass (one-pass group) and those with two or three passes (multiple-passes group). The two groups were compared in terms of cytological adequacy and the rate of AUS/FLUS diagnosis as well as US features and TIRADS scores.
Results:
A total of 1500 thyroid nodules of 708 patients (575 female and 133 male) were included in the study. The mean age of the patients was 51.57±12.51 years. 1409 (93.9%) nodules were performed one pass, and 91 (6.1%) were performed two (n=85) or three passes (n=6). While the cystic/mixed nodule ratio and macrocalcification rate were higher in the multiple-passes group, the rates of coalescent nodules and presence of halo were higher in the one-pass group (P=0.001, P=0.039, P=0.006, and P=0.040, respectively). TIRADS 3 score was higher in multiple-passes group (P=0.001). The adequacy and AUS/FLUS ratios were similar in the two groups.When nodules with macrocalcifications and cystic/mixed structures were evaluated as two separate subgroups, the adequacy and AUS/FLUS ratios were similar in one-pass and multiple-passes groups.
Conclusion:
Two or three passes to thyroid nodules have similar cytological adequacy and AUS/FLUS ratios compared to one pass.Although more passes are performed in cystic/mixed and macrocalcified nodules estimating that the material would be insufficient with macroscopic on-site evaluation, needle insertion of two or three times does not contribute to the adequacy and also the AUS/FLUS ratio compared to one pass.
Features | One-pass (n=1409) | Multiple-passes (n=91) | p |
Cystic/mixed structure [n (%)] | 87 (6.2) | 14 (15.4) | 0.001 |
Presence of macrocalcification [n (%)] | 119 (8.4) | 14 (15.4) | 0.039 |
Presence of peripheral halo [n (%)] | 250 (17.7) | 8 (8.8) | 0.040 |
Coalescence [n (%)] | 149 (10.6) | 1 (1.1) | 0.006 |
TIRADS Category | 0.003 | ||
3 | 73 (5.2) | 12 (13.2) | 0.001 |
4a | 702 (49.8) | 40 (44.0) | 0.278 |
4b | 579 (41.1) | 32 (35.2) | 0.265 |
4c | 55 (3.9) | 7 (7.7) | 0.078 |
5 | 0 (0.0) | 0 (0.0) | |
Cytological sufficiency [n (%)] | 1033 (73.3) | 65 (71.4) | 0.694 |
AUS/FLUS cytology [n (%)] | 240 (17.0) | 9 (9.9) | 0.103 |
323 - Are the neutrophil-to-lymphocyte ratio and large unstained cells (LUCs) different in hospitalized patients COVID-19 PCR positive with and without diabetes mellitus? - 2022
Uluslararası Bildiriler 24th European Congress of Endocrinology, 21-24 May 2022, Milan, Italy, Endocrine Abstracts (2022), Vol 81, OC14.3
Objectives:
The novel coronavirus disease-2019 (COVID-19) is the fastest-spreading disease worldwide, with over 380 million cases and 5 million deaths. The presence of diabetes mellitus (DM) in patients with COVID-19 was associated with mortality, acute respiratory distress syndrome, disease progression. COVID-19 was progressed with some hematological disorders, especially lymphopenia. Studies implicated that neutrophil-to-lymphocyte ratio (NLR) level can be a reliable marker in showing the severity of COVID-19 disease. A routine hematology analyzer measures the percentage of large unstained cells (%LUCs), reflecting activated lymphocytes and peroxidase-negative cells. In previous studies, the%LUCs was found to be associated with disease progression in patients with HIV. This study aims to investigate whether the%LUCs and NLR parameters are associated with disease progression in diabetic patients with COVID-19.
Materials and Methods:
The data of the patients hospitalized in the Infectious Diseases Service and Intensive Care Unit with a COVID-19 in Ankara City Hospital between 15.03.2020 and 15.07.2020were collected in our retrospective study. This study included 656 patients with COVID-19, 131 withDM, and 525 with theDM-free control group.White blood cell (WBC) count, neutrophils, neutrophil percentage, lymphocytes, lymphocyte percentage, LUCs,%LUCs, NLR, platelets, hemoglobin which was taken within the first 24 hours after admission, and history of DM were noted from the records.
Results:
The mean age was 61.29±13.81 years in the diabetic patient group and 44.37± 17.14 years in the non-diabetic control group with COVID-19, which was significantly higher in the diabetic group (P<0.001). NLR,WBC count, neutrophils, and neutrophil percentage were statistically significantly higher in patients with DM (respectively, P<0.001, P=0.008, P=0.008, P=0.003, and P=0.049). There were no significant differences between the groups regarding lymphocyte, platelet, LUCs, and%LUCs values (P>0.05).
Conclusion
There are studies in the literature that a decrease in%LUCs value and an increase in NLR are indicators of severe disease in COVID-19. Our study did not detect a difference in%LUCs value in diabetic patients, but our study is a preliminary study. Analysis of the data with clinics continues with more patients.
322 - Millimetric and Symptomatic Isolated Left Adrenal Medullary Hyperplasia. - 2021
Uluslararası Bildiriler Endobridge 2021, 21-24 October 2021, EP-015
OBJECTIVE: Catecholamine-secreting tumors originating from chromaffin cells of the adrenal medulla are called pheochromocytomas. Although pheochromocytomas may occur at any age, they are most common in the fourth to fifth decade.The symptoms of pheochromocytomas are caused by tumoral hypersecretion of catecholamines, 85 percent of catecholamine-secreting tumors are m the adrenal. Adrenal medullary hyperplasia (AMH) is defined as nodular or diffuse lesion of <1 cm in the adrenal medulla, where larger lesions are regarded as pheochromocytoma. ln this report, we present a case diagnosed as nine- millimeter symptomatic AMH.
CASE: A 30-year-old man presented with newly diagnosed hypertension; because he was a doctor, he had examined his blood pressure and found it had risen to 160 mmHg. The endocrinological reasons that may cause secondary hypertension were investigated; 24-hour urine catecholamines were high. High values of catecholamines as well as metanephrine 608 ug/24h (52-341 ug/24h) and normetanephrine 1227 ug/24h (88-444 ug/24h).Plasma renin activity, aldosterone, thyroid-stimulating hormone, intact parathyroid hormone, calcium, calcitonin, carcinoembryonic antigen, metanephrine. normetanephrine. epinephrine, norepinephrine levels were in the normal range. One milligram dexamethasone suppression test was suppressed. The findings of a physical examination were all normal. He had no medical or family history of pheochromocytoma and related syndromes. However his cousin had hypertension diagnose when he was 30 years old. No pathology was detected in the retinal examination. Ultrasonography revealed no morphological abnormalities of the thyroids, parathyroids. No pathology was detected in the adrenal MRI. 1231-metaiodobenzylguanidme (MIBG) single-photon emission computed tomography (SPECT) revealed specific uptake in a seven-millimetric nodule in the left adrenal gland Gallium-68 DOTA-O-Phel-Tyr-3 octreotate positron emission tomography (Ga-68 DOTATATE PET) was performed; reported as specific asymmetric uptake in a nine-millimetric nodule in the left adrenal gland. Adrenal MRI was re-evaluated; was reported as seven millimetric asymmetric nodular thickenings m the left adrenal gland. The patient was consulted with the genetic department, and there was no mutation at the succinate dehydrogenase beta (SDHB) gene. Other genetic tests have not yet been concluded. He was prescribed doxazosin which controls his blood pressure. Two months later, he had a surgery of laparoscopic left partial adrenalectomy. Histopathological findings confirmed a diagnosis of AMH. The patient s urine catecholamine levels decreased after surgery, his blood pressure was kept under control without medication.
CONCLUSION: A diagnosis of unilateral AMH is important because AMH resection can effectively treat hypertension. Because the lesions in AMH are small, they may not be visualized on CT or MRI so; 1231- MIBG-SPECT and Ga-68 DOTATATE PET are necessary diagnostic scanning modalities for AMH.
320 - Co-excistent gastric neuroendocrine cell hyperplasia, parathyroid adenoma and oral lichen planus. - 2021
Uluslararası Bildiriler Endobridge 2021, 21-24 October 2021, EP-068
Introduction: Gastric neuroendocrine tumors (NETs) derive from enterochromaffin-like cells in the gastric mucosa (1). Neuroendocrine hyperplasia of the stomach is a rare but important cellular event which can lead to development of gastric neuroendocrine tumor (2).
Case report: A 63-year-old female patient was admitted to our clinic with hypercalcemia. She had asthma, sleep apnea syndrome and oral lichen planus which was erosive and resistant to treatment for five years. Laboratory tests were as follows; calcium 11.5 mg/dL(8.4-10.2), albumine 3.9 g/dL(3.5-5.2), phosphorus 2.5 mg/dL(2.5-4.5), creatinine 0.74 mg/dL(0.5-1.1), parathyroid hormone 194pg/mL(15-65), 25OHvitaminD3 21.2 ng/mL(25-80), 24-hours urine calcium 236.5 mg/24hour (100-300). DEXA revealed a L1-L4 t-score of -2, femoral neck t score of -2.2, radius t score of -4.1. A lesion consistent with parathyroid adenoma was detected in ultrasonography and the patient underwent parathyroidectomy. A parathyroid adenoma and branchial cleft cyst were detected histopathologically. Upper GIS endoscopical biopsy performed for iron deficiency anemia was consistent with gastritis, atrophic intestinal metaplasia and neuroendocrine cell hyperplasia. Endosonography showed a 4 mm yellowish-colored appearance suggesting a carcinoid tumor, and 6 and 3 mm xanthoma in the posterior corpus wall and proximal antrum. Linearly increased pathological Ga-68 DOTATATE activity was observed in the posterior wall of the gastric corpus. Chromogranin A was 255.9ng/mL(0-100), gastrin was 607 pg/mL(13-115), neuron specific enolase was 13.4 ng/mIL(0-17). Multiple gastric biopsy results revealed a grade 1/3 (well differentiated) neuroendocrine tumor with Ki 67 proliferation index <2% and micronodular neuroendocrine hyperplasia in nontumoral areas, polypectomy was performed to two polip. Ga-68 DOTATATE imaging performed one year later showed decreased involvement of the gastric corpus and fundus. Calcium, parathyroid hormone, 24-hour urine catecholamines, pituitary hormones and pituitary MRI were normal. No mutation was detected in CDKN1B, MEN1 and RET genes.
Discussions: The diagnosis of gastric neuroendocrine tumor may be possible by multiple gastric biopsy in cases with gastric neuroendocrine cell hyperplasia (3). Patient with gastric neuroendocrine tumor and parathyroid adenoma may not have mutation in MEN genes.
319 - Eosinophilic granulomatosis with polyangiitis as a rare cause of the syndrome of inappropriate antidiuretic hormone secretion - 2021
Uluslararası Bildiriler Endobridge 2021, 21-24 October 2021, EP-038.
BACKGROUND: Eosinophilic granulomatosis with polyangiitis (EGPA, Churg-Strauss syndrome) is a rare multisystem necrotizing vasculitis that involves the small-to-medium-sized blood vessels and characterized by chronic rhinosinusitis, asthma, and eosinophilia. We report a rare case of the syndrome of inappropriate antidiuretic hormone (ADH) secretion (SIADH) secondary to EGPA.
CLINICAL CASE: A 53-year-old man applied with complaints of pain in the large joints and morning stiffness in knee for two months. The patient had the history of impaired fasting glucose, asthma, nasal polyp, urticaria, angioedema, hypertension, hyperlipidemia and obsessive-compulsive disorder. Physical examination revealed intrinsic muscle atrophy and weakness in right hand. Peripheral eosinophil count was 9.78x109/L (0.02-0.5), erythrocyte sedimentation rate 39 mm/h (0-20), and Creactive protein 0,0577 g/L (0-0.005). Rheumatoid factor, antinuclear, anti neutrophyl cytoplasmic and anti-cyclic citrulinated peptide antibodies were negative, complement 3 and 4 levels were within normal ranges. Migratory ground-glass pulmonary opacities had been reported in multiple previous chest computed tomography scans. Echocardiography revealed findings compatible with eosinophilic involvement. Electroneuromyographic evaluation showed acute distal axonal neuropathy of right ulnar nerve. EGPA was considered in the patient and oral methylprednisolone treatment was initiated. After myeloproliferative disorders were excluded by bone marrow biopsy, intravenous immunoglobulin (IVIG) and cyclophosphamide treatment and gradual tapering of oral steroids were planned. In pretreatment examination hyponatremia was detected (serum sodium was 123 mEq/L (132-146)) which persisted during follow-up. In twenty-four hour urine analysis, sodium was 387 mEq, creatinine was 1156 mg and volume was 3000 mL. When his medical records were investigated it was observed that hyponatremia was present for nearly two years. He had neither hyponatremia symptoms nor hypervolemia. No history of diuretic use, hyperlipidemia, and hyperproteinemia was present. Thyroid, adrenal, renal, and hepatic function tests were normal. While serum osmolality was 270, urine osmolality was 911 mOsm/kgH2O. So, SIADH diagnosis was made. Cranial MRI revealed no hypothalamo-hypophyseal ischemia, infiltration or mass lesion. Fluid intake was restricted. Although the patient's sodium level did not return to normal, it rose up to 130 mEq/L. After second cycle of EGPA treatment (cyclophosphamide and IVIG), serum sodium level was became normal.
CONCLUSION: Underlying pathologies of SIADH are numerous and treat-to-target approach improves it and so hyponatremia. There is only four other documented cases of SIADH with EGPA. We hypothesized that blood supply to the hypothalamus and/or posterior hypophysis might be affected from EGPA vasculitis. This report is important because showing that SIADH may be potentially resulted from or concomitant with EGPA
318 - A rare cause of levothyroxine malabsorption: Ileostomy. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, EP239
Introduction: It is recommended to determine levothyroxine (LT4) dose individually in patients with hypothyroidism. However, higher doses of LT4 therapy are required to achieve target TSH levels in significant number of patients. Oral LT4 absorption occurs in the small intestine, especially in the jejunum and proximal ileum, while a small amount is absorbed in duodenum. Causes of LT4 malabsorption include helicobacter pylori infection, chronic atrophic gastritis, celiac disease, lactose intolerance, pancreatic insufficiency, cirrhosis, nephrotic syndrome, gastrointestinal malabsorptive surgical procedures, short bowel syndrome, drug and diet-related interactions. Here, we present a case of ileostomy with multiple small intestine resection, which is a rare cause of LT4 malabsorption. Case: A 59-year-old male patient was consulted to our endocrinology clinic due to high TSH levels before ileostomy closure from the gastrosurgery clinic. The patient underwent total thyroidectomy in 2009 due to medical recurrence Graves disease and had postoperative hypothyroidism, he was euthyroid with levothyroxine treatment of 175 μg/day. With the diagnosis of rectal cancer in January 2020, the patient underwent a low anterior resection and colostomy. Pathology reported as moderately differentiated adenocarcinoma, followed by chemotherapy and radiotherapy. In October and November 2020, segmental small bowel resection due to radiation ileitis, ileus was performed. Ileostomy was performed in November 2020 for the patient whose colostomy did not work for a long time. Despite medical treatment, ileostomy was planned to be closed after 8 weeks due to the daily discharge of 14 times from ileostomy. It was consulted preoperatively in January 2021 due to TSH:66 mU/l. The oral levothyroxine dose was gradually increased from 150 μg/day to 350 μg/day due to increase in TSH to 80 mU/l, despite appropriate replacement of levothyroxine. When his TSH level was 37 mU/l, free T4 and T3 were normal with 350 μg/day oral levothyroxine, ileostomy was closed in February 2021. The patient’s free T4 and T3 values started to increase in 3 days after ileostomy closure, and levothyroxine dose was gradually decreased. The patient has been followed euthyroid with levothyroxine doşe of 150 μg/day. Conclusion: Intestinal absorption problems may cause high-dose LT4 therapy. The decrease of the intestinal absorption surface and the shortening of the intestinal transit time can be considered among malabsorption mechanisms. Further research should be conducted in the presence of increased serum TSH levels despite high dose LT4 therapy.
317 - Prostate cancer metastasis to cervical node chain-an unusual clinic. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, EP238
Introduction: While cervical lymph nodes are the region where head and neck malignancies frequently metastasize, prostate carcinoma rarely metastasizes to this area. Here, we will present a case with papillary thyroid microcarcinoma whose pathological lymph node cytology in the cervical region was found to be prostate carcinoma metastasis. Case: Since thyroid fine needle aspiration cytology (FNAC) results were nondiagnostic 3 times, an 64-year old male patient underwent bilateral total thyroidectomy. His pathological examination was compatible with papillary microcarcinoma, and was given 100 mci radioactive iodine (RAI) treatment. While post-ablation whole body scan (WBS) revealed the activity involvement compatible with residual tissue in the right lobe region, the diagnostic WBS was found to be normal (TSH, Tg and Anti Tg values are shown in Table 1). In PET-CT, pathological increased activity uptake was detected in the bilateral level IV lymph node area. Neck ultrasonography showed a lymph node with pathological appearance and 8.5×8.7×11 mm in size at left level IV. Cytological examination of this lymph node was compatible with carcinoma metastasis. Also, another pathological looking lymph node on the left level IV with 7.7×9.4×10.8 mm in size was found to be compatible with malignant cytology, carcinoma metastasis (Table 1). An immunohistochemical study of the prostate and thyroid origin (PSA, TTF1) has been conducted in cytology, but a definitive clue for the origin of the tumor has not been obtained. Thereupon, the FNAC was repeated from the level IV lymph node (8.5×8.7× 11 mm) of the patient and nondiagnostic cytology was found, afterall the cell block was applied. Finally, left level IV lymph node cytology was reported to be compatible with prostate adenocarcinoma metastasis. Table-1
TSH; thyroid stimulating hormone, Tg; thyroglobulin, Anti-Tg; anti- thyroglobulin,
WBS; whole body scan, RAI; radioactive iodine
Conclusion: Metastatic prostate adenocarcinoma (PAC) to cervical lymph nodes is rare. If the history is unknown, cases may be misdiagnosed as metastases from cervical neoplasms. Findings showing metastatic PAC to the cervical lymph nodes in FNAC are; the involvement of left-sided cervical lymph nodes and cellular smears consisting of flat layers with granular cytoplasm and uniform polygonal cells arranged in the acini, fuzzy cell borders, and round-oval nuclei with prominent nucleoli.
316 - Reduction in medication of multidrug hypersensitive patient by bariatric surgery. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, EP233
Introduction: Type 2 diabetes and hyperlipidemia are primarily managed with lifestyle modifications, self-monitoring of blood glucose, and medication. Patients who are obese and cannot achieve normal blood glucose levels despite diet, exercise, and multiple medications may be considered for bariatric surgery. Many diabetic patients with very high triglyceride levels are at high risk for ASCVD and therefore after triglyceride levels are controlled the patient should be evaluated for cardiovascular disease risk. Bariatric surgery is more effective at inducing weight loss than either diet or medications. Baratric surgrey is alsow associated more robust decrease in serum triglyceride levels and increase in HDL-C levels. Here we describe a bariatric surgery results of obese multidrug hypersensitive patient with a high level of serum triglyceride. Case: 44 years old woman, had Type-2 Diabetes Mellitus and hyperlipidemia for at least 3 years. She had no medication due to multidrug hypersensitive. Her BMI was 39.9, fasting glucose, serum triglyceride, VLDL, HDL, HbA1C are: 166 mg/dl, 2166 mg/dl, 433 mg/dl, 32 mg/dl, 60 mmol/mol respectively. İn addition to Initial treatment of very low-fat diet, we immediately started medication to reduce triglyceride levels into a safe range to prevent triglyceride-induced pancreatitis. After 10 day of receiving fenofibrate and dapagloflozin she had an generalized acute urticaria need hospitalization and first treated with antihistamine drugs. Here serum triglyceride level was 1906 that force us to continue medication tratment with antihistamine drug. After 4 mounth of treatment and weight loss (10 kg) we didn’t reach therapy goals of hyperlipidemıa. The patient had a bariatric surgrey after mutidisplanary consensur. After surgrey she stoped medication and her serum triglyceride measure was 240 mg/dl. Conclusion: We report a case of generalized urticaria probable or very probable induced by fenofibrate underwent bariatric surgery. Approximately 60-70%of patients with obesity are dyslipidemic. The Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy have been shown to improve A1C, reduce weight, and reduce the number of medications patients need for diabetes management. Comorbidities such as hyperlipidemia and hypertension also may improve. A reduction in medication of hypersensitive patients can be considered an additional benefit of bariatric surgery.
315 - Radioactive iodine therapy with recombinant human TSH (rhTSH) for well-differentiated thyroid cancer had no difference in GO outcome; case report. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP894
Background: The risk of cancer is relatively higher in Graves’ patients presenting simultaneously with thyroid nodules. Radioiodine (RAI) therapy recommended in intermediate-high risk differentiated thyroid carcinoma may be associated with worsening of a pre-existing Graves’ orbitopathy (GO) or developing a new onset. The impact of RAI therapy in patients with differentiated thyroid cancer on the course of a pre-exisiting GO has not been specifically investigated. we report a sever GO patient treated by recombinant Tsh (RhTSH) for intermediate-risk of papillary thyroid cancers (PTC). Case: A 47-year-old man, presented to our center with exophthalmos and ptosis of eyes. His thyroid function tests and thyroid autoantibodies were as follows: TSH; 0.01 (0.4–4 uIU/ml), FT3; 5.41 (1.6–4.9 pg/ml), FT4; 1.74 (0.78–1.76 ng/dl); anti TPO was positive TSH-R Ab; 1.249. On the ultrasonographic examination of the thyroid gland the paranchyme was heterogeneous and in the right lobe 11.2 × 8.9 mm heterogeneous, iso-hyporechogenic nodule and pathologic lymphadenopathy were detected in levels 4 of neck. US-guided fine-needle aspiration biopsy was performed and the cytological examination were suspicious for papillary thyroid cance of the nodule and malign sitology of the lymph node. Computed tomography scan of orbita demostrated bilateral anterior bulging of bulbus oculi clearly and bilateral enlargement of medial, inferior and superior rectus muscles and also swelling of the optic nerve. In addition to antithyroid and beta blocker, for severe ophthalmopathy intravenous pulse therapy with high doses of methylprednisolone as 500 mg tapered in 24 weeks duration, followed by 250 mg for 24 weeks. He underwent thyroidectomy and a dissection of the santral and right lateral lymph nodules was conducted. The diagnosis were PTC with < 5% of hobnail variant and mestatic lymph nodules was confirmed. Once stabilized of GO under oral methylprednisolone and became euthyroid he reseved 150 mCi RAI with rhTSH with no changes in GO after One month observation. Discussion: The risk of cancer is relatively higher in Graves’ patients in the presence of an accompanying nodular disease. Moreover, some authors reported that thyroid cancer associated with GD seemed to be more aggressive. RAI therapy is recommended in high-risk differentiated thyroid carcinoma, but it might worsen or induce a new onset of GO. Glucocorticoid treatment should be given especially in patients who will receive high doses of RAI. RAI with rhTSH had no difference in GO outcome at first month.
314 - Thyro-cutaneous fistula a rare presentation of thyroid lymphoma. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP885
Background: Primary thyroid lymphoma (PTL) is defined as a lymphoma involving only the thyroid gland or the thyroid gland and adjacent (regional) neck lymph nodes. Primary lymphomas of the thyroid are uncommon tumours, representing approximately 5% of the thyroid neoplasms and 2% of extranodal lymphomas. The most characteristic presentation is that of a rapidly enlarging neck mass often associated with dysphagia. The majority of patients are euthyroid and one third of patients have compressive symptoms. The mass is usually fixed to surrounding tissues and half the patients have unilateral or bilateral cervical lymph node enlargement. Abscess formation in the background of thyroid lymphoma with thyrocutaneous fistula is further rare. Reaching the final diagnosis can be delayed if insufficient biopsy material is obtained and it may be difficult to distinguish thyroid lymphoma from anaplastic carcinoma and thyroiditis. The present study describes the case of a patient who was presentad with abscess formation suggesting the possibility of anaplastic carcinoma and finaly diagnosd by diffuse large B-cell lymphoma.
Case: A 73-year-old female presented with anterior neck pain, hoarseness and rapidly expanding mass with abscess formation on here neck. The patient was admitted to our clinic for preoperative thyroid surgery suggesting the possibility of anaplastic carcinoma due to fine needle aspiration cytology of suspicious for malignancy. Her serum TSH was elevated to 47 mU/l and anti TPO was very high. Here neck ultrasound showed a significantly enlarged, diffuse parenchymal inhomogeneity and ill defined border of the thyroid gland. We performed Tru-cut biopsy and histological diagnosis was Diffuse large B-cell lymphoma of the thyroid gland. After 18FDG-positron emission tomography/computed tomography (PET/CT) scanning the patient reseaved 6 regimen of chemotherapy R-CHOP (rituximab, cyclophosphamide, doxorubicin [hydroxydoxorubicin], vincristine [Oncovin], prednisone with antibioticsand she has a good physical condition.
Discussion: Thyroid abscess is a rare clinical situation. It is most commonly associated with pyriform sinus fistula. Abscess formation in the background of thyroid cancer with thyro-cutaneous fistula is further rare. PTL is an uncommon malignancy of the thyroid. PTL occur most commonly in elderly women and are commonly of B-cell origin. Fine needle aspiration has become the procedure of choice for the initial pathological diagnosis of thyroid nodule. However, studies have also shown inconsistent results in the diagnosis of lymphoma of the thyroid. But clinical and radiological suspicion and cytomorphological features can help reaching the correct diagnosis in such cases.
313 - Hematological changes before and after radioactive iodine therapy. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP886
Objective: Radioactive iodine (RAI) therapy is widely used in both diagnosis and treatment of benign and malignant thyroid diseases. It is generally a well tolerated therapy. Bone marrow suppression is often a temporary side effect with a decrease in white blood cells and platelets up to 6–10 weeks. In this study, we aimed to examine hematological changes in patients who received RAI treatment for benign or malignant diseases of the thyroid. Methods: The records of patients who applied to our endocrinology clinic between January 2016 and January 2019 and received RAI treatment for benign or malignant etiologies were evaluated retrospectively. The demographic data of the patients and data on thyroid disease, additional diseases, and the drugs used were recorded, the patients were grouped according to the etiology and the RAI dose they received. Blood count parameters measured before RAI treatment within 7 days, after RAI treatment and at the last control of the patient were recorded and compared in these patients. Results: In the study, data of total 202 patients, including 158 women (77.5%) and 44 men (21.6%), were evaluated. 168 of these patients (82.4%) had received RAI treatment due to malign, and 34 benign (16.7%) etiologies. The median age they received RAI was 45 (20–84), while the median dose of RAI was 75 mCi (10–200). Pre-treatment and first control interval was median 44 (18–93) days, and the median time between pre-treatment and last control was 35 (4–56) months. In comparison of hematological parameters before and after treatment, the median leukocyte count was 7.72 (3.89–19.93) × 109/l before treatment, while it was significantly reduced 6.27 (0.86–14.5) × 109/l at the first control after treatment and 6.78 (3.58–10.8) × 109/l at the last control. Similarly, a decrease in neutrophil and lymphocyte counts was detected after treatment. While the median hemoglobin value was 13.95 (8.8–17.2) g/dl before RAI treatment, it was 13.5 (7.8–17.3) g/dl and 13.5 (6.7–17.6) g/dl at the first and last control after treatment, respectively. The median platelet count was 283 (149–563) × 109/l, and it was 250.5 (134–507) × 109/l at the first post-treatment control and 266.5 (116–539) × 109/l at the last control. While the median value of mean platelet volume(MPV) was 10.8 (8.5–13.8) fL before treatment, it was 10.15 (7.6–13.1) fL and 8.2 (6.6–11.1)fL, respectively, in controls. Conclusion: In our study, a significant decrease was found in the leukocyte, neutrophil, lymphocyte, platelet counts, hemoglobin levels and mean platelet volumes in the post RAI treatment period. According to these findings, it can be thought that the decrease in hematological parameters continues not only in the acute period but also in the chronic period after RAI.
312 - Clinical and pathological features of thyroid cancer in adolescents and young adults. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP882
Introduction: Thyroid cancer is the most common endocrine malignancy and its overall incidence has increased significantly in the last 30 years. Cancer in adolescents and young adults (AYA) is defined by the National Cancer Institute as diagnoses occurring among those aged 15 to 39 years. Thyroid cancer is the second most common cancer in the AYA population. In this study, we aimed to compare clinical, ultrasonographical, cytological and histopathological features of thyroid carcinoma in patients AYA with older counterparts. Materials and methods: The medical records of patients who underwent thyroidectomy between December 2006 and September 2016 and were diagnosed with thyroid cancer histopathologically were retrospectively reviewed. Patients were subdivided into two age groups: 1539 (Group1 ) and ? 40 years old (Group 2). Thyroid functions, ultrasonographic features of malignant nodules, cytological and histopathological findings were compared in patients with AYA patients and ? 40 years. Results: The study included 229 (22.6%) AYA patients and 784 (77.4%) patients aged ? 40 years. Thyroid functions, thyroid autoantibody positivity and thyroidectomy indications were similar. There were 305 (21.4%) and 1121 (78.6%) malignant foci in Group 1 and 2, respectively. Preoperative US features were similar in the two groups. Cytological results were distributed similarly in two groups (P = 0.512). Of all cancer types, 93.1% in Group 1 and 93.5% in Group 2 were papillary thyroid cancer (P = 0.772). Follicular cancer was found in 2.6% of Group 1 and 2.1% of Group 2 (P = 0.544). Medullary cancer constituted 1% of Group 1 and 1.1% of Group 2 (P = 0.895). Anaplastic cancer was found in 0.4% of Group 1 and 0.4% of Group 2 (P = 0.940). Lymph node metastasis was detected in 9.2% of group 1 and 7.4% of group 2 (P = 0.246). Distant metastasis was not detected in group 1, and it was found in 3 (0.4%) patients in group 2 (P = 0.366). There was not any significant difference in capsular and vascular invasion and extracapsular extension between groups. Conclusion: Previous studies have found that although AYA patients are more likely to be diagnosed with locoregional lymph node involvement compared to older patients, they are less likely to be diagnosed with distant metastases. In our study, the rate of diagnosis of lymph node metastasis was higher and the rate of distant metastasis was lower, but the difference was not statistically significant.
311 - A tru-cut biopsy proven rare thyroid neoplasia in a giant nodule with a benign fine needle aspiration cytology. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP884
Introduction: Extramedullary plasmacytoma (EMP) is a plasma cell neoplasm of extraosseous tissues. Less than 5% of all plasma cell neoplasms develop extramedullary. EMP is most common in the upper respiratory tract and oral cavity. The thyroid gland is one of the extremely rare regions. It is more common in men and the average age at diagnosis is 55. Primary thyroid plasmacytoma is one of the rare thyroid neoplasms. It often manifests as a rapidly growing mass in the neck and cause symptoms due to mass pressure. Pathological evaluation is particularly important. At the diagnosis of thyroid plasmacytoma, multiple myeloma must be ruled out. Here we present our case of thyroid plasmacytoma diagnosed by tru-cut biopsy. Case: A 71-year-old female patient, with hypothyroidism and multinodular goiter since 2014, presented with a 6-month history of dyspnea and neck swelling. She had type 2 diabetes mellitus, hypertension, and coronary artery disease. Thyroid gland was grade 3, fixed nodules were bilateral palpable. Thyroid function tests were euthyroid on levothyroxine treatment and thyroid autoantibodies were positive. An ultrasound scan of the thyroid revealed an enlarged thyroid with thyroid nodules on the right and left lobes, extending to the isthmus with a significant increase in size compared to previous controls. Fine needle aspiration cytology was benign. Due to suspicion of thyroid lymphoma, tru-cut biopsy was performed which suggested plasma cell neoplasia and plasmacytoma. Hematology consultation was made, as a result of the tests, multiple myeloma and other plasma cell disorders were excluded. The patient was evaluated as extramedullary plasmacytoma. In the council of endocrinology and metabolism, hematology, general surgery, nuclear medicine and radiation oncology departments operation was preferred. Bilateral total thyroidectomy was performed, histopathology reported as plasma cell neoplasm. Radiotherapy was not considered to be given to the patient as she had no residue in the examinations performed in the postoperative period. The patient has been followed in remission for one year. Conclusion: Primary thyroid plasmacytoma is a rare thyroid neoplasm. Clinical examination and imaging methods are usually not determinative in diagnosis, pathological evaluation is at the forefront of diagnosis. Even if fine needle aspiration biopsy is benign, patients should be evaluated for tru-cut biopsy in case of clinical suspicion. In the begining, multiple myeloma must be ruled out. Regular follow-up of the patient is necessary, as conversion to multiple myeloma may occur rarely.
310 - Association of thiol/disulfide homeostasis with Bethesda classification of thyroid nodules and thyroid cancer. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP879
Background: Ultrasonography and fine needle aspiration biopsy are frequently used in the diagnosis of thyroid cancer. However, supportive data might be required in case of diagnostic difficulty. In this study, we investigated whether there is a relationship between thiol/disulfide homeostasis and cytological and histopathological diagnosis of thyroid nodules. Materials and methods: A total of 119 participants were included in the study (81 euthyroid nodular goiter patients and 28 age and body mass index matched healthy volunteers). The patient group consisted of individuals scheduled for thyroidectomy. Thyroidectomy indications were giant nodule, cytological diagnosis and patient preference. Patients with diseases that would affect thiol/disulfide homeostasis were excluded. Cytological findings, histopathology results were evaluated. Native thiol, total thiol, and disulfide concentrations were measured, and disulfide/native thiol, disulfide/total thiol and native thiol/total thiol ratios were calculated. Thiol/disulfide levels were analyzed with automated spectrophotometric method. Results: There was no significant difference in oxidative stress parameters between different Bethesda categories. However, the increasing Bethesda categories were weakly positively correlated with the disulfide/native thiol (r: 0.241, p:0.030) and disulfide/total thiol (r: 0.250 p: 0.024). The disulfide concentration was 16.07±9.28 μmol/l in histopathologically benign, 19.85±11.28 μmol/l in malignant, and 14.87±7.62 μmol/l in the control group (P<0.001, f=11.724). Disulfide/native thiol was calculated as 3.58±2.0 in the benign group, 5.50±2.85 in the malignant group, and 3.41±1.70 in the control group (P < 0.001, f=8.415). Disulfide/total thiol was significantly higher in the malignant compared to benign and control groups (4.96±2.24, 3.27±1.80 and 4.96±2.24, respectively, P <0.001, f=9.49). Conclusion: Oxidative stress parameters were significantly higher in thyroid cancer. A weak positive correlation was detected between Bethesda categories and the disulfide/native thiol ratio and the disulfide/total thiol ratio. In case of diagnostic difficulties, additional benefit can be obtained from thiol/disulfide measurement.
309 - Papillary thyroid microcarcinomas that metastasize to lymph nodes. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP877
Background: We aimed to determine clinicopathological features that can predict lymph node metastasis (LNM) in papillary thyroid microcarcinomas (PTMC). Methods: Medical records of 872 patients with papillary thyroid cancer >1 cm (PTC >1 cm) and 1184 patients with papillary thyroid microcancer (PTMC) (£1 cm) were reviewed retrospectively. Demographical, clinical and histopathological features of (PTC >1 cm) and PTMC were compared. Association between clinicopathological features and LNM in PTMC was investigated. Results: The median age of patients with PTMC was significantly higher than patients with PTC>1 cm (49 vs 46 years old, P < 0.001). Multifocality, capsular invasion, vascular invasion, extrathyroidal extension (ETE) and LNM were more frequent in patients with PTC>1cm compared to patients with PMTC (P <0.001 for each). In PTMC group, those with LNM had significantly higher proportion of multifocality, capsular invasion, vascular invasion and ETE compared to those without LNM (P = 0.007, <0.001, P = 0.011 and P <0.001, respectively). Multifocality and ETE were significant factors for LNM with logistic regression analysis. Multifocality increased the risk of LNM by 1.737 times (95% CI: 1.079–2.979) and ETE increased the risk by 3.528 times (95%: 1.914–6.503). Primary tumor diameter ≥5.75 mm was predictive for LNM with a sensitivity of 0.782 and a specificity of 0.517 in PTMC. Conclusion: LNM should be investigated more carefully in patients with PTMC in the presence of tumor diameter≥5.75 mm, multifocality or ETE.
308 - A rare cause of malignant pleural effusion: Poorly differentiated thyroid carcinoma. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP872
Purpose: Poorly differentiated thyroid carcinoma (PDTC); is a rare type of thyroid cancer with a high risk of recurrence, metastasis, and death. Pleural effusion due to thyroid cancer has seldom been reported. In this report, we present a case with PDTC related malignant pleural effusion. Case: A 66-year-old male patient presented with neck swelling and shortness of breath. At another center, thyroid ultrasonography revealed a multinodular goiter and an irregularly circumscribed lymphadenopathy on the left level IV. He had multiple lung metastases in thorax computed tomography (CT). Positron emission tomography/computed tomography (PET-CT) detected “hypermetabolism in malignant nodules in the thyroid, multiple metastatic lymph nodes in the neck and bilateral metastatic lung nodules.” Cytology of lymph nodes at the right level 3,4,6–2a junction was malignant. The patient underwent bilateral total thyroidectomy, bilateral central lymph node dissection, and right modified radical neck dissection with a final pathologic diagnosis of “poorly differentiated thyroid carcinoma, right lateral and central tumor positive lymph node.” Upon persistence of dyspnea, thoracentesis was performed for a left-sided pleural effusion, which in the end had exudative characteristics. [blood thyroglobulin (Tg): 23960 ng/ml, Tg with pleural fluid dilution > 30000 ng/ml]. Cytology confirmed carcinoma infiltration. In the follow-up, mediastinal, lung, and pleural metastases in addition to effusion in the left hemithorax persisted. We performed pleurodesis after the initial tube thoracostomy. During follow-up pleural fluid cell-block was performed due to continued pleural effusion and reported as carcinoma metastasis. 200 mCi RAI treatment was given after preparation with recombinant thyroid stimulating hormone (TSH). After the comparative PET-CT revealed progression, transthoracic lung biopsy performed and reported as carcinoma metastasis. After these results tyrosine kinase inhibitor (sorafenib) was initiated to the patient. Conclusion: The most common sites of distant metastasis of PDTC are the lungs and bones. It constitutes about 85% of deaths related to the disease. Less than 1% of malignant pleural effusions are associated with thyroid cancers. Pleural fluid thyroglobulin level and immunohistochemical staining may enhance the diagnostic process.
307 - Comparative analysis of five different ultrasonographical risk-stratification systems in the preoperative diagnosis of malignant and benign thyroid nodules. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP870
Background: Our aim was to compare the effectiveness of five different risk-stratification systems using the ultrasonographical features of thyroid nodules in determining malignant histopathology.
Methods: The preoperative ultrasonography (US) features of 6925 nodules of 3030 patients who underwent thyroidectomy between 2007 and 2014 were analyzed retrospectively. The nodules were classified according to Kwak-TIRADS (Thyroid imaging reporting and data system), European Thyroid Association-TIRADS (EU-TIRADS), Korea-TIRADS, American Society of Clinical Endocrinologists (AACE), American Thyroid Association (ATA).1362 nodules (1042 patients) that could be scored in all of these systems were included. Malignancy rate, specificity, sensitivity, positive predictive value (PPV) and negative predictive value were calculated.
Results: In the nodules with high risk scored,malignant histopathology rate were 50%, 27.7%, 32.2%, 29.9%, 31.9% in Kwak-TIRADS, EU_TIRADS, Kore-TIRADS, AACE, ATA, respectively (Table 1). Area under curve (AUC) was higher than 0.5 for all systems (P <0.001,Table 2). When determining optimal cut-off for each system, sensitivity, specificity, PPV, and NPV were about 60%, 75%, 27–30% and 92%, respectively (Table 2). EUTIRADS had significantly lower AUC (corrected P<0.05). AUC of Korea-TIRADS was lower than that of ATA (corrected-P<0.001). AUCs of Kwak-TIRADS, AACE, and ATA were similar and significantly higher than the others (Table 2).
Conclusion: Risk-stratification systems have variable efficiency in predicting malignancy risk since they are operator dependent and require experience in that field. The sensitivity was found to be lower than the previous studies which might be due to retrospective evaluation of US reports rather than real time risk scoring.
Table-1.Distribution of benign and malignant nodules according to riskstratification systems
| Benign (n=1179) | Malignant (n=183) |
| n (%1/%2) | n (%1/%2) |
Kwak-TIRADS | ||
Possibly benign | 137 (97.9/11.6) | 3 (2.1/1.6) |
Low | 774 (91.8/65.7) | 69 (8.2/37.7) |
Intermediate | 61 (82.4/5.2) | 13 (17.6/7.1) |
Moderate | 195 (69.4/16.5) | 86 (30.6/47.0) |
High | 12 (50.0/1.0) | 12 (50.0/6.6) |
EU-TIRADS | ||
Benign | 97 (95.1/8.2) | 5 (4.9/2.7) |
Low | 729 (91.8/61.9) | 65 (8.2/35.5) |
Intermediate | 58 (100.0/4.9) | 0 (0.0/0.0) |
High | 295 (72.3/25.0) | 113 (27.7/61.8) |
Kore-TIRADS | ||
Benign | 129 (94.9/10.9) | 7 (5.1/3.8) |
Low | 787 (92.4/66.8) | 65 (7.6/35.5) |
Intermediate | 57 (81.4/4.8) | 13 (18.6/7.1) |
High | 206 (67.8/17.5) | 98 (32.2/53.6) |
AACE | ||
Low | 187 (96.4/15.9) | 7 (3.6/3.8) |
Intermediate | 729 (91.9/61.8) | 64 (8.1/35.0) |
High | 263 (70.1/22.3) | 112 (29.9/61.2) |
ATA | ||
Bening | 129 (94.9/10.9) | 7 (5.1/3.8) |
Very low | 58 (100.0/4.9) | 0 (0.0/0.0) |
Low | 729 (91.8/61.9) | 65 (8.2/35.5) |
Intermediate | 54 (80.6/4.6) | 13 (19.4/7.1) |
High | 209 (68.1/17.7) | 98 (31.9/53.6) |
1:Row percentage; 2:Column percentage | ||
306 - Frequency of euthyroid sick syndrome before and after renal transplantation in patients with end stage renal disease and its association with oxidative stress. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP869
Aim: Euthyroid Sick Syndrome (ESS) is a thyroid disease appeared in critical and noncritical illnesses. ESS can be seen in patients with end stage renal disease (ESRD). In this study, we aimed to evaluate the frequency of ESS before and after renal transplantation in patients with ESRD, and its association with oxidative stress by evaluating thiol-disulphide levels. Material and Method: In this study, free triiodothyronine (fT3), free thyroxine (fT4) and thyroid stimulating hormone (TSH) levels were recorded before and after renal transplantation in patients with ESRD. ESS was diagnosed in patients with unresponsive TSH to low fT3 and/ or fT4 levels, Thiol and disulphide parameters of patients before and after transplantation were also recorded. Results: One- hundred twenty one patients were included in the study. Of these, 69 (57%) were males and 52 (43%) were females. The mean age was 45±12.61 years. ESS was detected in 39 (32%) of 121 patients. Of 39 patients, 24 (61%) had ESS before transplantation and 15 (39%) after transplantation. Frequency of ESS was 19.8% in patients followed with ESRD. Sixteen of 24 (66.7%) patients with ESS before transplantation reached to normal thyroid functions after transplantation. After transplantation, patients with ESS had significantly higher urea and creatinine (respectively, P = 0.025 and P = 0.009), and lower fT4, fT3, total protein, and albumin (P = <0.001; for all parameters) compared to patients without ESS. Patients with ESS before transplantation had also significantly higher creatinine levels compared to patients without ESS (P = 0.034). Free T4 and fT3 levels were significantly low (P <0.001 for both). Thiol- disulphide levels of 20 patients with ESS at any time compared with 68 patients without ESS. We found that native thiol and total thiol were low significantly in patients with ESS (respectively, P = 0.025 and P = 0.044). Conclusion: Our study is the initial study evaluating the oxidative stress and antioxidation status in etiology of ESS in patients with renal transplantation. Presence of markedly low level of antioxidation in these patients supports the possible role of oxidative stress in etiology of ESS.
305 - Steroid Cell Tumor of the Ovary - A case presenting with hirsutismus. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP865
Introduction: Steroid cell tumors (SCTs) are a rare subgroup of sex-cord tumors of the ovary that account for less than 0.1% of all ovarian tumors. They are classified into three categories based on the cell origin: stromal luteoma, Leydig-cell tumor, and not otherwise specified (NOS). NOS tumors are the most common subtype and comprise the largest proportion of cases (60%).The clinical presentations are not specific, including abdominal pain, distention and bloating. However, the more significant presentations are those associated with the hormonal activity and virilizing properties of the tumor. The cornerstone of SCT-NOS treatment is surgery. Case: A 55-year-old female came to our hospital in November 2020 with months’ history of increasing facial and truncal hair. She also had hypertension and diabetes mellitus. In the medical history of the patient, she had been operated for papillary thyroid cancer, sleeve gastrectomy, total abdominal hysterectomy and left salpingo-oophorectomy 30 years ago. Physical examination revealed obesity (body mass index, 37.3 kg/m2).She had a Ferriman–Gallwey score of 24. Abdominal ultrasound identified a 40 × 20 mm solid, right ovarian mass.Biochemical data shows the levels of folicle stimulating hormone and luteinising hormone were as high as 52.1 U/l and 33.3 U/l, respectively. Serum adrenocorticotropic hormone, cortisol, estradiol, serum prolactin, dihydroepiandosterone sulfate were found within reference intervals.Total and free serum testosterone levels were found to be as high as 450 ng/dl (normal 7–49 ng/dl) and 19.99 (normal<4.2 pg/ml), respectively. Magnetic resonance imaging with contrast confirmed the ultrasound findings and detected no adrenal gland enlargement or tumor.The right salpingooophorectomy was done, and the specimen was sent to our department for histopathological examination. On surgical staging laparotomy, it was found that there was an enlarged (3×3×2 cm) right ovary with both solid and cystic component and normal ovarian contour.Microscopically, mitotic activity 2–3/10, mild atypia, and no significant necrosis. Immunohistochemistry revealed a result of MelanA(+), ER (+), CD56(+), Calretinin (+), Inhibin-α (+), ki-67 (5–6%+). Histological features were consistent with SCTs-NOS type.At post-operative follow-up, her total serum testosterone and serum free testosterone level had gone down to 13 ng/dl and 0.73 pg/ml, respectively. Conclusion: SCTs, NOS, are rare ovarian tumors which can be difficult to diagnose. Careful history and physical examination, in addition to laboratory values and imaging studies, are helpful in making the diagnosis.They are usually benign, unilateral and are characterized by hyperandrogenism and virilization. SCTs should be considered in differential diagnosis among women presenting with symptoms of virilization.
304 - A rare case of glucagonoma presented with high serum amilase and lipase. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP856
Introduction: Glucagonoma is an extremely rare type of functional pancreatic neuroendocrine tumor that is characterized by distinctive clinical manifestations such as diabetes mellitus, weight loss, deep vein thrombosis, and necrolytic migratory erythema which represents the hallmark clinical sign of glucagonoma syndrome. Here, we report the case of a 53-year-old male patient who presented with high amilase and lipase levels. In further investigation a pancreatic tumor was determined and after pancreatic surgery it was diagnosed as glucagonoma. Case: A 53-year-old male patient was examined routinely in cardiology. In the laboratory analysis, amilase and lipase were detected as above the upper limit of normal [amilase: 212 (Normal range: 30–118 U/l), lipase: 224 (Normal range: 12–53 U/l)]. He did not have any symptoms or signs associated with pancreatitis. Glycosylated A1c was 6.5%. In his past history he did not have diabetes mellitus. In the family history, he reported that his mother had diabetes. He referred to our outpatient clinic for prediabetes. Furtherly, 75 gr oral glucose tolerance test was performed. It was evaluated as impaired fasting glucose (0.min glucose: 115 mg/dl, 120.min glucose: 93 mg/dl). In the investigation of pancreatic enzyme abnormalities, abdominal ultrasound was performed. In the ultrasound, Grade 2 hepatosteatosis and a heterogenous weakly hypoechoic solid mass located in proximal pancreatic body which was 20x14.5 mm in diameter were detected. In abdominal MRI, a 21x16 mm mass located in posterior part of the pancreatic body which was mildly hyperintense in T2A and hypointense in T1A images was reported, and in contrasted images the tumor was found as prominent minimally according to parachyme, and had also diffusion restriction. For the investigation of neuroendocrine tumor, Ga-68 DOTA-PEPTIDE PET/CT was performed and it demonstrated a high pathologic Ga-68 enhancement in the pancreatic mass (SUVmax: 21.92). Then, the patient was operated. Distal pancreatectomy and splenectomy was performed. The histopathology was reported as grade 1 glucagonoma. Postoperatively, he had diabetes mellitus, he was under insulin treatment. His postoperative amilase, lipase values were normal. The postoperative glucagon value was 248 (normal range: 25–250 pg/ml). Conclusion: Glucagonoma is a rare pancreatic neuroendocrine tumor. Most common presentation is the skin lesions. Our patient was diagnosed after investigation of biochemical abnormality. He presented atypically as he did not have most typical presentations like most patients in the literature.
303 - A case of pituitary xanthogranuloma diagnosed with diabetes insipidus. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP850
Background: Pituitary xanthogranulomas are extremely rare tumors of the sellar region. A cystic mass lesion was found in the pituitary MRI of our patient diagnosed with central diabetes insipidus (DI). We aimed to present a case who was operated for a pituitary mass and diagnosed with sellar xanthogranuloma. Case presentation: 37-year-old female patient was applied to our outpatient clinic with complaints of polydipsia, polyuria and headache for 8 months. The anterior pituitary hormone levels were in normal. Plasma osmolarity: 291 mOsm/kg, urine osmolarity: 130 mOsm/kg, urine density: 1006 and serum electrolytes were in normal range. Pituitary MRI revealed a cystic mass lesion with prominent hyperintense mucoid content in T1-weighted sequences with a diameter of approximately 10 × 11 mm and completely obliterating the neurohypophysis in the posterior of the adenohypophysis. Also the cystic mass lesion showed expansion towards the posterior suprasellar system. Her visual field examination was found normal. The patient was admitted to our clinic for the water deprivation test. Complete central DI was diagnosed. Desmopressin treatment was started on. The clinic and laboratory findings of DI were improved after desmopressin treatment. The patient was evaluated by neurosurgery department. Transsphenoidal surgery was performed for the mass lesion in the pituitary. The pathology result was reported as sellar xanthogranuloma. Desmopressin therapy was continued in the postoperative period. Clinical and laboratory findings were found normal under desmopressin treatment. Pituitary MRI performed 3 months after the operation, no finding of residual-recurrent adenoma was detected in the sellar region. Conclusion: Sellar xanthogranulomas are very rare seen intracranial tumors. They have not any typical radiological feature. Patients can present with clinical signs such as headache, visual disturbance, vomiting, DI and hypopituitarism.
302 - Rare hypophysis tumor arising in a case with diabetes incipidus: Granular cell tumor. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP852
Introduction: Pituitary gland tumors constitute approximately 10–15% of primary brain tumors, and posterior pituitary tumors are extremely rare. Granular cell tumor (GCT) is a low grade non-neuroendocrine neoplasm. Here, we will present our case who was found to have GCT during follow-up of diabetes insipidus (DI). Case: A 23-year-old male patient applied to our outpatient clinic for routine control. 12 years ago, he was diagnosed with growth hormone deficiency and central hypothyroidism during tests performed for short stature, and used growth hormone and levothyroxine treatments, and it was learned that these treatments were discontinued after puberty, and he had been using desmopressin for partial DI for 10 years. He was using desmopressin 240 mg/day at presentation. His height and weight were 165 cm and 60 kg, his blood pressure was 120/80 mm Hg, and his pulse was 72 beats/min. Systemic examination was normal. Serum Na level was 142 mEq/l, serum osmolality was 291 mOsm/kg, spot urine osmolality was 693 mOsm/kg, and urine density was 1020 (Table 1). On the neurohypophysis lodge, a high-signal lesion area (granular cell tumor?) was observed with magnetic resonance imaging in T1A and T2A series with 1.4 × 1 × 0.6 cm dimensions, which created convexity at the base of the sella contour. When the pituitary images of previous years were examined, it was reported that neurohypophysis was normal in 2010 and 2016, tubular structure showing loss of signal in all sequences in the neurohypophysis (vascular structure?) was observed in 2013, and in 2019, it was determined that a lesion (lipoma?, terotoma?, dermoid cyst?) was detected in the neurohypophysis lodge, which showed suppression (?) in a fat-suppressed sequence of 13 × 7 mm in size, and did not form a distinct opacification pattern in dynamic study. He was evaluated in a multidisciplinary council and follow-up was planned. Discussion: DI was seen in 3–5% of GCT cases. In our case, no tumor was observed on neurohypophysis at the time of diagnosis, but GHT was detected during follow-up. We are of the opinion that periodic pituitary imaging in DI cases may increase the possibility of detecting rare tumors such as GHT.
Na; Sodium, K: Potassium, TSH: Thyroid stimulating hormone, st4: Thyroxine, GH: Growth hormone,
IGF1:Insulin-like growth factor, FSH: Follicle stimulating hormone, LH: Luteinizing hormone, ACTH:Adrenocorticotropic hormone
301 - Two thyrotropin secreting pituitary adenoma cases diagnosed after response to the somatostatin analogue. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP847
Introduction: Pituitary adenomas secreting TSH (TSHoma) are a rare cause of hyperthyroidism. They account for approximately 0.5–3 % of functioning pituitary tumours and much less than 1% of all cases of hyperthyroidism. TSHoma should be considered in all hyperthyroid patients, especially those with diffuse goitre and no extrathyroidal signs of Graves’ disease.
Case 1: A 30-year-old female applied to the internal medicine department with complaints of palpitations, diarrhea, sweating and weight loss. In repeated examinations, high levels of TSH, fT3 and fT4 were detected, TSH, fT3 and fT4 values examined in 3 different centres and again found to be high.The serum sex hormone-binding globulin concentration was slightly elevated. In family screening, no thyroid dysfunction was detected. In pituitary MRI, 5 mm adenoma was detected.The serum α-subunit level was 2.4 ng/ml (normal < 1.2), and the α-subunit/TSH molar ratio (α-subunit ×10/TSH) was 4.3 (normal < 1).We performed an analysis for mutations in the THRB gene; no mutations found. The serum TSH concentration didn’t increase in response to the thyrotropin-releasing hormone, while a fall in serum TSH concentrations was detected in response to administered T3. Since the tests showed discordance, a short course of long-acting (LAR) somatostatin analogue (SSA) was administered. Thyroid function tests returned to normal with LAR-SSA therapy and strengthened the diagnosis of TSHoma. Surgery was planned.
Case 2: A 35-year-old male patient was referred to the endocrinology department when elevated TSH, fT3 and fT4 values were detected in the smoking cessation outpatient clinic. Repeated examinations in the same centre and two different centres showed high TSH, fT3 and fT4 levels. No thyroid dysfunction was found in first-degree relatives.The serum sex hormonebinding globulin concentration was normal,and the serum α-subunit level was 0.7 ng/ml (normal<0.5). In pituitary MRI, 7 mm adenoma was detected. The serum TSH concentration didn’t increase in response to the thyrotropinreleasing hormone,while a fall in serum TSH concentrations was detected in response to administered T3. Since the tests showed discordance,a short course of LAR-SSA was administered. Thyroid function tests returned to normal with LAR-SSA therapy and strengthened the diagnosis of TSHoma. Surgery was planned.
Conclusion: Most TSHomas are detected as pituitary macroadenomas. The presence of a microadenoma on MRI is not specific for a TSH-secreting tumour and can be seen as an incidental finding in 10 per cent of normal individuals. The rutin tests used for the differential diagnosis of TSHoma and Thyroid hormone resistance sometimes may be discordant. In such cases, performing
the LAR-SSA test strengthen the diagnosis.
300 - Hemorragic degeneration after covid-19 infection in microprolactinoma. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP846
Introduction: Pituitary apoplexy is seen in 1.5–27.7% of pituitary adenomas. Common etiologies include hypertension, diabetes mellitus, radiotherapy, contrastenhanced MR, surgery, drugs, anticoagulant, antithrombotic, estrogen, head trauma and pregnancy. SARS-CoV-2 had spread rapidly, and caused COVID-19 pandemic. Although it mainly causes respiratory problems, there may also be extrapulmonary involvement. COVID-19 infection is associated with hemorrhagic complications, cardiac and renal infarction and cerebrovascular hemorrhage. In this report, we present a patient who was followed up with microprolactinoma and developed hemorrhagic degeneration in adenoma after Covid-19 infection.
Case: A 26-year-old female patient was found to have serum prolactin of 94.19 mg/l (4.79–25.3) in the tests performed due to menstrual irregularity and complaints of galactorrhea by provocation. Control prolactin was 104 mg/l, and macroprolactin was negative. Other anterior pituitary hormones, kidney and liver function tests were normal. A 4 × 6 mm microadenoma was detected on pituitary gland in pituitary MRI. Cabergoline 0.5 mg/week was initiated in March 2019 with the diagnosis of microprolactinoma. The pituitary MRI taken in February 2021 revealed a 7 × 5.5 mm lesion in the adenohypophysis with the presece of hemorrhagic degeneration. There were no complaints of severe headache, nausea, vomiting, or visual impairment during system inquiry. Anterior pituitary hormone levels were normal. Medical history showed that she was diagnosed with Covid-19 in September 2020. She used hydroxychloroquine sulfate 2 × 200 mg (5 days) and enoxaparin sodium 2 ×0.6 mg (10 days) and then acetylsalicylic acid for 10 days. It was thought that hemorrhagic degeneration might be due to the antiaggregant/antithrombotic treatment she had received or the Covid-19 infection itself.
Discussion: Case reports of pituitary apoplexy following Covid-19 infection have been presented in the literature. It is unclear whether this infection occurs as a contributing factor to pituitary apoplexy or coincidentally. It is possible that coronavirus infection could cause an acute hemorrhagic infarction of the gland. This risk increases with anticoagulant and antiaggregant treatments used during Covid-19 infection. Although bleeding into adenomas is spesific to macroadenomas, it should be kept in mind that it may also occur with microadenomas.
299 - Mucormycosis in a patient with newly diagnosed diabetes mellitus and diabetic ketoacidosis. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP825
Background: Mucormycosis is an opportunistic fungal infection that can be aggressive and mortal. Diabetic ketoacidosis(DKA) is a risk factor for mucormycosis. We present a case with mucormycosis presenting with newly diagnosed diabetes mellitus and DKA.
Case presentation: A 34-year-old male patient presented with confusion and vomiting. He had no comorbiditiy. On admission the patient was afebrile, hypotensive (85/55 mm/hg) and had tachycardia (120/bpm). Laboratory investigations revealed hyperglycemia (673 mg/dl), severe metabolic acidosis (pH:6.86, bicarbonate:2.6 mmol/l) and urinary ketones. The patient was intubated due to cardiac arrest and followed up in the intensive care unit for 15 days. After that, the patient with newly diagnosed diabetes was admitted to our clinic for blood glucose regulation. During follow up, he described a feeling of swelling in the left half of the face and blurred vision. There was an erythematous appearance on the left eyelid. Diagnostic nasal endoscopy showed widespread crusting filling left nasal cavity and necrosis in the adjacent septum and middle meatus
which was suggestive of mucormycosis. Paranasal sinus CT revealed mucosal thickening in the left frontal sinus, left anterior-posterior ethmoidal cells, sphenoid sinus in the left compartment and in the left maxillary sinus, causing almost complete loss of ventilation. Mucosal thickening was observed in the left compartment of the sphenoid sinus and the ethmoidal cells on the left. Left frontal and left sphenoethmoidal recesses were obliterated. Left precentral fatty tissue and left pterygopalatine fossa, around the sphenopalatine foramen were dirty. Orbital CT was normal. Cranial MRI showed 22 × 10 mm flair hyperintensity accompanied by effacement in the sulcus in left frontal lobe, frontobasal-orbitofrontal level, cortical-subcortical located in the medial part. In this location, frontal bone integrity was not clearly differentiated, and signs of inflammation were observed in the adjacent frontal sinus. The patient was operated urgently. Histopathology confirmed the diagnosis of mucormycosis. Liposomal amphotericin-B treatment was started. The patient was discharged with intensive insulin treatment after five weeks.
Conclusion: Mucormycosis is an invasive and progressive disease which requires immediate diagnosis and treatment including surgical debridement. Although uncontrolled and long standing diabetes is a well-known important risk factor for this opportunistic infection, it is rare to see it in patients with newly diagnosed diabetes. Our case is important in terms of showing that this infection can also occur in newly diagnosed diabetes.
298 - Awareness of normal weight, overweight and obese patients about complications, risk factors and prevention of obesity. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP814
Background: We aimed to determine the awareness of obese, overweight and normal weight patients about the complications, causes and prevention of obesity. Methods: Patients who admitted to our clinic during a four months period were included. Demographical features, familial histories of obesity, smoking, alcohol use, chronic diseases, medications, medical nutrition therapy and exercise habits were determined. Answers of agree, not agree or no idea were obtained for 40 questions regarding the definition, consequences, risk factors and prevention of obesity. Patients were grouped as normal, overweight and obese according to the WHO criteria.
Results: Data of 352 patients (282 female and 70 male) were analyzed. There were 51(14.5%) normal weight, 72 (20.5%) overweight and 229 (65.0%) obese patients. Median ages were 49, 44 and 33 in obese, overweight and normal patients, respectively (P < 0.001). Education level was lower and familial history of obesity was higher in obese patients (P < 0.001). The rates of agreeing that obesity may cause insulin resistance, type 2 diabetes, cardiovascular disease, hypertension, dyslipidemia, fatty liver, sleep apnea, asthma, gastrointestinal problems, depression, mental problems, limitation of movement and mortality varied between 69.60% and 92.61%. Only 130 (36.93%), 138 (39.20%) and 191 (54.26%) patients agreed that obesity is associated with cholelithiasis, pancreatitis and cancer, respectively. The rate of patients who thought that obesity may cause death, sleep apnea and asthma were significantly higher in obese compared to normal weight patients. Approximately half of the patients agreed that obesity in family, eating too much, skipping meals, and engaging in other activities during eating are risk factors for obesity. Rates of agreement about risk factors for obesity were similar in three groups. More than 2/3 of patients agreed with how a healthy diet should be, and believed in the benefit of exercise. The rate of those who agreed that 4–6 meals/day and not to miss snacks are important for a healthy diet was highest in the obese group (72.92%, P = 0.043). There was no significant difference between groups in terms of other questions regarding a healthy diet.
Conclusion: While awareness about some of the obesity associated complications are high, awareness about others such as gall bladder disease, pancreatitis and cancer are low. Obese patients have higher awareness that obesity can cause death, sleep apnea and asthma. The knowledge about risk factors of obesity related with eating habits was relatively low. It is important to raise awareness of both obese and non-obese patients for the prevention and appropriate treatment of obesity.
297 - Post-transplant dyslipidemia in two cases. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP811
Introduction: Lung transplantation was associated with a 32% prevalence of hypercholesterolemia and a 41% prevalence of hypertriglyceridemia. The prevalence of dyslipidemia in liver transplant recipients is 43% and 31% –51%. In this report, we present 2 cases who developed dyslipidemia after transplantation.
Case 1: The blood test of a 73-year-old male patient who had lung transplantation about 3 years ago revealed Triglyceride (TG) 475 mg/dl (<150), LDLCholesterol: 382 mg/dl (<100), HDL 53 mg/dl (>40), Total cholesterol 431 mg/dl (<200) and HbA1C: 8.3. Six months ago, he was diagnosed with diabetes mellitus by his primary physician. He was on everolimus, prednisolone, and mycophenalate sodium therapy, and was referred to us. There were no cutaneous findings related to hyperlipidemia. After the diet and blood sugar regulation, the tests were repeated; TG was 422 mg/dl and LDL was 366 mg/dl. He had elevated liver function test (LFT) levels, and hepatitis panel and liver auto antibodies were negative. Atorvastatin 1×10 mg was initiated on 14/02/2020. TG was 210 mg/dl (<150), and LDL cholesterol level was 123 mg/dl (<100).
Case 2: A 65-year-old female patient underwent liver transplantation from a cadaver on 12/09/2019 due to toxic hepatitis and on 25/09/2019 due to hepatic vein thrombosis after transplantation. Receiving tacrolimus and mycophenolic acid treatments after transplantation, she developed refractory dyslipidemia after the second transplant. Tests performed in February 2020 showed levels
of Triglyceride 474 mg/dl (<150), LDL-Cholesterol 512 mg/dl (<100), Total Cholesterol 815mg/dl (<200) and HDL cholesterol 11 mg/dl (>50). Pravastatin 1 × 40 mg was initiated in February 2020 and intermittent lipid apheresis was performed. In April 2020, ezetimibe 1 × 10 mg was added to her treatment. In May 2020, LDL level was determined 186 mg/dl.
Discussion: Maintaining or improving allograft function after transplantation and reducing cardiovascular risk are main objectives during follow-up. Interventions for dyslipidemia have the effect of reducing cardiac events in clinical studies specific to transplant population.
296 - Comparison of patients with normocalcemic and hypercalcemic primary hyperparathyroidism. Severe hypercholesterolemia with primary sclerosing cholangitis. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP799
Objective: Primary hyperparathyroidism (PHPT) is the most common cause of hypercalcemia. A group of patients who were followed up with a diagnosis of PHPT had normal calcium levels with high parathyroid hormone (PTH) levels. For the diagnosis of normocalcemic PHPT, secondary causes of hyperparathyroidism such as vitamin D deficiency should be excluded. In this study, the data of 318 PHPT patients who were operated were retrospectively analyzed, and biochemical and clinical characteristics of hypercalcemic and normocalcemic patients were compared.
Methods: The data of patients who were admitted to our hospital’s endocrinology clinic between January 2012 and January 2019, diagnosed with PHPT and operated according to guidelines (all symptomatic patients and asymptomatic patients with at least one operation indication) were retrospectively evaluated. A total of 318 patients were divided into two groups as hypercalcemic and normocalcemic according to the corrected calcium level. The two groups were compared according to clinical and biochemical properties.
Results: Female gender was dominant in both groups (P = 0.07). The mean age was similar in both groups (P = 0.36), while it was 54.0 ± 10.3 in the hypercalcemia group, and 55.4 ± 12.8 in the normocalcemia group. As expected, serum corrected calcium (Ca), PTH levels and urinary Ca excretion were higher in the hypercalcemia group (P < 0.01). While phosphorus (P) level was lower in the hypercalcemia group (P < 0.01), urinary P excretion was similar between the two groups (P = 0.77). There was no difference between the two groups in alkaline phosphatase, creatinine, and vitamin D levels. Percentage of localization with preoperative ultrasonography and mean adenoma size were similar. Also, there was no difference in adenoma features (echogenicity, cystic appearance) and localization, thyroid nodules and thyroiditis prevalence on ultrasonography. The positive result obtained on neck MRI and MIBI scanning was similar. There was no difference between the two groups in terms of stone incidence and osteoporosis prevalance (P = 0.72 and P = 0.08, respectively).
Conclusion: In our cohort, corrected Ca and PTH levels and urinary Ca excretion were high in the hypercalcemic group, as expected. But, the phosphorus level was significantly lower in the hypercalcemia group. In the normocalcemic group, the PHPT phenotype was found to be similar to the hypercalcemic group. These findings suggest that the frequency of surgical indications is similar
in normocalcemic PHPT patients to that in hypercalcemic PHPT patients.
295 - Severe hypercholesterolemia with primary sclerosing cholangitis. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP795
Introduction: Hypercholesterolemia may develop due to primary and secondary causes. Diabetes mellitus, hypothyroidism, nephrotic syndrome and liver diseases are among the most common causes of secondary hyperlipidemia. Here, we will present a case with severe hyperlipidemia due to primary sclerosing cholangitis(PSC).
Case: A 36-year-old male patient was admitted to our outpatient clinic due to severe hypercholesterolemia. It was learned in his history that he had increased liver enzymes for 3 years. He was diagnosed with PSC 4 months ago and liver transplantation was planned. The patient was using ursodeoxycholic acid 2x500 mg treatment. On physical examination, blood pressure was 120/70 mmHg, heart rate was 78 beats/minute and he had icteric appearance. Xanthoma, xanthelasma, arcus cornea was not observed. In laboratory tests, AST, ALT, ALP, GGT, total bilirubin, total cholesterol, LDL, triglyceride, VLDL, HDL were 111 U/l, 108 U/l, 1037 U/l, 301 U/l, 17 mg/dl, 574 mg/dl, 499 mg/dl, 348 mg/dl, 70 mg/dl, 5 mg/dl, respectively. The patient had no other comorbid diseases other than PSC. There was no history of early cardiovascular disease or sudden death in family members. It was learned that the patient’s LDL value was 102 mg/dl 5 years ago. The cause of hypercholesterolemia in the patient was considered depending on the PSC. Statin therapy was not considered due to impaired liver function tests. We planned to start cholestyramine 12 grams per day.
Conclusion: PSC is a liver disease with biliary obstruction. Lipid disorder due to biliary obstruction is associated with lipoprotein X (LpX). LpX is a abnormal low density lipoprotein. It is unable to exert negative feedback on the cholesterol synthesis rate limiting enzyme hydroxymethyglutaryl coenzyme A (HMGCoA) reductase. In contrast, the presence of LpX increases the activity of HMG-CoA reductase in the liver with increased hepatic cholesterol synthesis. Patients with biliary obstruction have increased LDL and decreased HDL. Hypercholesterolaemia improves with removal of obstruction or liver transplantation. LDL apheresis, statins and cholestyramine decrease
cholesterol levels in patients with PSC.
294 - Cushing’s syndrome presenting with dilated cardiomyopathy: A case report. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP794
Background: Cardiovascular complications of Cushing’s syndrome (CS) include; hypertension, left ventricular hypertrophy, and myocardial ischaemia. Also, CS can cause structural and functional changes in the heart, leading to dilated cardiomyopathy in rare cases. Here, we present a case with dilated cardiomyopathy related to Cushing’s syndrome.
Case: A 31-year-old male patient applied to the cardiology department with shortness of breath that worsened with exertion for a year. Globally advanced hypokinetic and globally dilated heart was found in echocardiography with ejection fraction (EF) 20%. His medical treatment was arranged by cardiology department and referred to endocrinology clinic due to the 25 kg weight gain in one year, increased appetite and purple striae on the abdomen and shoulder. Laboratory tests revealed that; ACTH was <5 pg/ml, cortisol: 24.3 mg/dl, night cortisol: 24.7 mg/dl. After 1 mg dexamethasone suppression test (DST) and, 2 day 2 mg DST cortisol levels were found 18.9 mg/dl and 31.79 mg/ dl, respectively. Because these findings suggest the CS, abdominal MRI was performed and revealed that a mass lesion (adenoma?) with a smooth contour, 37 × 28 mm in size, showing heterogeneous signal loss in the outer phase in the left adrenal gland. No pathological finding was found in pituitary MRI. With these findings, the patient was diagnosed with adreanal Cushing Syndrome. Viral myocarditis, lupus or autoimmune myocarditis was ruled out by negative
viral respiratory panel, and negative autoimmune panel respectively. Absence of hilar adenopathy excluded sarcoidosis. Cardiac MRI conducted for cardiac exclusion of mixoma and revealed no findings that were consistent with the mixoma. After the exclusion of other reasons of cardiomyopathy the patient was diagnosed with dilated cardiomyopathy. In the control echocardiography 2 months after heart failure treatment, EF was found 40%. Metyrapone therapy was started gradually to lower the risk of surgery by lowering the patient’s preoperative cortisol load. The cortisol level was found to be 17.4 mg/dl, 2 hours after the first metyrapone treatment. 10 days after metyrapone treatment, when the cortisol level decreased by 14.8 mg/dl, left adrenal gland
excision was performed. Postoperative cortisol was found to be 1.8 mg/dl and 3.2 mg/dl. Pathology result was compatible with nodular diffuse hyperplasia.
Conclusion: Dilated cardiomyopathy and left ventricular failure are rare presentations of CS. Since cardiomyopathy can be reversed following successful treatment of Cushing’s syndrome it is important to consider this diagnosis in patients with both heart failure and signs of CS.
293 - A case of non-familial pheochromocytoma presenting one of the identical twin at young age. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP796
Background: Pheochromocytomas are rare tumors originating from chromaffin cells and characterized by excessive catecholamine synthesis. They are usually benign lesions. Hypertension(HT), tachycardia, sweating and headache are frequently observed. We aimed to present a high malignancy suspected pheochromocytoma case diagnosed in a young age female.
Case presentation: A 20-year-old female patient was admitted to the emergency department due
to high blood pressure, tinnitus and headache. The patient was hypertensive (220/110 mmHg) and had tachycardia (130/bpm). For the etiology of HT, renal doppler USG was performed. An extra-renal solid mass lesion (pheochromocytoma?) was reported. She was referred to our clinic. Surrenal MRI revealed a lesion in the left paraaortic area with 40 × 37 mm enhancement in the area corresponding to the adrenal region. 24-hour urinary normetanephrine and metanephrine levels were found 10 times higher than upper limit of the reference range. Laparoscopic partial adenomectomy was performed by the urologist. After surgery, blood pressure was return to normal range without any medication. In histopathology, Ki 67 proliferation index was reported as 20%. Periadrenal adipose tissue invasion, atypical mitosis, lymphovascular invasion and capsule invasion were found positive. Calculated PASS score was reported 6/21 and it was evaluated as high suspicion of malignancy. Genetic analysis (VHL, MEN, SDH) result was negative. The patient had an identical twin. Pheochromocytoma symptoms of the identical twin were not present. In the literature some cases of identical twins which have concominant pheochromocytoma were reported.
We performed pheochromositoma screening tests for identical twin and no pathology was found.
Conclusion: Although pheochromocytoma is most common in the 4th and 5th decades, it can be seen in all age ranges. The majority of patients are sporadic, there are also hereditary forms. Genetic background should be investigated in patients diagnosed with pheochromocytoma at the young age. Although our case was diagnosed with pheochromocytoma at a young age, her genetic tests was not
showed any mutation.
292 - Significant regression of primary adrenal lymphoma after acute steroid replacement therapy: a case with an insufficient initial biopsy. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP788
Objective: There is limited clinical data available on bilateral adrenal masses (BAM). Here we present a case with BAC and adrenal insufficiency. The patient’s lesions disappeared after steroids, re-grew in the follow-up, allowing a biopsy.
Case: A 60-year-old male patient presented with abdominal pain, nausea, and weakness to another hospital. Hyponatremia and hyperkalemia accompanied by hypotension were detected. Abdominal tomography revealed, “irregularly demarcated hyperdense mass lesions, 60 × 44 mm in the right and 75 × 26 mm in the left adrenal.” Upon referral to our hospital, we employed PET-CT, which demonstrated “mass lesions of 49 × 52 × 71 mm in the right and 56 × 57 × 75 mm in the left adrenal as well as pathological hypermetabolism in multiple foci in the skeletal system.” After diagnosing adrenal insufficiency, we initially gave the patients intravenous hydrocortisone, followed by oral maintenance. There were no pathological findings in tuberculosis tests, viral and autoimmune panel, and malignancy screening. Urine and plasma catecholamine and 17-hydroxy progesterone levels were normal. CT-guided biopsy of the adrenal mass revealed fat necrosis. After 45 days, we attempted a repeat biopsy without success due to almost wholly regressed adrenal masses. Also, bone lesions could not be visualized. Adrenal MRI showed “14 mm lesion on the right and, only diffuse thickening on the left adrenal.” A control PET-CT was obtained. “Evident decrease in the size of the adrenal lesions, in addition to the fairly reduced metabolic activity of adrenal masses and bone lesions.” We performed a biopsy from the most active bony lesion; however, it was inadequate. Two months after the initial presentation, he was admitted with abdominal pain. His lesions had progressed. In CT he had, 70 × 41 mm right adrenal mass invading liver and IVC, 56 × 38 mm left adrenal mass, and numerous metastasis in his liver and lungs. Adrenal biopsy, this instance was compatible with “CD20 + B cell lymphoma infiltration.” Patient died of cerebrovascular incident, whilst awaiting biopsy results.
Conclusion: Primary adrenal lymphoma is a rare etiological cause of BAM with only a handful of reported cases. Adrenal lesions vanishing after steroids should raise the suspicion of adrenal lymphoma. The shrinkage of tumors may lead to diagnostic difficulties such as our patient.
291 - Heterozygous 461A> T (p.Asp154Val) Mutation in POR gene in a male case. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP782
Background: Cytochrome P450 oxidoreductase (POR) deficiency is an autosomal recessive steroidogenesis disorder similar to combined deficiencies of 17α-hydroxylase, 17,20-lyase, 21-hydroxylase. POR deficiency (PORD) is a very rare type of congenital adrenal hyperplasia(CAH) characterized by sexual development disorders and skeletal anomalies. We present a case that was evaluated with a prediagnosis of nonclassical CAH and was found to have a heterozygous mutation in the POR gene.
Case report: A 23 years old male patient applied to our clinic with complaint of excessive hair. These symptom had started on her arms and legs at 6 years old, appeared on her back at 8 years old, then spread to all over the body. He has reached his final adult height at about 15 years old. He had no history of chronic illness, his 47 years old mother and 56 years old father were consanguineous. On physical examination, his blood pressure was 120/80mm/hg, height was 161cm, the length of the penis was 9.5cm and testicular volume was 20 ml. Laboratory tests were as follows; glucose 89 mg/dl (70−99), sodium 138 mEq/l (132−146), potassium 4.7 mEq/l (3.5−5.5), cortisol 20.3 mg/dl (5.2−22.4), ACTH 37.8 pg/ml (<46), TSH 1.6 mU/l (0.55−4.78), sex hormone binding globulin 7 nmol/l (10−57), FSH 3.2U/l (1.4−18.1), LH 6.9U/l (1.5-9.3), progesterone 1.26 mg/l (0.28−1.22), total testosterone 383 ng/dl (164−753), dehydroepiandrosteronesulfate 698.72 mg/dl (34.5−568.9), 17-alpha-hydroxyprogesterone (17-OHP) 1.22 ug/l, free testosterone 26.6 pg/ml (15−50), androstenedione 13.5 nmol/l (2.1−10.8). Maximum 17-OHP was 3.36 mg/l after ACTH-stimulation. Abdominal magnetic resonance imaging showed normal adrenal glands. Scrotal ultrasonography was normal. Bone age was 18 years. Genetic testing revealed that the patient was heterozygote for c.461A > T(p.Asp154Val) mutation in exon 5 of POR gene while CYP21A2, CYP17A1, CYP11B1, HSD3B2, STAR genes were normal. Subsequent genetic testing of parents showed that his mother also had POR(NM_000941.3):c.461A > T(exon5) heterozygote mutation, while there was no mutation in his father.
Conclusion: A great number of POR variants affecting more than 130 amino acids in the POR protein have been reported. There is clinical heterogeneity in patients with POR gene mutations, making the diagnosis difficult. Considering that the POR gene mutation shows ethnic differences, we think that the determination of variant cases in our society will clarify its importance in this case in the future
290 - The value of serum thyroglobuline alteration after ultrasonographyguided fine-needle biopsy of suspicious cervical lymph nodes in the diagnosis of metastasis in patients with differentiated thyroid cancer. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, AEP693
Aim: It is known that serum thyroglobulin (TG) can increase after fine-needle biopsy of thyroid nodules. We aimed to determine whether TG is increased after ultrasonography guided fine needle capillary biopsy (FNC) of suspicious cervical LNs in thyroidectomized patients and investigate the
possible association between change in TG and cytology results.
Material and methods: Data of 188 patients who underwent FNC of suspicious cervical LNs were
retrospectively evaluated. Demographical features, radioactive iodine (RAI) treatment status, thyroid-stimulating hormone (TSH), TG, anti-TG antibody and ultrasonography features of LNs were noted. TG levels before FNC (TGb-FNC), after FNC (TGa-FNC), TGa-FNC/TGb-FNC ratio and the number of patients with increased TG were determined. Patients were grouped as benign, nondiagnostic, suspicious for malignancy and malignant according to the cytological results.
Results: The age, gender, clinical diagnosis, history of RAI treatment and TSH levels were similar in different cytological groups. TGa-FNC, Tgb-FNC/Tga-FNC, and rate of patients with increased TG were significantly higher in malignant cytology group than other groups (P<0.001)(Table). The optimal cut-off level of TG increase that was predictive for malignancy was 7.6% with a sensitivity of 73.7% and specificity of 85.2%. TG increase was not associated with age, sex, TSH level, antiTG positivity and US features of LNs while signficantly lower in patients who received RAI treatment.
Among 31 patients with positive anti-TG, TGb-FNC/TGa-FNC, and rate of patients with increased TG were higher in malignant compared to benign and nondiagnostic cytology groups.
Conclusions: Serum TG increment and rate of patients with increased TG after FNC of suspicious cervical LNs were higher in patients with malignant cytology than with all other cytology results both in all study group and in subgroup of anti-TG positive patients. Increase in TG after FNC might be an additional tool for determining LN metastasis.
Table. Demographical, clinical and ultrasonography features and thyroglobulin levels in patients with respect to the cytological results of lymph nodes
Characteristics | Benign (n=124, 66.0%) | Malignant (n=19, 10.1%) | Nondiagnostic (n=38, 20.2%) | Suspicious for malignancy (n=7, 3.7%) | p-value | |
TGb-FNC (mcg/L) | 0.076 (0.012-0.471)1 | 1.283 (0.207-7.931)1,2 | 0.224 (0.036-1.385)2 | 0.161 (0.026-0.998) | <0.001 | |
TGa-FNC (mcg/L) | 0.072 (0.014-0.382)1 | 2.313 (0.437-12.247)1,2,3 | 0.196 (0.037-1.037)2 | 0.071 (0.013-0.375)3 | <0.001 | |
TGa-FNC / TGb-FNC | 1.000 (1.000-1.000)1 | 1.408 (1.068-1.839)1,2,3 | 1.000 (0.824-1.000)2 | 0.821 (0.531-1.000)3 | <0.001 | |
Increased TG | 18 (14.5)1 | 14 (73.7)1,2,3 | 7 (18.4)2 | 0 (0.0)3 | <0.001 | |
Quantitative and categorical variables are summarized by median (IQR: 25th -75th percentiles) and frequency (%), respectively.
1,2,3The same numbers indicates that the corresponding groups are significantly different from each other.
289 - Adherence to levothyroxine treatment and factors related with adherence in hypothyroid patients. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, PEP15.7
Objectives: Adherence to treatment is one of the most important parameters that affect the success of the treatment in hypothyroidism. We aimed to evaluate the use and adherence to treatment and determine the factors that are related to adherence in patients on levothyroxine therapy.
Materials and Methods: Patients older than 18 years old and using levothyroxine for hypothyroidism were recruited. Demographical, sociocultural and clinical statuses of patients were determined. The practices of using levothyroxine and compliance were evaluated through a questionnaire. Thyroid hormones and antibodies were obtained from medical records. Those who answered the frequency of not using/skipping the drug as never/rarely, sometimes and frequently/often were grouped as high, medium and low adherence, respectively. Data of high, medium and low adherence patients were compared.
Results: A total of 335 patients - 282 (84.18%) female and 53 (15.82%) - male were included. Mean age was 47.36±12.50. 330 (98.50%) patients were taking levothyroxine in the morning and 332 (99.10%) were taking fast. The period between the drug and meal was 15 min in 66 (19.88%), 30 min in 170 (51.20%), 45 min in 25 (7.53%), at least 1 h in 63 (18.98%) patients, while 8 (%2.41) patients were taking it just before or during the meal. Among 145 (45.03%) patients who use a medication that may interfere with the absorption of levothyroxine, 66.66% were using it in less than 2 h of levothyroxine. There were 218 (65.08%) high, 98 (29.25%) medium and19 (5.67%) low adherence patients. Drug adherence was not associated with sex, age, marrital and working status, smoking, alcohol use, the cause and duration of hypothyroidism, presence of comorbid disease and thyroid hormones. The rate of patients graduated from primary school was higher in low adherence and rate of patients graduated from university was higher in high adherence groups (P = 0.008). Familial history of thyroid disease was associated with high adherence (P = 0.013).
Conclusion: We showed that drug adherence is medium or low in 34.92% of hypothyroid patients, and education level and familial thyroid disease were related with high adherence. Although majority of patients take levothyroxine at fast, 22.29% eat less than 30 min after taking the drug. In addition, a considerable amount of patients using medications that inhibits the absorption of levothyroxine did not leave required time between two medications. For effective treatment of hypothyroidism, it is important to increase drug compliance and inform patients about hypothyroidism and levothyroxine.
288 - Diabetic euglycemic ketoacidosis in newly diagnosed type 1 diabetes mellitus during A ketogenic diet. - 2021
Uluslararası Bildiriler 23rd European Congress of Endocrinology, 22-26 May 2021, Endocrine Abstracts (2021), Vol 73, PEP15.1
Background: Diabetic ketoacidosis (DKA) is one of the most serious complications of diabetes. It is characterised by the triad of hyperglycemia (blood sugar >250 mg/dl), ketosis and metabolic acidosis (arterial pH <7.3 and serum bicarbonate <18 mEq/l). Rarely these patients can present with blood glucose (BG) levels of less than 200 mg/dl, which is defined as euglycemic DKA.
Case: A 22-year-old female patient applied to the primary care physician with tingling and numbness in the hands. Fasting blood glucose was 205 mg/dl with normal renal and liver function tests in the first laboratory evaluation and then suggested to apply to the endocrinology clinic. After learning about high blood sugar level, she avoided foods containing carbohydrates and followed a ketogenic diet. She is 160 cm tall and 45 kg heavy. The patient referred to the endocrinology clinic with nausea two weeks later. Her plasma glucose level was 86 mg/dl with an HbA1C of%10.3. HbA1C measurement was repeated and confirmed to be high. She was diagnosed with diabetes. Her laboratory assessments revealed an elevated anion gap of 20.9, increased urinary and plasma ketones, and metabolic acidosis. Low hCG values excluded pregnancy The diagnosis of euglycemic DKA was made, and treatment with intravenous fluids and insulin was initiated, then the patient improved.The C-peptide level was 0.42 mg/l (n:0.81-3.85 low normal). Anti-glutamic acid decarboxylase and anti-insulin antibodies were negative, while the anti-islet cell antibody was positive. There was no one with diabetes in her family. She was screened for liver diseases and glycogen storage diseases, and no pathological condition was detected.
Conclusion: We present a type 1 diabetic patient diagnosed with euglycemic DKA. The possible aetiology of euglycemic DKA includes decreased caloric intake, heavy alcohol consumption, the recent use of sodium-glucose cotransporter 2 inhibitors, chronic liver disease and glycogen storage disorders. DKA in pregnancy has also been reported to present with euglycemia. Our patient had euglycemic DKA triggered by the ketogenic diet. Euglycemic DKA can be missed or inadequately treated in patients presenting with euglycemia on initial presentation. Recognising this condition in newly diagnosed patients can also be a challenge for physicians.
287 - Nivolumab induced relapse of graves’ disease: A case report. - 2020
Uluslararası Bildiriler 22nd European Congress of Endocrinology, 5-9 September 2020, Endocrine Abstracts (2020), Vol 70, EP469
Background: Immune checkpoint inhibitors, including anti-programmed cell death-1 (PD-1) antibodies, have become promising treatments for a variety of advanced malignancies. Nivolumab, an anti-PD-1 monoclonal Ab, is an effective treatment of unresectable metastatic melanoma, non-small cell lung cancer, renal cell carcinoma, head and neck cancer, Hodgkin lymphoma, and gastric cancer. These medicines can cause immune-related adverse events (irAEs), including endocrinopathies. Thyroid dysfunction (TD) is a common irAE induced by nivolumab. The TD includes hypothyroidism and thyrotoxicosis, which are generally mild to moderate. The most common endocrine adverse event with anti-PD-1 therapy is hypothyroidism (around 5.9% cases). Thyrotoxicosis is related to destructive thyroiditis in most of the cases. Patients with TgAbs or TPOAbs are prone to develop destructive thyroiditis after initiation of nivolumab treatment. The development of hyperthyroidism owing to Graves’ disease is virtually very rare, with only 4 cases reported so far. Here we aimed to present the 5th case of Graves’ disease after Nivolumab therapy.
Case presentation: A 75-year-old woman with primary malignant urethral melanoma received three courses of nivolumab at a dose of 240 mg every two weeks. Laboratory tests performed before the 4th course due to the patient’ palpitation. Thyroid- stimulating hormone (TSH), free triiodothyronine and free thyroxine level were < 0.015 (normal range [NR]: 0.55-4.78) mU/l, 7.44 (NR: 2.3-4.2) ng/l and 2.4 (NR: 0.89-1.76) ng/dl, respectively. Her thyroglobulin (Tg-Ab) and thyroid peroxidase antibody (TPO-Ab) were both positive, while TSH receptor antibody (TRAb) was negative. Thyroid ultrasonography showed enlargement of both thyroid lobes with low echogenicity and increased vascularity. Thyroid scintigram showed an increased and diffuse uptake. She had been diagnosed with Graves’ disease approximately eight years ago and treated medically. Tg-Ab and TPO-Ab were both positive, and TRAb was negative like now. After medical treatment was over, the patient was euthyroid in follow-up and even before PD-1 treatment.
Conclusion: While antibody positivity often causes destructive thyroiditis, differently caused Graves’ disease in this case. Also, this is the first case-reported that nivolumab therapy induced a relapse of Graves’ Disease.
286 - Nonmedullary hypercalcitoninemia in a hypocalcemic patient: Shoud we look at serum calcitonin level in the differantial diagnosis of hypocalcemia? - 2020
Uluslararası Bildiriler 22nd European Congress of Endocrinology, 5-9 September 2020, Endocrine Abstracts (2020), Vol 70, EP100
Background: Although high levels of calcitonin suggest neoplastic proliferations such as medullary thyroid carcinoma, C cell hyperplasia and some neuroendocrine tumors, systemic diseases and drugs may also elevate calcitonin. Although calcitonin is not as effective as PTH, it has got a role in calcium hemoastasis. Supraphysiological calcitonin level can lead to hypocalcemia.
Case presentation: A 57-year-old male patient was diagnosed with epilepsy with complaints of contraction in the body at the age of 16. Phenytoin therapy was started. He had no epileptic seizures for 13 years. Basal ganglia calcification was detected in brain CT which had been taken when he had muscle contractions while he had been hospitalized for measles in 1992. Calcium: 6.9 mg/dl phosphorus: 5.3 mg/dl albumin: 4.7 g/dl, parathormone: 499 pmol/l (219-659) calcitonin: 145 (0-50) was measured and hypoparathyroidism was diagnosed. Calcitriol and calcium carbonate treatment had been started. In another medical center it was thought that he had pseudohipoparathyroidism, because calcium was normal, vitamin D and parathormone were high while he was not taking calcium replacement treatment. He came to outpatient clinic in 2018 while he was taking 2000 mg oral calcium carbonate treatment. Calcium: 8.9 mg/dl (8.7-10.4) phosphorus:3.5 mg/dl albumin:4.5 g/ dl, parathormone: 41 ng/l (18-80), 25-OH vitamin D: 41 ng/ml (25-80), 1,25OH vitamin D: 24.1 pg/ml (18-64) kalsitonin:117 ng/l (<8.4) was measured. Pseudohipoparathyroidism wasn’t considered with clinical findings. The control calcitonin value was 144, and the highest calcitonin value was 323. Thyroid USG and CEA levels were normal. He had no medullary thyroid carcinoma history in the family. CDKN1B, RET, menin gene analysis were normal. 24-h urinary calcium was 55 mg/day. The heterophile antibody examined by the PEG precipitation method and heterophile antibody-coated tube was negative. No pathological lesions were detected in GA-68 DOTA peptide imaging performed for possible neuroendocrine tumor.
Conclusion: In cases of hypercalcitoninemia, C cell neoplasms should be investigated primarily. In this case, medullary thyroid carcinoma was not considered with the current findings. Due to the coexistence of hypocalcemia and endogenous hypercalcitonemia, the possibility of autosomal dominant hypocalcemia was considered in which calcium sensing receptor activation is playing a role. However, hypocalcuria was interpreted against this possibility. In case of low/normal parathormone in the etiology of hypocalcemia, it is also suggested to measure the calcitonin level.
285 - Diagnostic value of Bethesda system for reporting thyroid cytopathology in patients with prior thyroid surgery - 2020
Uluslararası Bildiriler 22nd European Congress of Endocrinology, 5-9 September 2020, Endocrine Abstracts (2020), Vol 70, AEP973
Background: Fine needle aspiration biopsy (FNAB) and Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) have proven to be the most valuable diagnostic procedure for preoperative discrimination of benign and malignant thyroid nodules. Thyroid surgery may cause regional scarring and some degree of fibrotic process which may result in problems when collecting FNAB samples and evaluating the cellular abnormalities. In this study, we aimed to determine whether the Bethesda classification system in thyroid nodules is reliable in patients with a history of thyroid surgery.
Methods: We retrospectively examined outcomes of 130 patients with 260 nodules who underwent a thyroidectomy for recurrent goiter (Group 1) and compared them with 2821 patients with 5890 thyroid nodules who underwent first thyroidectomy (Group 2) in our center between 2007 and 2014.
Result: Malignancy rate was significantly lower in group B (24 (18.5%) patients) compared to group A (911 (32.3%) patients) (P = 0.016). The most frequent operation indications in group A may explain the hight rate ofmalignancy in this group, that were giant nodule and suspicious cytology results in group B and group A respectively (P = 0.001). Hypothyroidism was significantly higher in group B and result by a hight ratio of gaint nodules (P = 0.001). Although a relationship between giant nodule and higher malignancy rate was reported in previous studies, we did not find a correlation between giant nodules and malignancy rate of patient in group B. Diagnostic value of Bethesda was determined in patients with primary and reoperative thyroid surgery. Benign cytology was considered negative and suspicious for malignancy and malignant cytologies were considered positive. Sensitivity, specifity, PPV, NPV and accuracy of Bethesda classification in patients with primary thyroid surgery were 74.50%, 98.18%, 83.38%, 96.92% and 95.60%, respectively. In patients with reoperative thyroid surgery, sensitivity was 62.50%, specifity was 98.91%, PPV was 71.43%, NPV was 93.38% and accuracy was 97.39%.
Table 1. Diagnostic value of Bethesda classification in patients who underwent primary and reoperative thyroid surgery.
Primary | Reoperative | |||
a (n = 3710) | b (n = 3814) | a (n = 192) | b (n = 199) | |
Sensitivity | 74.50% | 76.37% | 62.50% | 66.66% |
Specifity | 98.18% | 96.09% | 98.91% | 95.79% |
Positive predictive value | 83.38% | 71.61% | 71.43% | 42.86% |
Negative predictive value | 96.92% | 96.92% | 98.38% | 98.38% |
False positive | 16.62% | 28.38% | 28.5% | 57.14% |
False negative | 3.07% | 3.07% | 1.62% | 1.62% |
Accuracy | 95.60% | 93.83% | 97.39% | 94.47% |
Conclusion: FNAB is known to be the most accurate and cost-effective method that provides avoidance of unnecessary surgery in 25% of patients with benign thyroid disease. A lower frequency of malignancy was observed in patients/nodules with reoperative thyroid surgery compared to patients/nodules with primary thyroid surgery in this surgical series. Sensitivity and PPV of Bethesda were affected negatively by previous thyroid surgery. This might be considered in these patients while deciding for a recurrent surgery which has a higher risk of complications.
284 - Severe insulin resistance with cirrhosis: A case report - 2020
Uluslararası Bildiriler 22nd European Congress of Endocrinology, 5-9 September 2020, Endocrine Abstracts (2020), Vol 70, AEP321
Background: Alstrom syndrome is a rare autosomal recessive genetic disorder characterised by vision loss, hearing loss, childhood obesity, insulin resistance and hyperinsulinemia, type 2 diabetes, hypertriglyceridemia, cardiomyopathy, and progressive pulmonary, hepatic, and renal dysfunction. Hyperinsulinemia develops early, and pancreatic islets show beta-cell proliferation, thus suggesting that both insulin resistance and increased insulin secretion might contribute to glucose intolerance. Increased triglyceride levels, steatosis in the liver and pancreas can also amplify the insulin resistance.
Case presentation: A 20-year-old male patient was diagnosed with congenital amaurosis at the age of 6, diabetes mellitus and hypothyroidism at the age of 8, and hearing loss at the age of 9. Then mutations in ALMS1 detected and Alstrom syndrome was diagnosed. No pathology was detected in bone marrow biopsy for pancytopenia in 2015, and follow-up planned. Chronic liver disease and esophageal varices were detected in 2017. He was admitted to our Endocrinology outpatient clinic with high blood sugar. The serum level of FPG, HbA1c, insulin (fasting), and c-peptide were 148 mg/dl, 10.5%, 63.1 mU/l (3-25) and 5.31 mg/l (0.81-3.85), respectively. Anti-GAD, anti-islet antibody and anti-insulin antibody were negative. He was hospitalised for blood glucose regulation. His height was 155 cm and body weight was 55 kg. On admission, he received 15 units/day insulin glargine and 25 units/day insulin aspart. The total daily insulin requirement increased to 216 units and blood glucose was in the range of 150-300 mg/dl. Due to cirrhosis, the recommendation of pediatric metabolic disease doctors was taken, and then metformin and pioglitazone treatment were started while sodium benzoate treatment was continuing. Liver decompensation did not develop at follow-up and insulin requirement gradually decreased to 160 units/day and blood glucose decreased to 90-190 mg/dl.
Conclusion: In diabetes mellitus types with insulin resistance such as Alstrom syndrome, drugs that increase insulin sensitivity such as metformin and glitazone come into prominence. Due to cirrhosis of our case, metformin and pioglitazone treatment was started cautiously. There was a significant decrease in insulin requirement and improvement in the brittle blood glucose profile without any side effects.
283 - The transition range and acceleration from normocalcemia to hypercalcemia in patients with primary hyperparathyroidism: Does it provide a new perspective? - 2020
Uluslararası Bildiriler 22nd European Congress of Endocrinology, 5-9 September 2020, Endocrine Abstracts (2020), Vol 70, AEP235
Objective: Primary hyperparathyroidism (PHPT) is a clinical condition characterized by hypercalcemia-specific symptoms and signs caused by excessive secretion of parathormone. After the evaluation of blood calcium measurements within routine tests, the frequency of hyperparathyroidism increased and there is a marked decrease in the frequency of classical symptoms and signs. Recently, most PHPT cases are detected in the asymptomatic period, and which of these asymptomatic patients will go to surgery, is individually evaluated. In this study, it was investigated whether there is any feature that can be taken into account in the diagnosis and follow-up by considering the calcium course in the period until the development of hypercalcemia.
Methods: The biochemical records of patients who were operated with the diagnosis of PHPT and whose histopathological diagnosis was parathyroid adenoma were reviewed from our database. We evaluated patients who had at least 2 consecutive albumin corrected calcium levels before the time of first hypercalcemia were detected, during the preoperative period. The date when the first hypercalcemia detected, first hypercalcemic value, normocalcemic values and dates, and the intervals between them were recorded. We determined delta change and percentage changes within the patients who had at least 1 year of periyod between normocalcemia values.
Results: In this study,18(94.7%) female and 1(5.3%) male,19 patients with PHPT were included and the mean age was 52.21 ± 10.9. The median time to develop hypercalcemia after the last normocalcemia time was 5 months (0.5-36 months). Median hypercalcemia level was 10.3 mg/dl (10.1-10.9),median for last normocalcemia was 9.8 mg/dl (9.3-10.0). It was found that the development time of hypercalcemia was decreasedas the normal calcium level increased (P = 0.044). A higher hypercalcemic value was found as the time between normocalcemia and hypercalcemia increased (P = 0.049). The course of increase in calcium levels over time was statistically significant (P = 0.0). For the course of changes in normocalcemic values determined in these 19 patients until hypercalcemia was detected, delta change and percentage changes of 12 patients with 2 normocalcemic values at least 1 year intervals before the development of hypercalcemia were calculated.
Conclusion: Recently, some patients with primary hyperparathyroidism who are asymptomatic at the time of admission are treated surgically and some of them are followed up. Individualized treatment is applied in this regard, according to the guidelines some of the patients recommended surgery are followed, some of those recommended for follow-up are also operated. More information about the natural course of untreated primary hyperparathyroidism can help resolve this imprecise situation.
282 - Can serum calcium, phosphorus and parathyroid hormone levels predict histopathological diagnosis in patients with primary hyperparathyroidism? - 2020
Uluslararası Bildiriler 22nd European Congress of Endocrinology, 5-9 September 2020, Endocrine Abstracts (2020), Vol 70, AEP209
Aim: While the histopathological diagnosis is parathyroid adenoma in majority of patients with primary hyperparathyroidism (PHPT),parathyroid hyperplasia, atypical parathyroid adenoma or parathyroid carcinoma can be seen in others. Although it is known that serum calcium (Ca) and parathyroid hormone (PTH) levels are higher in patients with parathyroid carcinoma, there are not any cut-off value for serum Ca, phosphorus (P) and PTH levels defined for different histopathological parathyroid lesions. In this study, we aimed to determine cutoff levels for serum Ca, P and PTH in different histopathological PHPT lesions.
Materials and Methods: The data of 392 patients operated for PHPT were evaluated retrospectively. Patients were grouped as parathyroid hyperplasia, parathyroid adenoma and atypical parathyroid adenoma according to histopathological results. Three way ROC analysis was used to evaluate the performance of serum Ca, P and PTH to determine the three groups. It was shown that Volume Under Surface (VUS) higher than 0.17 was giving information beyond chance. Cut-off levels and correct classification rates (CCR) were calculated when the VUS value was significantly higher than 0.17.
Results: There were 19 patients with parathyroid hyperplasia, 343 with parathyroid adenoma and 31 with atypical parathyrod adenoma. Serum Ca, P and PTH levels were significantly different between groups (P = 0.026, P = 0.003 and P ≤ 0.001, respectively). Serum Ca was significantly lower in parathyroid hyperplasia group compared to other two groups (P = 0.032 and P = 0.036, respectively). Serum Ca was similar in patients with parathyroid adenoma and atypical parathyroid adenoma (P = 0.999) (Table 1). The performance of serum P and PTH to determine groups were not sufficient significantly (P >0.05). In determining the groups, only the VUS value of serum Ca was statistically significantly higher than 0.17 (P = 0.005). The cut-off values for the variable
were determined as C1 = 10.73 mg/dl and C2 = 11.40 mg/dl, respectively.
Conclusion: In this study, we found that serum Ca levels can be predictive for the histopathological diagnosis in patients with PHPT. Serum Ca lower than 10.73 mg/dl, 10.73–11.40 mg/dl and >11.40 mg/dl were determined to predict parathyroid hyperplasia, parathyroidadenoma and atypical parathyroid adenoma, respectively.
Table 1. Serum calcium, phosphorus and parathyroid hormone in patients with primary hyperparathyroidism according to histopathological diagnosis
Parathyroid hyperplasia (n = 19) | Parathyroid adeoma (n = 342) | Atypical parathyroid adeoma (n = 31) | p | |
Calcium (mg/dl) | 10.98 ± 1.31 | 11.39± 0.98 | 11.56± 1.24 | 0.026 |
Phosphorus (mg/dl) | 3.83 ± 2.08 | 2.62 ± 0.69 | 2.35 ± 0.59 | 0.003 |
Parathyroid hormone (pg/ml) | 806.71 ± 923.07 | 229.82 ± 311.67 | 402.54 ± 383.46 | <0.001 |
281 - A new and valuable predictor for the diagnosis of primary hyperparathyroidism: Ca/P Ratio. - 2020
Uluslararası Bildiriler 22nd European Congress of Endocrinology, 5-9 September 2020, Endocrine Abstracts (2020), Vol 70, AEP138
Introduction: Primary hyperparathyroidism (PHPT) is a common endocrine disorder that is characterized by hypercalcemia and elevated or normal levels of parathyroid hormone (PTH). Most PHPT cases are incidentally discovered when routine laboratory analysis reveals hypercalcemia. PHPT should be considered in any person with elevated serum calcium (Ca) levels and no clear evidence of malignancy. Serum phosphorus (P) is low due to the phosphaturic effects of PTH and mostly in the lower half of the normal range. As serum Ca and P are inversely related in PHPT, we examined the diagnostic value of the serum Ca/P ratio in the diagnosis of PHPT.
Method: A total of 364 patients followed at our clinic with a diagnosis of PHPT were retrospectively analyzed. As a control group, we selected 98 patients who attended the clinic in the same time period, presenting serum PTH, Ca and P within the normal range. The main outcome measures were: serum Ca, P, albumin, PTH, 25-OH vitamin D and creatinine. Both patients with normocalcemic PHPT and hypercalcemic PHPT were included. The diagnostic accuracy of Ca/P was investigated using receiver operator characteristic (ROC) curve analysis. The resultant cut-off was verified using the independent set of data containing 100 patients and 50 control cases.
Results: There were 317 (87%) females and 47 (13%) males in patients group, and the mean age of the cohort was 53.9 ± 11.4 years (range: 20–82 ). Ca and PTH were significantly higher in PHPT than in controls (P < 0.0001). The Ca/P ratio was also significantly higher in PHPT than in controls (P < 0.0001). ROC curves analyses identified a cutoff value as 3.23 (mg/dl) for Ca/P ratio with a sensitivity and specificity of 94% and 93%, respectively (P < 0.0001). This cut-off value was confirmed by an independent group of cases (100 PHPT and 50 control cases) with 91% sensitivity and 80% specificity.
Conclusion: Ca/P is a precious predictor for the diagnosis of PHPT and it can be used instead of evaluating serum Ca and P levels solely. As Ca/P ratio is easily accessible and inexpensive, it will be useful for PHPT diagnosis and provide simplicity especially for the practitioners with limited resources.
280 - Are young primary hyperparathyroidism patients differ from older ones regarding clinical and biochemical features? - 2020
Uluslararası Bildiriler 22nd European Congress of Endocrinology, 5-9 September 2020, Endocrine Abstracts (2020), Vol 70, AEP137
Introduction: Primary hyperparathyroidism (PHPT) is a prevalent endocrinologic disease and the most common cause of hypercalcemia. PHPT usually affects the elderly. PHPT younger than 40 years of age is less frequent. In young patients especially for ones younger than 30 years of age, screening for familial syndromes such as MEN 1 and MEN 2A is recommended. However, in most of the cases genetic tests are negative and evidence for other endocrine components are absent. Herein this study we retrospectively evaluated the data of 322 patients with asymptomatic PHPT patients who were operated and compared the biochemical and clinical features of young patients (<40 years old) with older ones.
Method: This study had a retrospective design. We evaluated the data of the patients who admitted to our university hospital’s endocrinology clinics and diagnosed with PHPT between September 2015-may 2018. According to the clinical guidelines all symptomatic patients and asymptomatic ones who had
at least one indication for surgery were operated. There were 346 adenomas belonging to 322 patients in total. The patients were classified into 2 groups regarding age (<40 years or >40 years old as Group 1 and 2, respectively). Two group was compared according to clinical, biochemical and histopathologic features.
Results: There wasn’t any statistically significant difference between groups according to histopathology (adenoma, hyperplasia and carcinoma) (P = 0.065). In both groups there was female predominance, but number of male patients was significantly higher in Group 1 compared to Group 2 (P = 0.004). Serum Ca levels were similar whereas PTH level was higher in Group 1. According to ultrasonographic features, Group 2 had higher prevalence of accompanying thyroid nodules or thyroiditis (P <0.001).Interestingly T scores on femur and total vertebra and prevalence of osteoporosis were similar in between two groups. The percentage of preoperative localization with US and mean size of adenomas were similar. However positive result on MIBI scan was higher in Group 2. median Urinary Ca excretion was higher in Group 1 despite similar vitamin D levels (P = 0.0012).
Conclusion: The phenotype of PHPT in young adults is different from older patients. In our cohort number of male patients, serum PTH, urinary Ca excretion were higher in younger patients.
279 - Severe and long-standing hypocalcemia secondary to denosumab treatment in a patient with postoperative hypoparathyroidism, breast cancer and bone metastasis. - 2019
Uluslararası Bildiriler Endobridge 2019, Antalya, Turkey, 24-27 October 2019, Poster presentation-12.
Introduction: Denosumab is a monoclonal antibody, which is used to prevent bone-related
outcomes in patients with solid tumor bone metastasis and reduces the transfer of calcium from
bone into the blood. It rarely causes severe hypocalcemia as a side effect. Here we present a case of
severe hypocalcemia lasting 8 months after administration of a single dose of denosumab given for
diffuse bone metastasis. The patient’s concomitant surgical hypoparathyroidism has also contributed
to the development of hypocalcemia.
Case: A 57-year-old female patient who underwent left mastectomy for breast cancer in 2002 and
received chemotherapy and radiotherapy was operated for multinodular goiter in 2013.
Histopathological diagnosis was multifocal papillary thyroid carcinoma and it was in complete
remission. In April 2018, she was diagnosed with postoperative hypoparathyroidism and her serum
calcium levels were in normal ranges with calcitriol 0.5 mcg/day and calcium carbonate 1000
mg/day. In December 2018, she was given denosumab 60 mg subcutaneously and capecitabine
treatment due to disseminated bone metastasis of breast cancer detected in 18F-FDG-PET
examination. Although her serum calcium was 9.3 mg/dL a few days before denosumab, four days
after injection her serum calcium was 6.9 mg/dL. Her calcitriol and oral calcium supplementation
doses were increased in course of time in another clinic. At the second month of denosumab, she
was consultated to our clinic due to weakness, tingling in the body and numbness and a serum
calcium was 6.2 mg/dl (8,7-10,4), phosphorus was 4.3 mg/dL (2,4-5,1), albumin was 36 g/L
(32-48) and parathyroid hormone was 28.0 pg/mL (18,5-88) despite treatment with calcitriol 2
mcg/day and oral calcium 5000 mg/day. She was hospitalized and intravenous calcium infusion was
given with oral active vitamin D and calcium supplementation. Since the patient had low calcium
values with calcitriol, treatment was replaced by alphacalcidol. During hospitalization, intravenous
calcium infusions were repeated and oral vitamin D and calcium supplementation doses were
increased. Her serum calcium could be maintained between 7.5-8 mg/dl with high doses of vitamin
D and calcium. She was on 3 mcg/day alphacalcidol, 8000 mg/day calcium carbonate and she had a
serum calcium of 7.6 mg/dl when she was discharged at the 25th of hospitalization. She was
followed weekly and then every 15 days in the outpatient clinic and vitamin D and calcium
supplementation doses were reduced, gradually. Finally at the 8th month of denosumab injection,
the treatment doses of alphacalcidol and calcium carbonate could be reduced to basal levels which
were 0.5 mcg/day and 1000 mg/day, respectively.
Conclusion: Hypocalcemia is a known side effect of denosumab, however it is usually mild. In the
case of coexisting hypoparathyroidism, severe and prolonged hypocalcemia that needs to be treated
with intravenous calcium and very high doses of vitamin D and oral calcium supplementation may
occur.
278 - Parathyroid adenomas with atypical histopathology have also atypical ultrasonography findings. - 2019
Uluslararası Bildiriler Endobridge 2019, Antalya, Turkey, 24-27 October 2019, Poster presentation-11.
Background: It is known that 85-90% of the parathyroid adenomas (PA) are found in usual locations while
5-10% can be located ectopically in the thymic band or mediastineum. PAs are visualized as oval and
hypoechoic lesions generally parallel to the thyroid gland in two dimensional ultrasonography (US) images.
However, adenomas with atypical locations can be in different forms in the three dimentional plane. The
most common form is the bean grain type. In this report we present four cases of atypical PA with different
US features and locations.
Case-1: A 41-year old patient was referred to emergency service with hypercalcemia crisis. His calcium (Ca)
and intact parathyroid hormone (iPTH) levels were 14.24 mg/dl and 735 pg/ml respectively. His biochemical
parameters were shown in table. Since Ca level did not decrease with intravenous hydration and loop
diuretics, hemodialysis was performed and his Ca level decreased to 11 mg/dl. There was no lesion
compatible with PA in his first neck US. Technetium-99m-sestamibi was compatible with PA. No adenoma
was found in the second US evaluation also. But when the US probe was changed from 13-5 MHz to 10-5
MHz and the tissue penetration was also changed, a giant PA isoechoic with the thyroid gland was seen
inferior to the right thyroid lobe starting from the lower end extending to the cervical vertebrae. PA was
removed successfully with minimally invasive procedure (MIP) and the histopathological diagnosis was
atypical PA.
Case 2: A 52-year old woman was referred to our clinic because of hypercalcemia. Her biochemical
parameters were shown in the table. US revealed a hypoechoic lesion (compatible with PA) with
macrocalcific areas, fibrous bands and partial cystic changes in the inferior posterior part of the right thyroid
gland. She underwent MIP and atypical PA was detected histopathologically.
Case-3: A 35-year old woman admitted to emergency clinic due to the hypercalcemia crisis (biochemical
parameters were shown in table). A giant PA lesion in the right thyroid gland starting from the middle part to
the inferior part was detected in neck US. It was iso-hypoechoic and had partial cystic areas. After the
removal of the PA, her Ca level was normalized and histopathologically atypical PA was observed.
Case-4: A 82-year old man was referred to our outpatient clinic due to hypercalcemia. His US finding was
consistent with PA located superior to the right thyroid gland. It was isoechoic and had partial cystic areas.
He underwent MIP and Ca levels decreased to normal levels. The histopathological diagnosis was atypical
PA.
Conclusion: The common US findings of these four atypical PAs were either the anteroposterior diameter
was longer than the transvers diameter (in all of the four cases) or the PA was larger than the longest
diameter of the thyroid gland (case 3 and 4). Our findings suggest that the location and the size of atypical
PAs may also be atypical.
Table. Biochemical features and Technetium-99m-sestamibi results of the patients and sizes of the
parathyroid adenomas and the longest diameter of the thyroid gland
Variables Case 1 Case 2 Case 3 Case 4
Calcium (mg/dl) 14.24 13.4 15.3 12.3
Albumin (gr/dl) 4.82 4.5 4.61 4
Phosphorus (mg/dl) 2 1.9 2.5 1.8
Creatinine (mg/dl) 1.35 0.8 0.75 1.2
Alkaline phosphatase
(IU/L)
66 159 290 132
Parathyroid hormone
(pg/ml)
735 270 998 387
25-hydroxy vitamin D
(µg/L)
16.4 23.3 5.1 8.13
Parathyroid adenoma size
(mm)
Anteroposterior 40 25.8 21 30
Transvers
Longitidunal
18.5
38.7
18.9
33.5
12.9
49.7
25
40
Technetium-99m-
sestamibi scintigraphy
positive positive negative positive
Longest diameter of the
thyroid gland (mm)
40 45 45 35
277 - Severe hypocalcemia and dramatic increase in parathyroid hormone after denosumab in a patient with grade IV renal failure. - 2019
Uluslararası Bildiriler Endobridge 2019, Antalya, Turkey, 24-27 October 2019, Poster presentation-10.
Introduction: Chronic kidney disease-mineral and bone disorder (CKD-MBD) is frequently seen in
advanced stages of chronic kidney disease. These patients are at high risk of fracture. Denosumab,
an injectable human monoclonal antibody with affinity for nuclear factor-kappa ligand, is an
effective treatment for osteoporosis in postmenopausal women and men. In contrary to the
bisphosphonates, the pharmacokinetics and pharmacodynamics of denosumab are not influenced by
the renal function and are being increasingly used for patients having CKD-MBD with low bone
mineral density to reduce the risk of fragility fractures. Hypocalcemia is a known side effect of this
drug along with compensatory increase in parathyroid hormone (PTH). Here, we present a patient
with grade IV renal failure who developed severe symptomatic hypocalcemia and dramatic increase
in PTH following denosumab therapy.
Case: A 84 years old female patient with coronary heart disease, essential thrombocytosis,
hypothyroidism and chronic renal disease was consultated to our clinic for osteoporosis. She had
stage IV chronic renal disease for 7 years. Her serum creatinine, urea, glomerular filtration rate
(GFR), calcium, phosphorus, albumin and PTH were 1,8 mg/dl, 58 mg/dl, 25 ml/min/1.73 m 2 , 9.3
mg/dl, 4.7 mg/dl, 3.4 mg/dl, and 65 pg/ml, respectively. Dual energy X-ray absorptiometry revealed
a femoral neck t score of -3.7 and lumbal vertebra t-score of -3.3. She was given vitamin D 7500
IU/day for 8 days and then denosumab 60 mg subcutaneously. Ten days after injection, her serum
calcium was 6 mg/dl, albumin was 3.6 mg/dl, phosphorus was 2.5 mg/dl and PTH was 669 pg/ml.
She had mild numbness and tingling in her fingers but no other symptoms of hypocalcemia,
however Chvostek and Trousseou signs were positive. She was initially managed with intravenous
calcium and then oral calcium supplementation and calcitriol. One week after therapy serum
calcium was 8 mg/dl, albumin was 3.8 mg/dl and PTH was 569 pg/ml. She was managed as an out-
patient with close monitoring of calcium homeostasis. Three weeks after therapy serum calcium
was 8,4 mg, albumin was 3,8 g/dl, phosphorus was 3,3 mg/dl, and PTH was 380 pg/ml.
Conclusion: Denosumab is increasingly used to prevent skeletal-related events related with
osteoporosis and metastatic bone disease. Hypocalcemia is a known side effect of denosumab but it
is generally mild and can be avoided by simultaneous vitamin D and calcium supplementation.
Patients with a low baseline GFR are at significantly increased risk for developing hypocalcemia.
Clinicians should ensure special attention in recognizing patients at risk of developing this serious
adverse effect, so that prompt treatment and preventive strategies can be implemented.
276 - Poorly differentiated thyroid cancer presenting with thyrotoxicosis and disseminated bone metastasis. - 2019
Uluslararası Bildiriler Endobridge 2019, Antalya, Turkey, 24-27 October 2019, Oral presentation-32.
Introduction: Poorly differentiated thyroid carcinomas (PDTC) are a rare subtype of thyroid
carcinomas that are biologically situated between well-differentiated thyroid carcinomas (WDTC)
and anaplastic thyroid carcinomas. Even a minor poorly differentiated component of only 10% of a
given carcinoma significantly affects patient prognosis. Here we present a 63-year-old female
patient who presented with diffuse bone pain and thyrotoxicosis, and diagnosed with PDTC and
diffuse bone metastasis.
Clinical course: A 63 years old female patient with nodular goitre was suggested thyroidectomy 20
years ago, but she has declined the operation. She presented with back and hip pain which
intensified in the last two months and could not be relieved with nonsteroidal anti-inflammatory
drugs. In laboratory examination she had thyrotoxicosis and methimazole was started. Technetium-
99m scintigraphy revealed a hypoactive nodule in the right thyroid lobe. The sacroiliac magnetic
resonance imaging showed a 45x36 mm lesion in the right half of the sacrum. In 18F-FDG PET
scan, a 65x60 mm lesion with calcifications and necrotic areas filling the right thyroid lobe and
isthmus of the neck, extending into the upper mediastinum at the inferior, narrowing the trachea at
this level, with borders that cannot be clearly distinguished from neighbouring anatomical structures
was observed. Additionally, there were mediastinal lymph nodes and metastatic foci in the right
lung, left scapula, T5 vertebrate, right sacrum, left ischium and right femur. Bone biopsy from the
left scapula resulted in WDTC metastasis. Since her thyroid functions were not normalized despite
60 mg/day methimazole treatment, total thyroidectomy and lymph node dissection were performed
after 3 days of plasmapheresis. Histopathologically, a 60 mm tumoral tissue in the right thyroid lobe
was detected. Approximately 20% of the tumor was composed of poorly differentiated cancer cells
including trabecular, solid and insular pattern. The remaining areas were morphologically WDTC.
There were also capsular and lymphovascular invasion. An additional follicular variant papillary
carcinoma of 3 mm was observed in the same lobe. Four central lymph nodes were excised and all
were reactive. At the 6th day of surgery, her serum TSH was <0.008 uıU/ml (0.55-4.78), free
thyroxine was 0.60 ng/dl (0.89-1.76) and free triiodothyronine was 2.47 pg/ml (2.3-4.2) and
methimazole treatment was stopped. The patient was discharged with radioactive iodine treatment
planned.
Conclusion: PDTC patients have worse outcomes than patients with WDTC. There is no difference
in the outcomes of PDTC and WDTC with poorly differentiated component. In our case;
approximately 20% of the tumor was composed of poorly differentiated cancer cells and at the time
of diagnose patient had bone metastasis without cervical LAP metastasis.
275 - Evaluation of patient satisfaction in an endocrinology and metabolism diseases center. - 2019
Uluslararası Bildiriler 21th European 1. Congress of Endocrinology, 18 - 21 May 2019 Lyon, France, Endocrine Abstracts (2019) Vol 63, P998.
Introduction: In our country, some health institutions are allowed to constitute additional service
buildings/centers in order to increase the accessibility to outpatient services and decrease the
crowdiness in hospitals. We aimed to investigate the satisfaction of the patients evaluated in our
endocrinology and metabolism diseases center-ENDOOTEM (Endocrinology-Nuclear Medicine-
Diabetes-Obesity-Osteoporosis-Thyroid Diagnosis and TreatmentCenter)- which serves as a part of
our university hospital since 2007.
Methods: Patients who were examined in our center between September 2018-January 2019 were
asked to participate in satisfaction survey. ‘Satisfaction surveys application guide’ published by
Ministry of Health of our country, satisfaction survey recommended by ‘American Association of
Family Physicians-AAFP’ and PQ8-18 survey developed in 1994 were modified to create our own
satisfaction survey.
Results: 1387(58.6%) female and 979 (41.4%) male patients completed the questionnaire. The
question of ‘Are you satisfied with our center in general?’ was answered as yes by 1374 (58.1%),
partially by 625 (26.6%) and no by 353 (14.9%) patients. There were 1526 (64.5%) patients who
thought that the doctor spent enough time for his/her illness and 368 (15.6%) patients who thought
he/she partially spent enough time. Whether the doctor was polite and respectful was answered as
yes by 1800 (76.7%), partially by 335 (14.3%) and no by 213 (9.1%) patients. There were 1930
(82.0%) patients who were completely or partially pleased with the attitude of the staff and 1988
(84.5%) patients who stated that his/her personal privacy was taken care of. Waiting rooms were not
enough according to 1406 (59.4%) and not comfortable according to 1140 (48.2%) patients. The
main problems were defined as difficulty of making appointment by 990 (41.8%), waiting for a
long time for evaluation of results by 1056 (44.6%), waiting for a long time for examination dates
by 734 (31.0%), difficulty in transportation and car parking by 573 (24.2%) and not being able to
make appointment for the same doctor by 472 (19.9%) patients. 1695 (72.2%) patients declared that
they wanted to continue the follow-up in our center.
Conclusion: Majority of patients were satisfied with the services, the physicians and the staff
working in our center. However, the difficulty in making appointments and physical conditions
seem to be the most important problems. These results suggest that specialized centers may increase
the quality of health services and the number of such centers should be increased. Nevertheless, it is
important to provide the proper physical conditions before opening a specialized health center.
274 - Addison disease in a patient with familial mediterranean fever. - 2019
Uluslararası Bildiriler 21th European Congress of Endocrinology, 18 - 21 May 2019 Lyon, France, Endocrine Abstracts (2019) Vol 63, P832.
Introduction: Familial Mediterranean Fever (FMF) is an autosomal recessive hereditary disease
characterized by fever and inflammation of serous membranes. The most important complication of
FMF is amyloidosis which has significant role in the prognosis. It is unclear how endocrine system
hormones are affected in FMF. We present adrenal insufficiency in a an FMF patient without
amyloidosis.
Case: A 39 years old male patient who had been diagnosed with FMF at the age of 14 years
admitted to the emergency department with the weeklong complaints of cough, fatigue, fainting and
abdominal pain. He had started colchicine treatment at the diagnosis but was not using it regularly.
He had a personal history of hospitalization in the intensive care unit with the diagnosis of
pericardial effusion and FMF attack 6 years ago. His blood pressure was 80/50 mm/hg, body
temperature was 36.88? ?C. In laboratory examination, his blood glucose was 40 mg/dl, sodium was
133 mmol/l, potassium was 6.1 mmol/l, calcium was 8.2 mg/dl, phosphorus was 3.0 mg/dl and
albumin was 4.0 g/dl. Cortisol and adrenocorticotrophic hormone were 0.326 ug/dl and 324.4
pg/ml, respectively.
He was hospitalized with the diagnosis of adrenal insufficiency and glucocorticoid and
mineralocorticoid therapies were started. 24 hour urine protein excretion was 265.1 mg/day which
was suggestive for lack of renal amyloidosis. The size of the kidneys was normal in the abdominal
ultrasonography. Abdominal magnetic resonance imaging showed aplastic/hypoplastic right adrenal
gland that could not be distinguished and a small left adrenal gland. His complaints regressed with
hydrocortisone, fludrocortisone and colchicine treatments.
Conclusion: The most common cause of adrenal insufficiency in developing countries is
tuberculosis while its most common cause in developed countries is autoimmune adrenalitis. Lack
of proteinuria and presence of hypoplastic adrenal glands were suggestive for the absence of
amyloidosis in our patient. Coexistent FMF and Addison’s disease in a patient might be associated
with the immunopathogenic mechanisms or just a coincidence rather than amyloid involvement of
adrenal glands.
273 - Evaluation of ultrasonographical and cytological features of thyroid nodules in patients treated with radioactive iodine for hyperthyroidism. - 2019
Uluslararası Bildiriler 21th European Congress of Endocrinology, 18 - 21 May 2019 Lyon, France, Endocrine Abstracts (2019) Vol 63, P745.
Aim: Radioactive iodine (RAI) is one of the treatment approaches in Graves and toxic nodular or
multinodular goiter (TNG/TMNG) with low cost and high efficacy. In this study, we aimed to
evaluate ultrasonographical and cytological features of thyroid nodules in patients who were treated
with radioactive iodine for hyperthyroidism years ago.
Methods: Patients who had a history of RAI treatment for hyperthyroidism and had thyroid nodules
that were evaluated with fine needle aspiration biopsy (FNAB) were included in the study.
Ultrasonographical features, and cytological and histopathological results of nodules were obtained
from the records.
Results: There were 27 patients (22 female and 5 male) with a mean age of 59.3±13.5. The
indication for RAI treatment was Graves in 5 (18.6%), TNG/TMNG in 16 (69.2%) and unknown in
6 (22.2%) patients. A total of 48 thyroid nodules were evaluated with FNAB and cytological
diagnosis were benign in 24 (50.0%), nondiagnostic in 15 (31.2%), atypia of undetermined
significance in 5 (10.4%), suspicous for malignancy in 2 (4.2%) and malignant in 2 (4.2%) nodules.
Mean duration between RAI treatment and FNAB was 76.4±63.1 months. Thyroidectomy was
performed in 10 patients and 5 were benign (50.0%) and 5 (50.0%) were malignant
histopathologically. FNAB result was benign in 1 (20.0%), atypia of undetermined significance in 1
(20.0%), suspicious for malignancy in 1 (20.0%) and malignnt in 2 (40.0%) nodules with malignant
histopathology. Ultrasonography features of 31 cytologically/histopathologically benign and 5
cytologically/histopathologically malignant nodules were compared. Rates of nodules with
anteroposterior/transverse diameter ratio higher than 1, solid structure, presence of peripheral halo,
marginal irregularity and microcalcification were similar in benign and malignant nodules
(P=0.303,P=0.684, P=0.829, P=0.973 and P=0.621, respectively). There were 1 (20.0%) isoechoic,
1 (20.0%) hypoechoic and 3 (60.0%) iso-hypoechoic nodules among malignant nodules, while 24
(77.4%) of benign nodules were isoechoic, 3 (9.7%) were hypechoic and 4 (12.9%) were
isohypoechoic (P=0.025). Macrocalcification was observed in 4 (80.0%) of malignant and 10
(32.3%) of benign nodules (P=0.042).
Conclusion: In patients treated with RAI due to hyperthyroidism, thyroid nodules with suspicious
ultrasonography features, particulary hypoechoic appearence and presence of macrocalcification,
should be evaluated with FNAB irrespective of the period after RAI treatment. Atypia related with
previous RAI treatment might cause diagnostic problems in cytological evaluation.
272 - Discordance in biochemistry and ultrasonography: Nonsecretory parathyroid adenoma. - 2019
Uluslararası Bildiriler 21th European Congress of Endocrinology, 18 - 21 May 2019 Lyon, France, Endocrine Abstracts (2019) Vol 63, P503.
Aim: Although nonsecretory parathyroid carcinoma is relatively more frequent, nonsecretory
parathyroid adenoma was also reported. It is thought to precede functioning parathyroid adenoma.
Case report: An iso-hypoechoic 6.5x9.5x16.1 mm thyroid nodule with irregular borders in the
superior-posterior part of right thyroid lobe was observed in ultrasonography in a 44-year-old
female euthyroid patient. Fine-needle aspiration (FNAB) biopsy resulted with non-diagnostic
cytology (degeneration of follicular epithelial cells, colloidal material). A second FNAB was
recommended but she admitted five years later. There was subclinical hypothyroidism with positive
thyroid autoantibodies and normocalcemia in laboratory examination. The nodule in the superior-
posterior part of right thyroid lobe was well circumscribed and hypoechoic with diameters of
5.4x13.2x18.1 mm. The ultrasonographical apperarence was found to be suspicous for an
intrathyroidal parathyroid adenoma. Serum calcium was 8.99 mg/dL, albumin was 4.6 g/dL,
parathyroid hormone was 70.22 pg/mL and 25-OH Vitamin D3 was: 6.52 ng/mL. Parathyroid
hormone decreased to 37.94 pg/mL after replacement of vitamin D. The lesion was evaluated with
FNAB and the cytological result was again nondiagnostic (small amount of colloidal material, a few
epithelial cells). Parathyroid hormone washout was >5000 pg/mL in fine-needle aspiration fluid.
24-hours urinary calcium excretion was 210 mg. In Tc99m-sestamibi SPECT/CT revealed persistent
activity at superior-posterior part of upper pole of the right thyroid lobe. There was increased
echogenity compatible with crystalloid in urinary system ultrasonography. Z score was within the
expected range for age in bone mineral density. Surgical excision of the lesion was performed and a
parathyroid adenoma was confirmed histopathologically.
Conclusion: Parathyroid hormone washout should be considered in a lesion with suspicion of
intrathyroidal parathyroid adenoma even when primary hyperparathyroidism can not be shown
biochemically. If surgery is not performed, patients should be followed for possible development of
primary hyperparathyroidism.
271 - Selective arterial calcium stimulation test in two cases with occult insulinoma . - 2019
Uluslararası Bildiriler 21th European Congress of Endocrinology, 18 - 21 May 2019 Lyon, France, Endocrine Abstracts (2019) Vol 63, P454.
Introduction: 80-90% of insulinomas are smaller than 2 cm, equally located in the head, body and
tail of pancreas. Computer tomography (CT) is 75%, magnetic resonance imaging (MRI) is 55-
90%, endoscopic ultrasonography (EUS) is 85-95% and selective arterial calcium stimulation test
(SACST) is 95-100% sensitive in the diagnosis of insulinomas. Here, we presented two cases of
insulinoma which could not be located by conventional methods and evaluated with SACST.
Case 1: A 29-year-old male who described hypoglycemic symptoms especially after exercise in the
last 4 months was admitted to the hospital for a prolonged fasting test. At the 8th hour of the test,
laboratory results were as follows; blood glucose 36mg/dl, insülin 21 uIU/dl, c-peptide 4 ng/dl,
proinsulin 22 pmol/l and cortisol 18 ug/dl. Blood ketone and anti-insulin antibody were negative.
No pathology was observed in the abdominal CT and EUS. Abdominal MRI revealed a 10 mm
diameter nodular lesion in the posterior medial of the stomach which was suspicious for insulinoma.
It was seen only in T2A sequence in the venous phase in contrast-enhanced examination. Galium-
68 Dotatate scintigraphy showed no involvement in the pancreas. SACST was performed. A ten-
fold increase in insulin levels was observed in the splenic artery and distal pancreatectomy was
performed.
Case 2: A 41-year-old woman who had episodes of hypoglycemia for 3-4 months was referred with
a pre-diagnosis of insulinoma. The patient underwent a prolonged fasting test. At the time of
hypoglycemia (blood glucose 45 mg/dl), serum insülin was 7.8 uIU/dl, c-peptide was 2.2 ng/dl,
proinsulin was 8 pmol/l and, serum ketone and anti-insulin antibody were negative. There was no
contrast enhancement in the pancreas in the abdominal MRI, but a suspicious hyperintense area of
10 mm diameter was seen in T2A sequence. There was no pathology in abdominal CT and EUS. In
SACST, a five-fold increase in insulin levels was detected in the mesenteric artery which was
suggestive for an insulinoma lesion in the head of pancreas. Surgical excision was recommended
but the patient refused.
Conclusion: Although the biochemical diagnosis of insulinomas are usually not complicated, the
localization might be problematic. Because of the low sensitivity of non-invasive methods in tumors
smaller than 2 cm, invasive methods can be used for the localization like in our cases.
Table 1: 29 year-old man patient’s(case 1) selective arterial calcium stimulation test results
Gastroduodenal
artery
SMA (superior
mesenteric
artery)
Splenic artery Gastric artery
0.second 22,51 uIU/ml 3,31 uIU/ml 2,014 uIU/ml 31,83 uIU/ml
20.second 25,58 uIU/ml 3,88 uIU/ml 19,8 uIU/ml 17,18 uIU/ml
40.second 28,22 uIU/ml 4,42 uIU/ml 33,42 uIU/ml 23,34 uIU/ml
60.second 19,23 uIU/ml 6,24 uIU/ml 23,53 uIU/ml 23,7 uIU/ml
Table 2: 41 year-old woman patient’s(case 2) selective arterial calcium stimulation test results
SMA Proximal splenic
artery
Gastroduodenal
artery
Distal splenic
artery
0.second 17,54 uIU/ml 21,54 uIU/ml 19,8 uIU/ml 20,69 uIU/ml
20.second 18,49 uIU/ml 30,37 uIU/ml 20,01 uIU/ml 15,5 uIU/ml
40.second 84,93 uIU/ml 21,22 uIU/ml 20,52 uIU/ml 16,83 uIU/ml
60.second 110,3 uIU/ml 24,03 uIU/ml 22,36 uIU/ml 20,24 uIU/ml
270 - The Effect of Ramadan fasting on thyroid hormone levels in patients on levothyroxine treatment. - 2019
Uluslararası Bildiriler 21th European Congress of Endocrinology, 18 - 21 May 2019 Lyon, France, Endocrine Abstracts (2019) Vol 63, P380.
Aim: Contradictory results in limited number of studies were reported about the effects of Ramadan
fasting on thyroid hormones. We aimed to evaluate the thyroid functions in Ramadan, and compare
late evening or pre-sahour use of levothyroxine in patients being treated for hypothyroidism.
Methods: Patients taking levothyroxine for hypothyroidism who were seen in the last one week
before Ramadan (8-15 May 2018) and had normal thyroid functions were recruited. Patients were
offered to take levothyroxine at 22.30-23.00 pm before sleep (Group-1) or between 01:30 and
03:00 am at least 30 min before sahour (Group-2).
Results: Basal thyrotophin (TSH) was 2.01? ?1.05 mIU/ml and significantly increased at the end of
Ramadan (3.09? ?3.38 mIU/ml, P=0.008). Free-triiodothyronine (FT3) decreased while free-
thyroxine (fT4) increased (P<0.001, P=0.028). Eighteen patients were in Group-1 and 44 were in
Group-2. There was unsignificant increase in TSH and FT4 in Group-1 (P=0.160, P=0.425), while
both increased significantly in Group-2 (P=0.022, P=0.008). FT3 decreased in Group-1 and 2
(P=0.016, P<0.001). At the end of Ramadan, TSH increased in 39(%63.9), decreased in 22
(%36.1) and did not change in 1 patient. Anti-thyroid peroxidase antibody was positive in 65.5% of
patients with increased TSH and in 35.3% of patients with decreased TSH (P=0.047).
Conclusion: Although mean TSH increased significantly,about one third of patients had lower TSH
indicating for the need to evaluate every patient individually and follow closely during this month.
Use of levothyroxine in late evening seems to maintain more stable thyroid hormones compared to
pre-sahour. Clinical studies with larger sample sizes will be helpful to determine the optimal time
for levothyroxine use during Ramadan.
269 - Can urinary iodine be used in the diagnosis and follow up of subacute thyroiditis? - 2019
Uluslararası Bildiriler 21th European Congress of Endocrinology, 18 - 21 May 2019 Lyon, France, Endocrine Abstracts (2019) Vol 63, P375.
Introduction: Subacute thyroiditis is an iflammatory disease of the thyroid gland characterized by
pain, tenderness and swelling in the neck. Less frequently, it may present with painless or silent
thyroiditis that occurs spontaneously or in the postpartum period. In a few studies in the literature,
urinary iodine was reported to be high in patients with postpartum thyroiditis, but it was not
evaluated in patients with subacute thyroiditis. We aimed to evaluate urinary iodine in patients with
subacute thyroiditis and determine whether it might have any role in the differential diagnosis.
Materials and methods: Patients diagnosed with subacute thyroiditis between April 2018 and
January 2019 were included in the study. Patients younger than 18 years old, with a history of
exposure to iodinated contrast media and pregnant or lactating women and patients with postpartum
thyroiditis were excluded. Demographic features, thyroid functions, thyroid autoantibodies, serum
thyroglobulin, erhytrocyte sedimentation rate (ESR), C-reactive protein (CRP), urinary iodine,
thyroid ultrasonography and Tc99m pertechnatate scintigraphy results were evaluated.
Results: There were 23 patients (16 female and 7 female) with a mean age of 38.65? ?7.99. At the
time of diagnosis, median serum thyrotrophin was 0.140 mIU/mL (minmax: 0.001-0.25) (normal
levels: 0.27-4.2 mIU/mL), mean serum free triiodothyroxine and free thyroxine were 8.29? ?3.53
pg/mL (normal levels: 1.8-4.6 pg/mL) and 3.56? ?1.34 ng/dL (normal levels: 0.9-1.7 ng/dL),
respectively. There was 1 (4.3%) patient with positive antithyroid peroxidase and 6 (26.1%) patients
with positive antithyroglobulin. Median serum thyroglobulin was 116 ng/mL (min-max: 2.7-500)
(normal levels: 0-78 ng/mL), mean ESR was 52.24? ?25.47 mm and median CRP was 63 mg/L (min-
max: 4.2-188) (normal levels: 0-5 mg/L). Ultrasonographically, thyroiditis was observed in 22
(96.7%) patients and 5 (21.7%) patients had thyroid nodules. Median urinary iodinewas 441 mcg/L
(min-max: 255-1843) and it was higher than 250 mcg/L in all patients. Thyroiditis was controlled
with nonsteroidal antiinflammatory drugs and beta blockers in 13 (54.5%) patients, while additional
corticosteroid treartment was required in 10 (45.5%) patients.
Conclusion: In patients with subacute thyroditis, urinary iodine was very well above normal limits.
This might be helpful in the differential diagnosis and follow up of the disease. While, high iodine
levels may be a consequence of thyroid follicle epithelial cell damage, the possibility of being an
etiological factor should not be ignored. Large-scale prospective studies are required to determine
the role of iodine in subacute thyroiditis
268 - The frequency of confirmed primary hyperaldosteronism in patients with high aldosteron renin ratio. - 2019
Uluslararası Bildiriler 21th European Congress of Endocrinology, 18 - 21 May 2019 Lyon, France, Endocrine Abstracts (2019) Vol 63, P22.
Introduction: The aldosterone-to-renin ratio (A/R) is the most frequently used screening test for
primary hyperaldosteronism (PH) and a confirmation test is recommended when it is high.We
aimed to determine the frequency of PH in patients with high A/R and investigated possible clinical
features that might help to prevent unnecesary confirmation tests.
Method: Patients who underwent saline infusion test because of high A/R (>3.8) were
retrospectively reviewed. PH was diagnosed in patients with plasma aldosteron >10 ng/dl after 4
hours of saline infusion. Patients with postinfusion aldosteron level between 5-10 ng/dl and with <5
ng/dl were defined as indeterminate and not to have PH, respectively. Patients with and without PH
were compared.
Results: There were 38 patients (27 female and 11 male) with a mean age of 55.18? ?10.13. Mean
serum potassium (K) was 4.01? ?0.69 mmol/l and aldosteron was 30.24? ?14.61 ng/dl. Median renin
and A/R were 2.015 ng/l and 12.913, respectively. After saline infusion test, the diagnosis of PH
was confirmed in 17 (43.6%) and excluded in 11 (28.2%) patients. Indeterminate results were
obtained in 10 (25.6%) patients. There were 9 female and 8 male patients with PH, while all 11
patients without PH were female (P=0.007). 16 (94.1%) patients with PH and 7 (63.6%) without PH
were hypertensive (P=0.040). The age, presentation, adrenal imaging findings, sodium and renin
were similar in patients with and without PH. Mean serum K were 3.57? ?0.65 mmol/l and 4.31? ?051
mmol/l in patients with and without PH, respectively (PZ0.003). Mean aldosteron and median A/R
were higher in patients with PH, however the differences were not statistically significant [For
aldosteron; 36.67? ?15.38 ng/dl vs 25.14? ?13.02 ng/dl, P=0.050, for A/R 16.27 (4.90-264.50) and
7.36 (3.97-53.84), P=0.051]. Median aldosteron after saline infusion was 19.40 ng/dl (10.26-64.35)
in patients with PH and 3.70 ng/dl (1.50-4.83) in patients without PH (P<0.001).
Conclusion: Confirmation of PH in less than half of patients with high A/R is suggestive for high
false positivity of this screening method. It may be rational to repeat measurements before
confirmation tests in women, patients without HT and without hypokalemia. However, male sex,
presence of HT and hypokalemia seem to be stronger clinical findings that requires confirmation
tests in patients with
high A/R.
267 - Awareness, treatment rates and compliance to treatment in patients with serum LDL cholesterol higher than 250 mg/dL, and possible, probable and definite familial hypercholesterolemia. - 2019
Uluslararası Bildiriler 21th European Congress of Endocrinology, 18 - 21 May 2019 Lyon, France, Endocrine Abstracts (2019) Vol 63, GP47.
Aim: Familial hypercholesterolemia (FH) is an autosomal dominant genetic disease characterized
by increased levels of low density lipoprotein cholesterol (LDLchol). Despite relatively high
prevalance and significant association with increased mortality, the awareness of physicians and
patients is low and it is an underdiagnosed and undertreated disease. We aimed to detect patients
with FH and determine treatment status and compliance.
Materials and methods: Patients >18 years old and have a serum LDL-chol? ?250 mg/dL between
January 2010-December 2016 were identified from the database of our hospital. A survey was
performed by reaching patients via phone. Demographic features, smoking status, use of alcohol,
exercise, presence of cardiovascular disease (CVD), use of medication for dyslipidemia, CVD and
high cholesterol levels in the family were questioned. Patients with a serum
thyrotrophin10? ?mIU/mL, patients with glomerulonephritis and nephrotic syndrome, patients with
high liver enzymes and patients with serum triglyceride >400 mg/dL were excluded. DUTCH lipid
diagnostic criteria was used to classify patients.
Results: LDL-chol was ? ?250 mg/dL in 1918 measurements. When repeated measurements were
excluded, 1365 patients were identified. Patients that could not be reached by phone and who
refused to interview were excluded and data of 367 patients were analyzed. There were 248 (67.6%)
female and 119 (32.4%) male patients and mean age was 50.5? ?11.66. LDL-chol was ? ?330 mg/dL in
50 (13.6%) and 250-329 mg/dL in 317 (86.4%) patients. Mean DUTCH score was 6.36? ?1.63. 40
(10.9%) patients were classified as definite, 181 (49.3%) as probable and 146 (39.8%) as possible
FH. Among patients with definite or probable FH, 84 (38.0%) had CVD. DUTCH scores were
8.09? ?1.54 and 6.74? ?1.31 in patients with and without CVD, respectively. Considering all patients,
42% were taking medication for dyslipidemia. Among 213 patients that were not on antilipidemic
treatment, 162 (76.1%) stated that medication was never recommended previously, 30 (14.1%) had
stopped medication him/herself and 21 (9.8%) had stopped medication with the advice of the
physician. 49 (58.3%) definite or probable FH patients with CVD was taking antilipidemic
treatment.
Conclusion: A significant proportion of patients with LDL-chol? ?250 mg/dL were not taking
antilipidemic drugs and other cardiovascular risk factors were not under control. Similar with many
other countries, diagnosis and treatment rates of FH patients were very low in our country. Further
national studies are required to increase awareness of the disease in both physicians and patients
266 - Evaluating effects of thyrotrophin receptor antibody positivity on cytology and histopathology in patients with graves disease. - 2019
Uluslararası Bildiriler 21th European Congress of Endocrinology, 18 - 21 May 2019 Lyon, France, Endocrine Abstracts (2019) Vol 63, GP261.
Aim: It has been reported that thyrotrophin receptor antibody (TRAb) is associated with frequency
and aggressiveness of thyroid cancer in patients with Graves disease (GD). However, there is not
any data regarding the effects of TRAb on cytology and histopathology results of patients with
nodular GD. Thus, the aim of the present study is to evaluate the effects of TRAb on cytology and
histopathology results in patients with nodular or multinodular thyroid disease on the basis of GD.
Materials and Methods: Clinical data of patients with GD who had thyroidectomy and
preoperative TRAb levels were reviewed retrospectively. The cytology and histopathology results
of 548 nodules from 598 patients with GD were evaluated for the present study.
Results: Of 598 patients, 189 (31.6%) were men and 409 (68.4%) were women. However 352
patients did not have nodular disease on preoperative thyroid ultrasound, 74 had only one nodule
and 172 had ≥2 nodules. 517 (86.5%) patients had benign and 81 (13.5%) had malignant final
histopathology. In malignant group, 77 (95.1%) patients had papillary throid carcinoma, 2 (2.5%)
had follicular thyroid carcinoma, 1 (1.2%) had thyroid tumor of uncertain malignant potential, and
1 (1.2%) had hurthle cell thyroid carcinoma. However, TRAb was detected as positive in 359 (60%)
patients, it was found as negative in 239 (40%) patients. There were 185 nodules in TRAb positive
group and 363 nodules in TRAb negative group, and there was no significant difference in cytology
results between groups (p=0.181) (Table 1). Malignancy was detected in 48 (13.4%) and 33
(13.8%) patients with TRAb positive and negative patients, respectively (p=0.878), and there was
not any difference in histopathology results between groups (p=0.161) (Table 1). Furthermore, there
was no difference in features of carcinoma such as capsular, vascular, and lymphatic invasions
between TRAb positive and negative groups (p>0.05).
Conclusion: In the present study, it was found that malignancy rate was similar in TRAb positive
and negative patients. Contrary to literature, TRAb positivity was not associated with increased
malignancy rate and also had no effect on cytology and histopathology results in patients with GD.
Table 1. Comparison of the cytology and histopathology results of Thyrotrophin receptor antibody
positive and negative patients with Graves Disease
TRAb Positive TRAb Negative p
Cytology (n,%) n=185 n=363
Nondiagnostic 52 (28,1) 81 (22,3) 0,181
Benign 113 (61,1) 258 (71,1)
Atypia of undetermined
significance/ Follicular
lesion of undetermined
significance
13 (7,0) 19 (5,2)
Follicular neoplasia/
Suspicious for follicular
neoplasia
1 (0,5) 1 (0,3)
Suspicious for malignancy 4 (2,2) 3 (0,8)
Malignant 2 (1,1) 1 (0,3)
Histopathology (n,%) n=48 n=33
Papillary thyroid carcinoma 47 (97,9) 30 (90,9) 0,161
Follicular thyroid carcinoma 0 2 (6,1)
Thyroid tumor of unceratin
malignant potential
0 1 (3,0)
Hurthle cell thyroid
carcinoma
1 (2,1) 0
265 - Are clinicopathological features of isthmic thyroid nodules different from nodules located in thyroid lobes? - 2019
Uluslararası Bildiriler 21th European Congress of Endocrinology, 18 - 21 May 2019 Lyon, France, Endocrine Abstracts (2019) Vol 63, GP255
Aim: Although thyroid nodules located in isthmus were less frequent, papillary thyroid cancer in
this location was reported to be more aggressive in some studies. Our aim was to evaluate
hormonal, ultrasonographic, and cytopathologic features of nodules located in isthmus (isthmic
nodules).
Material and methods: Data of patients who underwent thyroidectomy between 2006-2014 were
reviewed retrospectively. Hormonal, ultrasonographic, and cytopathologic features of patients with
isthmic and with lober (non-isthmic) nodules were compared.
Results: Patients with isthmic nodules (Group-1) and non-isthmic nodules (Group-2) consisted of
260 and 2171 patients, respectively. Age and gender distributions were similar. AntiTg positivity
was higher in Group-1 (28.6% vs 21.2%; P=0.018). Subsequently, 268 isthmic (10.7%) and 5347
non-isthmic (89.3%) nodules were compared. Although ultrasonographical features such as
presence of microcalcification and halo, nodule diameters, echogenicity, texture, margin, and
vascularity were similar between groups, macrocalcification rate was lower in isthmic nodules
(19% vs 27%; P=0.004). Furthermore, cytologic results were also similar. However, malignancy
rate was lower in isthmic nodules (6.0% vs 11.4%; P=0.006), type of thyroid cancer was similar in
isthmic and non-isthmic nodules. When malign isthmic (n=16, 2.6%) and malign non-isthmic
nodules (n=605, 97.4%) were compared, diameter and type of tumor, lymphovascular and capsular
invasion, extrathyroidal extension and multifocality rates were statistically insignificant. Malign
isthmic nodules (n=16, 6%) had smaller size [10.05(4.00-34.50) mm vs 20.05(8.40-74.10)mm;
P=0.002], higher hypoechogenity (31.2% vs 5.6%, P<0.001) and exophyticity rates (28.6% vs
4.9%; P=0.007) compared to benign isthmic nodules (n=251, 94%).
Conclusion: Although isthmic nodules had lower malignancy rate compared to non-isthmic ones,
histopathologic features were similar in isthmic and non-isthmic nodules. Relatively small,
hypoechoic, and exophytic nodules located in isthmus should be evaluated immediately for
malignancy.
264 - Characteristics of hypertensive patients in a population with type 2 diabetes. Results from the Turkish Nationwide SurvEy of Glycemic and Other Metabolic Parameters of Patients with Diabetes Mellitus (TEMD Hypertension Study). - 2018
Uluslararası Bildiriler 18th International Congress of Endocrinology/53rd SEMDSA Congress, Cape Town, South Africa. 1-4 December 2018. Abstract ID 1004.
263 - Is anti thyroid peroxidase positivity protective against thyroid cancer in Graves disease? 41st Annual Meeting of the European Thyroid Association, Newcastle upon Tyne, UK. - 2018
Uluslararası Bildiriler 15-18 September, 2018 . P1-04-33.
ABSTRACT
Aim: Anti thyroid peroxidase (AntiTPO) and antithyroglobulin (AntiTg) Ankara Yildirim
Beyazit University, School of Medicine, Endocrinology and Metabolism Diseasesare known to
be positive in 75-90% and 35-50% of patients with Graves disease, respectively. Although
studies investigating the association between thyroid cancer and Hashimoto thyroiditis (HT) -in
which AntiTPO is an important hallmark of the disease- reported controversial results, studies
showing higher risk in HT outweigh. However, the association between AntiTPO and thyroid
cancer in patients with Graves disease was not studied. We aimed to investigate whether
AntiTPO or AntiTg positivity have any effect on malignancy risk in these patients.
Methods: Graves patients operated in our center was recruited for the study retrospectively. The
clinical features, operation indications and thyroid autoantibodies (AntiTPO, AntiTg and TSH
receptor antibody) were recorded. Patients were grouped as benign and malignant according to
histopathological diagnosis.
Results: Data of 602 patients were analyzed. There were 410 (%68.1) female and 192 (%31.9)
male patients with a mean age of 43.65±12.69. Preoperative ultrasonography revealed no nodule
in 286 (%47.5), single nodule in 63 (%10.5) and multiple nodules in 253 (%42.0) patients.
There were 400 (66.4%) patients with positive AntiTPO and 279 (46.3%) with positive AntiTg.
Histopathological diagnosis was benign in 512 (85%) and malignant in 90 (15%) patients. Age,
sex and TSH receptor antibody positivity did not differ between benign and malignant patients.
267 (52.1%) patients in benign and 19 (21.1%) patients in malignant group had no nodule in
preoperative ultrasonography (p<0.001). There was significant difference in operation
indications between benign and malignant patients (p<0.001). AntiTg was positive in 48.2% of
benign and 35.6% of malignant patients (p=0.026). AntiTPO was positive in 356 (69.5%) of
benign and 44 (48.9%) of malignant patients (p<0.001). With multiple regression analysis,
association between AntiTg positivity and benign histopathology was lost (p=0.600), while
association between AntiTPO positivity and benign histopathology remained (p=0.016).
Conclusion: In accordance with the literature, the presence of nodule in Graves patients
increased malignancy risk in our study. Additionaly, for the first time we showed that AntiTPO
positivity might play a protective role against thyroid cancer in patients with Graves disease.
262 - The rates of overtreatment and deintensification of antidiabetic and antihypertensive medications in patients with diabetes mellitus - 2018
Uluslararası Bildiriler American Diabetes Association’s 78th Scientific Sessions, Orlando, Florida, 22 - 26 June, 2018, 191-LB.
ABSTRACT
Background: Targeting better HbA1c and blood pressure (BP) goals may endanger older adults
with type 2 diabetes mellitus (T2DM) for a number of risks. Overtreatment of T2DM and
hypertension (HTN) is a trending issue but awareness and attitudes of physicians need to be
explored.
Objective: To assess the rates and predictors of overtreatment and undertreatment of glycemia
and blood pressure in older adults with T2DM. Treatment deintensification or intensification by
the physicians were also investigated.
Method: Data from older adults (≥65 years) enrolled in a large nationwide T2DM survey in
2017 across Turkey were analyzed. Overtreatment was defined as HbA1c <6.5% plus use of ≥2
oral hypoglycemics or insulin, and systolic BP <120 mmHg or diastolic BP <65 mmHg plus use
of ≥2 drugs). Undertreatment was defined as HbA1c >9% at all, and SBP >140 mmHg or DBP
>90 mmHg plus use of <3 drugs. Deintensification or intensification rates were calculated
according to treatment modification by the physicians.
Results: A total of 1276 patients were included. The overtreatment rates for glycemia and BP
were 9.8% and 5.9%, whereas undertreatment rates were 14.2% and 17.7%, respectively. In the
adjusted model, use of oral hypoglycemics only (OR:3.1, 95% CI:1.9-5.3) and follow-up at a
private clinic (OR:2.2, 95% CI:1.2-3.9) were the predictors of glycemia overtreatment. Presence
of microvascular complications (OR:2.0, 95% CI:1.1-3.5) was the only predictor of BP
overtreatment. The deintensification and intensification rates for glycemia were 25% and 75.7%
respectively, and for the BP 10.9% and 9.0% respectively.
Conclusion: The overtreatment rates of diabetes and BP in Turkish older adults with T2DM
were consistent with the previous studies, while the undertreatment rates were much higher.
Doctors seem to feel more comfortable to intensify glycemic management and largely ignore BP
control. The results warrant enforced measures to improve care of older adults with T2DM.
261 - Two cases of Graves dermopathy: A rare and pathognomonic symptom - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, EP169, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Pretibial myxedema is a rare manifestation of Graves’ disease caused by local autoimmune attack of the connective tissue probably mediated by anti TSH receptor autoantibodies (TRab). Its prevalence changes between 0.4 and 5% in Graves ‘patients and usually is accompanied by opthalmopathy. The diagnosis requires physical examination and clinical suspicion and in doubtful cases biopsy may be performed.
Case 1: Sixty four years old female patient who has been taking methimazole treatment with the diagnosis of Graves’ disease for eight months came to the endocrinology clinic with the complaint of a lesion on the anterior face of lower third of right leg. At the dermatological examination, a plaque with a shiny surface, measuring five centimeters, looking like an orange peel was observed. Upon palpation, it presented a firm and non-depressible consistency. Patient had a history of active moderate orbitopathy and received iv steroid therapy (4.5 gr prednisolone in divided doses). The patient was euthyroid at the time of evaluation with methimazole 2 tb/day and Trab was 1.3 IU/l (at the time of diagnosis it was 135 IU/l). Histopathological incisional biopsy was performed and histopathology revealed accumulation of mucin in reticular dermis leading to separation of collagen bundles. Dermopathy was successfully treated topical corticosteroids.
Case 2: Thirty seven years old female patient admitted to the clinics with symptoms of palpitations, excessive sweating and weight loss. She was diagnosed to have Graves’ disease. Radioactive iodine uptake of the thyroid was increased and TRab was three times higher than the upper limit of normal range. She had reddish edema on the distal tibia and was referred to the dermatology clinics. Pretibial myxedema diagnosis was made clinically and the lesion disappeared completely with topical steroids.
Conclusion: Graves’ dermopathy is typically asymptomatic, they are rarely pruritic or painful. In severe cases, associated with acropathy, bone pain may result from an underlying periosteal reaction. In patients with high TRab levels and orbitopathy, we should make a proper physical examination and refer the patient to a dermatologist if the patients has a lesion and the diagnosis is equivocal.
260 - Presence of empty sella in a patient with clinical and biochemical diagnosis of acromegaly - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P853, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Acromegaly is an acquired disorder related to excessive production of growth hormone (GH) and insulin-like growth factor-1 (IGF-1). It is characterized by progressive somatic disfigurement and systemic manifestations. Empty sella (ES) is an anatomical condition comprising sella turcica that is partially or completely filled with cerebrospinal fluid mainly due to intrasellar herniation of subarachnoid space. Primary ES may be associated with endocrine dysfunction and intracranial hypertension. Primary ES has to be distinguished from secondary ES, which has been linked to iatrogenic factors (surgery, radiation, medical treatment) or may be due to pituitary tumor apoplexy or autoimmune hypophysitis. Here, we describe a patient who presented with clinical and biochemical features of acromegaly and who had an empty sella on pituitary MRI.
Case: A 73-year-old male patient was consulted to our clinic for acromegalic phenotype while planning to be operated due to colorectal adenocarsinoma. The patient noticed gradual enlarging of his hands, feet, lips, and nose for 30 years, but never consulted to any clinician for this reason. Physical examination revealed typical acromegalic features. Visual field defect was not detected. Laboratory data showed elevated serum growth hormone (GH; 20.6 ng/ml)(normal <3 ng/ml) and insulin-like growth factor-1 (IGF-1; 531 ng/ml)(normal, 69-200 ng/ml). An oral glucose tolerance test (OGTT) showed no suppression of GH values. Serum levels of prolactin (PRL), adrenocorticotropic hormone (ACTH), cortisol (CS), thyroid-stimulating hormone (TSH), follicle-stimulating hormone (FSH), andluteinizing hormone (LH) were normal. T1-weighted magnetic resonance imaging (MRI) revealed an empty sella. Thorax computed tomography (CT), abdomen CT and 18F-FDG PET-CT did not have any finding consisted with ectopic GH secretion. Adenoma releasing growth hormone releasing hormone (GHRH) was not considered as GHRH was in the normal range (<100 mg/dl). He was treated with Octreotide LAR 20 mg per 28 days. At 6th month evaluation, serum GH and IGF-1 levels were decreased to 5.45 ng/ml and 274 ng/ml (normal, 69-200 ng/ml), respectively.
Conclusion: The mechanism underlying the association of acromegaly and empty sella remains unclear. However, our patient did not have a history of pituitary apoplexy, we should keep in mind that apoplexy on existing pituitary adenoma and then formation of necrosis can proceed empty sella. Yet, we have not found any reason for secondary empty sella in our patient. So, he has probably primary empty sella.
259 - Thicknesses of Chorioretinal layers in Prolactinoma Patients: A Spectral Domain Optical Coherence Tomography Study. - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P842, Endocrine Abstracts, Volume 56, ISSN 1479- 6848 (online)
ABSTRACT
Introduction: Prolactinoma is a type of pituitary tumor that produces excessive amount of the hormone prolactin. It is the most common type of hormonally-active pituitary tumor. These tumors can result in ocular complications such as vision loss and visual fields (VF) defect. In this study, we aimed to evaluate thicknesses of chorioretinal layers in patients with prolactinoma.
Material and method: We enrolled 21 prolactinoma patients (13 females, 8 males and mean age: 40.7G 8.1 years) and 18 age and gender matched healthy controls. All participants underwent complete hormonal and ophthalmological examination including thicknesses of chorioretinal layers and VF test. We used the Spectralis spectral domain optical coherence tomography for evaluation of chorioretinal layers in an outpatient setting. The seven layers were retinal nerve fiber layer (RNFL), ganglion cell layer (GCL), inner plexiform layer (IPL), inner nuclear layer (INL), outer plexiform layer (OPL), outer nuclear layer (ONL), and retinal pigment epithelium (RPE). Additionally, we calculated the mean thickness of two combined layers: inner retinal layer (IRL) and photoreceptor layer (PL). The results of prolactinoma patients were compared with the control group.
Results: There were no statistically significant differences in median right-left and mean RNFL, GCL, IPL, INL, OPL, ONL, and IRL measurements between prolactinoma and control groups (PO0.05 for each). Median right and mean RPE were significantly low in the prolactinoma group (PZ0.018 and PZ0.028, respectively). Median right-left PL was similar in two groups, while mean PL was significantly lower in patients with prolactinoma compared to control group (PZ0.04) None of the patients had VF defect. When we compared two subgroups of prolactinoma patients (active/inactive), we found that the thicknesses of layers were not significantly different between the groups.
Conclusion: To our knowledge, this is the first study that evaluates thicknesses of chorioretinal layers in patients with prolactinoma. Thicknesses of many layers were similar with control group, while mean RPE and PL were lower in prolactinoma group.
258 - Coincidental prolactinoma and parathyroid adenoma in a patient with negative MEN1 and MEN4 - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P1081, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Multiple endocrine neoplasia type 1 (MEN 1) is associated with neoplasia and hyperfunction of the parathyroid and pituitary glands, pancreatic islet cells, and neuroendocrine cells of the gut. Many authors advocate routine subtotal or total parathyroidectomy and autotransplantation for these patients. Here we demonstrate negative MEN1 and MEN4 gene mutation analysis in a case with prolactinoma and a large parathyroid adenoma that could not be localized with preoperative imaging techniques.
Case: A 21-year-old man applied with a 8 years history of recurrent renal stones and increased serum calcium (11.25 mg/dl [Normal-9-10.5mg/dL]), alkaline phosphatase (147 U/L [Normal-30-120U/L]), serum parathyroid hormone (137 pg/l[Normal-10-60pg/mL]) and low phosphorus (2.1 mg/dl [Normal 3-4.5mg/dL]). Localization studies by imaging techniques (neck ultrasonography, Computed tomography and Tc-99m MIBI scintigraphy) failed to determine the number and location of diseased parathyroid glands. In addition, laboratory studies demonstrated elevated serum prolctine (246, Normal - 4.79-25.3 ng/mL). Other pituitary hormones were normal. Pituitary magnetic resonance imaging revealed 7.5 mm pituitary adenoma. He was started on cabergoline. Germ-line mutation analysis for MEN1 and Multiple endocrine neoplasia type 4 (MEN4) genes were negative and he had no familial history of endocrine tumors. Intraoperative parathyroid exploration demostrated a 3 cm paratyhroid adenoma. Histopathpolohical diagnosis was compatiel with parathyroid adenoma. There was no hypocalcemia or recurrence with a follow-up of 14 months.
Conclusion: Coexistence of hyperparathyroidism and prolactinoma in a young patient might not be always related to MEN1. A careful intraoperative exploration by an experienced parathyroid surgeon can be the best approach when hyperparathyroidism is diagnosed biochemically despite negative localization.
257 - Thyroid amyloidosis mimicking medullary thyroid carcinoma - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P1079, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Amyloid accumulation in the thyroid gland leading to a clinically detectable mass is a rare clinical entity. The diagnosis of thyroid amyloidosis can be confused clinically as well as cytologically with both colloidal goiter or neoplastic processes of the thyroid. We report a case of thyroid amyloidosis that was initially misinterpreted as medullary thyroid carcinoma (MTC) clinical and cytological examination.
Case: A 24 years old man with chronic renal failure admitted to our hospita with rapidly progressive enlargement of a neck mass. He was suffering from renal failure for at least 10 years secondary to nephrolithiasis and was on 3 day/week hemodialysis after the rejection of renal transplantation 2 years before. He had dysphagia and dyspnea for about 5 months. Further workup demonstrated multinodular goiter with compressive symptoms and substernal extension. He had multiple nodules with the largest diameter of 80 mm in ultrasonography. Serum TSH was 1.68mIU/L (0.27-4.2), free T4 was1.01ng/dL (0.9-1.7), free T3 was2.84ng/dL (1.8-4.6) and thyroglobulin was 758 ng/mL (0-78). Anti-thyroglobulin and antithyroid peroxidase antibodies were negative. His calcitonin level was high which was suggestive for possible diagnosis of MTC (12.6 pg/mL normal:2-8 pg/mL). Fine needle aspiration cytology of the largest nodule displayed MTC. 24 hour urine catecholamine levels were within the normal range and computerized tomography of adrenal glands revealed no pathology. Total thyroidectomy was performed and the final histopathological diagnosis was thyroid amiloidosis.
Conclusion: Although amyloid deposition in thyroid is a well known fact in MTC, it should be remembered that it is not a histological finding exclusive of this disease. In patients with a rapidly enlarging thyroid gland presenting with dysphagia, dyspnea, or hoarseness, amyloid goiter should be included in the differential diagnosis particularly when the patient has a chronic disease that might be associated with amyloidosis.
256 - A rare case of mixed medullary and papillary thyroid carcinoma related with heterozygous VAL804MET mutationa rare case of mixed medullary and papillary thyroid carcinoma related with heterozygous VAL804MET mutation - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P1179, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Papillary thyroid carcinoma(PTC) and medullary thyroid carcinoma(MTC) have always been considered different tumors. Concomitant presence of MTC and PTC in the same patient is a rare clinical event.
Case report: A 43 year-old woman admitted with fatigue, a serum thyrotropin of 4.6 uIU/ml and a 15!11 mm thyroid nodule in right lobe detected in another center. Fine needle aspiration(FNA) of the nodule was consistent with MTC. In family history, her mother had thyroid cancer but the type was unknown. Repeat thyroid ultrasonography revealed a 14!11.8!18.4 mm solitary thyroid nodule in right lobe. There were also suspicious lymph nodes in right level VI and IV and left level IV. FNA along with tyroglobuline and calcitonin wash-out was performed to lymph nodes and thyroglobulin levels were 8423, 373.3 and 0.3 ng/ml respectively while calcitonin wash-out results were O2000 pg/ml in all lymph nodes. FNA cytologies were atypia of undetermined significance for the right and nondiagnostic for the left lymph nodes. Serum calcitonin was 655 pg/ml (!5 pg/ml) and carcinoembryonic antigen(CEA) was 45.1 ng/ml (0-3.4 ng/ml). Evaluation for concomitant primary hyperparathyroidism and pheochromocytoma revealed no pathology. Total thyroidectomy with right lateral, left lateral and bilateral central lymph node dissection was performed. Pathology of the nodule was reported as 17!14 mm mixed medullary and papillary thyroid carcinoma’. Immunhistochemistry was positive for TTF-1 and calcitonin, and in focal areas thyroglobuline, CK-19 and HMBE-1 stainings were positive. One right lateral and three right central lymph node were tumour positive. The patient received 150 mCi radioactive iodine ablation therapy. Stimulated thyroglobuline was 4.2 ng/ml and a focal activity uptake in thyroid location was seen in postablative whole body scanning. Serum calcitonin and CEA regressed to 20.0 pg/ml and 2.7 ng/ml, respectively. The patient was heterozygote for C2410GOA (VAL804MET) mutation in RET protooncogene analysis. 26-year old daughter of the patient was also heterozygote for C2410GOA (VAL804MET) while other daughter had no mutation. Mutation carrier daughter of patient preferred active surveillance rather than prophylactic thyroidectomy.
Conclusion: Our patient is one of the rare cases of mixed medullary and papillary thyroid carcinoma that was evaluated completely both clinically and genetically. Mixed medullary and papillary thyroid carcinoma is a rare clinical entity but merits consideration in differential diagnosis of thyroid nodules particularly in patients with a family history of thyroid malignancy.
255 - May cinacalcet improve psychiatric symptoms by decreasing calcium levels in lithium-associated hyperparathyroidism? - 2018
Uluslararası Bildiriler 20th EuropeanCongress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P1182, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Lithium is the preferred and most efficacious therapy for acute and maintenance therapy of bipolar depressive disorder. Lithium use is associated with an increased incidence of hyperparathyroidism (4.3-6.3%) and have a female preponderance. Bilateral neck exploration was the most common surgical approach while a few patients were managed medically. The initial management of Lithium-associated hyperparathyroidism (LAH) is medical intervention which includes discontinuation of lithium or use of an alternative treatment such as atypical antipsychotics and calcimimetics. Here we demonstrate improved psychiatric symptoms after cessation of lithium and successful treatment of hypercalcemia by cinacalcet in a geriatric patient with LAH.
Case: 81-year-old woman with a history of bipolar disorder treated with lithium carbonate for more than 10 years presented with nocturia and polyuria. Her serum calcium was 11.58 mg/dl (Normal - 9-10.5 mg/dl), alkaline phosphatase 175 U/L (Normal - 30-120 U/l)), serum parathyroid hormone 380 pg/ml (Normal - 10- 60 pg/ml) and phosphorus 2.1 mg/dl (normal 3-4.5 mg/dl). No definite parathyroid lesions were identified by neck ultrasonography and Sestamibi/SPECT scans. Lithium treatment was stopped after consultation with psychiatrist. More than 3 months later, she had persistent hypercalcemia and depressive symtomps recurred. Cinacalcet (30 mg once daily) was started. After 2 weeks of treatment serum calcium level decreased to 9.5 mg/dl and PTH level was 160 pg/ml.Cinacalcet was well tolerated and the patient’s psychiatric symptoms improved without any need for lithium or other antidepressant drug.
Conclusion: Cinacalcet is known to be effective in primary hyperparathyroidism but our observations also support the use of this calcimimetic agent in lithium-induced hyperparathyroidism as a potential alternative to surgery in geriatric patients. Treatment of hypercalcemia might help to resolve depressive symptoms in these patients. Cinacalcet could represent an important pharmacological intervention in MEN1-associated primary hyperparathyroidism before surgery and in postsurgical recurrences.
254 - Are there any differences between hot and cold nodules according to cytology and histopathology results? - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P1155, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Many recent studies have shown that detection of an incidental thyroid cancer among patients operated for a toxic thyroid disease is not infrequent. We aimed to compare cytology and histopathology results of cold, warm and hot nodules in patients who had thyroidectomy due to toxic multinodular goiter (TMNG).
Methods: The cytology, histopathology and scintigraphy records of 1069 thyroid nodules from 413 patients who had operation with TMNG were reviewed in this study. The nodules were categorized as hypoactive (cold), normoactive (warm) and hyperactive (hot) groups according to scintigraphy. 0f 1069 nodules, 560 with undetermined scintigraphic activity were excluded. The cytology and histopathology results were compared.
Results: Of these 413 patients (118 men, 295 women), 23 (5.6%) had malignant and 390 (94.4%) had benign histopathology. In malignant group, 16 patients had papillary thyroid carcinoma (PTC), 3 had follicular thyroid carcinoma (FTC), 1 had an undifferentiated thyroid cancer (UTC), and 3 had thyroid tumors of uncertain malignant potential (TT-UMP). The 509 thyroid nodules were grouped as normoactive [nZ23 (4.5%)], hypoactive [nZ122 (24.0%)], and hyperactive [nZ364 (71.5%)] according to scintigraphy. Cytological evaluations of 23 normoactive nodules were as follows: 7(30.4%) nondiagnostic (ND), 15(65.2%) benign, 1(4.3%) suspicious for follicular neoplasia (SFN). The cytology of 122 hypoactive nodules were ND in 25(20.5%), benign in 86(70.5%), atypia of undetermined significance (AUS) in 5(4.1%), follicular lesion of undetermined significance (FLUS) in 3 (2.5%), SFN in 1(0.8%), and finally suspicious for malignancy (SM) in 2 (1.6%). The 364 hyperactive nodules were determined as ND, benign, AUS, FLUS, SFN, SM, and malignant in 80 (22%), 259(71.2%), 10(2.7%), 7(1.9%), 2 (0.5%), 2 (0.5%) and 4 (1.1%), respectively. There were no differences according to cytological results between groups (PZ0.616). Histopathology of normoactive nodules were PTC in 1(4.3%) nodule and benign in 22 (95.7%) nodules. However, 7 (5.7%) nodules had PTC and 1 (0.8%) nodule had FTC, 114 (93.4%) nodules had benign histopathology in hypoactive group. Histopathologies of the hyperactive group were as follows; 8 (2.2%) nodules with PTC, 2(0.6%) with FTC, 1(0.3%) with UTC, 3 (0.8%) with TT-UMP, and 350 (96.1%) nodules with benign pathology. There were no differences according to histopathological results between groups (PZ0.905).
Conclusion: Recently, incidental papillary carcinomas originating from hot nodules have been reported. Contrary to conventional knowledge, we demonstrated similar malignancy rates in hot nodules when compared with cold and warm nodules.
253 - ABO blood groups, Rh factor and thyroid cancer risk: To ‘B’ or not to ‘B’ - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P1137, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Aim : In this study, we aimed to evaluate ABO blood groups and Rh factor in patients with thyroid cancer. We also assessed whether the ABO/Rh factor had any effect on prognosis, agressive features and advanced stage of thyroid malignancies.
Methods: Medical records of patients who underwent thyroidectomy between December 2006 and September 2014 were evaluated retrospectively. Demographical and clinical features, cytological results (according to Bethesda classification), ABO blood groups and Rh factor status of patients with benign and malignant thyroid disease were compared. Additionaly, in malignant group, histopathological features were compared in patients with different ABO blood groups, and Rh positive and negative patients.
Results: Histopathological diagnosis was benign in 1299 (63.5%) and malignant in 744 (36.5%) patients. There were no significant difference in age, sex, thyroid autoantibody positivity and ABO blood groups in benign and malignant patients (PO0.05 for each). Ratio of Rh positive patients was significantly higher in malignant compared to benign group (91.8% vs 88.1%, P<0.046). In all subgroups of cytology, malignancy rates were similar in different ABO blood groups, and Rh positive and negative patients. Considering malignant patients, extrathyroidal extension and advanced stage (3-4) were more prevalant in patients with B compared to non-B blood groups (PZ0.028 and PZ0.042, respectively). Patients with O blood group had lower rate of capsular invasion than patients with non-O blood groups (PZ0.018). ABO blood groups or Rh status were not associated with thyroid cancer in this study. However, patients with B blood group had higher risk of extrathyroidal extension and advanced stage compared to patients with non-B blood group.
Conclusion: For the first time in our study, we evaluted the association of Rh factor status and thyroid cancer, and found no significant relation. ABO blood groups also did not increase malignancy risk in thyroid nodules. In malignant patients, extrathyroidal extension and advanced stage were higher in B compared to non-B blood groups. Our findings can be considered as a preliminary to investigate ABO blood groups and Rh status as factors that can identify patients with higher risk.
252 - Association between preoperative thyrotrophin and clinicopathological and aggressive features of papillary thyroid cancer - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, GP224, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Aim: We aimed to investigate the relation between preoperative serum thyrotrophin (TSH) and clinicopathological features in patients with papillary thyroid carcinoma (PTC) and microcarcinoma (PTMC).
Methods: Patients who underwent thyroidectomy and diagnosed to have benign nodular disease or PTC/PTMC in our clinic were evaluated retrospectively. Patients with a previous history of thyroid surgery, patients using antithyroid medications or thyroid hormone and patients with tumors known to be unresponsive to TSH were excluded. Histological variants of PTC were classified as nonaggressive (classical/conventional and follicular variants), aggressive (tall cell, diffuse sclerosing and columnar variants) and other variants.
Results: Data of 1632 patients were analyzed. Histopathological diagnosis was benign in 969 (59.4%) and malignant in 663 (40.6%) patients. Preoperative median serum TSH was significantly higher in malignant compared to benign group (1.41 IU/dl vs 0.98 IU/dl, P<0.001). Malignancy risk increased gradually as going from hyperthyroidism to euthyroidism and hypothyroidism (20, 40.6 and 59.1%, respectively, P<0.05). Serum TSH was lowest in benign nodular disease, higher in PTMC and highest in PTC (P<0.001). This was also true when patients with positive antithyroid peroxidase/antithyroglobulin and with lymphocytic thyroiditis were excluded from the analysis (P<0.001). Serum TSH was higher in patients with bilateral tumor, capsular invasion and lymph node metastasis (LNM) compared to patients with unilateral tumor, without capsule invasion and without LNM, respectively (PZ0.036, PZ0.002 and PZ0.001, respectively). Patients with aggressive variant PTC had higher serum TSH than nonaggressive ones (P<0.05).
Conclusion: Preoperative serum TSH was associated with increased risk of thyroid cancer and LNM regardless of autoimmune thyroid disease. With the present study, for the first time, we showed higher preoperative TSH in aggressive variants of PTC compared to nonaggressive ones.
251 - Case report: management of a patient with malignant insulinoma - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, EP9, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Malignant insulinoma is a rare functional endocrine tumor of the pancreas. Therefore, there are few data regarding their optimal therapy and long term prognosis. Malignancy is defined by the presence of metastases, mostly in lymph nodes or the liver. Generally these patients present with severe hypoglycemia and require multiple therapies. Here, we described the management of a patient with malignant insulinoma.
Case: A41-year-old womanwith symptomatic and proven hypoglycemia, presented with a 11x10 mm hypodense cystic lesion and a 16!14 mm hyperdense lesion in the tail of the pancreas, and multiple liver metastases following a computerized tomography (CT) scan. Distal pancreatectomy, splenectomy and biopsy from the metastatic liver lesions were performed. Pancreatic resection showed evidence of tumor infiltration into the peripancreatic adipose tissue and extense perineural and lymphovascular invasions. 4 of the 15 resected lymph nodes were evaluated as metastatic. The ki-67 proliferation index of the insulinoma was 7.8%. After surgery, the patient was treated with 120 mg lanreotide autogel/28 days, and with 100 mg of diazoxide two times a day. Dexamethasone therapy was started with 4 mg daily and progressively increased to 16 mg daily. Selective internal radiation therapy with yttrium-90 (Y-90) was administered to treat liver metastases. But the patient did not have benefit from radiation therapy. The patient was evaluated for the liver transplantation because Ga68 scintigraphy showed metastases only in the liver. Although dexthamethasone, lanreotide and diazoxide therapies, hypoglycemic episodes reappeared and she was rehospitalised for persisted hypoglycemia and diuretic resistant edema. Diazoxide was stopped after 6 weeks. Intravenous glucose (10-20% dextrose) infusion and subcutaneous glucagon average 1-2 ampules/day administration were performed. Oral everolimus at a dose of 10 mg/day was also started. Hypoglycemia did not resolve and then parenteral nitrution was performed. Chemotherapy was planned but general status of the patient was deteriorated and patient had respiratory distress due to probably infection or drug associated pneumonitis. Brochoscopy was planned but general status of the patients did not permit the procedure. She died from acute respiratory distress syndrome(ARDS) 3 months after the initial diagnosis.
Conclusion: Refractory hypoglycemia in patients with metastatic insulinoma is an important cause of morbidity and mortality. Surgery is the only curative treatment but does not mostly solve the hypoglycemia caused by malignant insulinomas. For our patient, although hypoglycemic episodes were controlled with aggressive medical treatment, she died due to respiratory distress.
250 - Frequency of multiple endocrine neoplasia-1 in patients with primary hyperparathyroidism - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P623, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Aim: Multiple endocrine neoplasia-1 (MEN-1) is described in patients as presence of clinical two or more primary MEN-1 associated tumors or patients who have MEN-1 clinics and also have family members with MEN-1 associated tumors. It is associated with loss of activation genetic mutation in a tumor suppressor gene called Menin. MEN-1 is associated with tumors involving the parathyroid glands, anterior hypophysis, and pancreatic islet cells. Primary hyperparathyroidism (PHPT) is the most common feature of MEN-1. In this study, we aimed to evaluate the frequency of MEN-1 associated mutation in patients with PHPT.
Materials and methods: We scanned the medical records of 361 patients with PHPT who were followed up in our department between January 2010- December 2017. We presented the data of 14 patients who had genetic analysis due to suspicious clinical findings.
Results: Totally 14 patients (two men, 12 women; median age 31.2G5.7 years) with PHPT were evaluated in genetic analysis. Menin gene mutation was found in 3 (21.4%) patients. In overall patients with PHPT (nZ361), frequency of MEN-1 (nZ3) was evaluated as 0.83%. Genetic analysis of three patients with menin mutation were as follows:
Case 1: A 37-year-old man presented with a history of recurrent nephrolithiasis during 14 years. He was diagnosed as PHPT after biochemical analysis. Genetic analysis was reported as MEN-1:c.643_646delACAG (p.Thr215Serfs*13) heterozygous. Other tumoral components of MEN-1 were not found in physical and laboratory examinations.
Case 2: A 35-year-old man was diagnosed as PHPT and prolactinoma. Genetic analysis was reported as MEN-1: c.654C1GOA heterozygous. He did not have other MEN-1 associated tumors.
Case 3: A 26-year-old woman who had hypoglycemia, hyperammonemia, hyperinsulism,partial empty sella and hyperprolactinemia in her medical history was evaluated. Genetic analysis was associated with heterozygous genomic changes as c984cOa in MEN-1 gene on 7th exon.
Conclusion: MEN-1 frequency in PHPT patients is estimated as 1-18%. The diagnosis of PHPT is usually made in second decade in MEN-1 patients. So, the guidelines mostly recommend scanning for PHPT before 30 years of age. In our study population, two patients are between ages of 30 and 40 years. It must be kept in mind that the estimated penetrance of 100% is present up to 40-50 years of age in an individual harboring the MEN-1 gene.
249 - A case of diabetes insipidus due to ectopically located neurohypophysis presented during pregnancy - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P710, Endocrine Abstracts, Volume 56, ISSN 1479- 6848 (online)
ABSTRACT
Background: Gestational diabetes insipidus (DI) is a rare complication of pregnancy, usually developing in the last trimester and resolves spontaneously 4-6 weeks postpartum. It is mainly caused by excessive vasopressinase activity, an enzyme expressed by placental trophoblasts which metabolises arginine vasopressin (AVP). However in some cases, it can develop in a patient who had limited reserve of ADH and marginal central DI prior to pregnancy and may not resolve after delivery. Herein we represent a case of DI developed in pregnancy and consisted after delivery due to ectopically located neurohypophysis.
Case: 24 year old female patient admitted to our clinics with the complaints of polyuria and polydipsia. The amount of daily consumed water was 18 l. The complaints were started in the last 2 months of pregnancy and did not resolve in 2 years after delivery. She did not have any previously diagnosed psychiatric illness such as obsessive compulsive disorder, somatization or depression. She did not have history of head trauma or symptom or sign of any pituitary hormone deficiency. She was not using any drugs which could be related with DI. In the basal biochemistry, the serum Na level was 143 mmol/l, serum osmolarity was 293 mosm/l. The urine osmolarity was 93 mosm/l. Anterior pituitary hormone levels were normal except mildly elevated prolactin (29 ng/ml). She was hospitalized for water deprivation test. During the test, urine osmolarity did not change with water deprivation but became %200 concentrated after vasopressin which was compatible with cental DI. In the pituitary MRI neurohypophyseal T1- bright spot situated ectopically in the infundibulum. Desmopressin nasal sprey was started and the symptoms resolved immediately.
Conclusion: Gestational DI is a rare complication of pregnancy occurring in two to four out of 100,000 pregnancies. It usually develops at second half of pregnancy and remits spontaneously 4-6 weeks after delivery. Serum and urine osmolality are required for the diagnosis, but other tests such as serum sodium, glucose, urea, creatinine, liver function may be informative. The water deprivation test is normally not recommended during pregnancy because it may lead to significant dehydration, and should be dane in the post partum priod. After delivery pituitary MRI should be performed at some point to exclude lesions in the hypothalamo-pituitary region.
248 - Assessment of calcium and vitamin D medications adherence in patients with hypoparathyroidism after thyroidectomy - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P231, Endocrine Abstracts, Volume 56, ISSN 1479- 6848 (online)
ABSTRACT
Aim: In this study, we aimed to evaluate the vitamin D and calcium treatments adherence in patients with hypoparathyroidism after surgery.
Materials and methods: To elucidate the medication adherence, we performed a questionnaire survey using the six item Morisky Medication Adherence Scale for medication of patients with postoperative hypoparathyroidism. These 6 questions were as follows; 1) Do you sometimes have problems remembering to take your medications? 2) Do you pay attention to take medications at exact time? 3) Do you sometimes leave your medication when you feel yourself well? 4) Do you stop sometimes your medication if you feel yourself bad and think that it is associated with medication? 5) Do you know long term benefits of taking your drugs? 6) Do you forget to being prescribed your medications when the prescription time comes? The answers were evaluated as Yes/No. In addition to these six questions, three more questions were added concerning to have worry about side effects of drugs.
Results: Totally 64 patients (12 men, 52 women; median age 48.6G11.6 years) who had postoperative hypoparathyroidism were included in our study. Average duration from diagnosis to evaluation time was 73.0G72.6 months. Average calcium and vitamin D dosages were 1388.39G897.92 mg and 0.61G0.39 mg, respectively. However, in evaluation of calcium usage, motivation level was low in 16 (26.2%) patients and information level was low in 12 (19.7%) patients. Moreover, for vitamin D usage, motivation and information levels were low in 8 (13.3%) and 4 (6.7%) patients, respectively. We found that motivation score of calcium usage was significantly low compared to vitamin D usage (P!0.001) Calcium motivation score was found as decreasing significantly with increasing disease time (rZK0.256 and PZ0.046). 38 (59.4%) patients had worry about side effects of calcium treatment. Of these, 10 (15.6%) patients left medication due to this feeling. 55.5% of patients had worry about renal problems such as nephrolithiasis and renal toxicity. 21 (32.8%) of patients declared that they were using lower doses of both drugs than recommended.
Conclusion: In this study, we found that one third of the patients had low motivation for calcium usage and more than half of patients had worry about side effects. We think that these patients must be informed about side effects and convinced about regular and careful follow-up of treatment associated side effects especially in patients who are under calcium treatment.
247 - Detection of pulmonary metastases with 18F-Fluorocholine PET/CT and treatment of refractory hypercalcemia with denosumab in a patient with long-term parathyroid carcinoma - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P187, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Parathyroid carcinoma (PC) mediated hypercalcemia is often severe and more resistant to medical treatment. 18F-Fluorocholine PET/CT is a new technique used for determining the localization of parathyroid lesions. Denosumab, novel antiresorbtive agent, has been shown to have a useful role in hypercalcemia treatment. We report a male patient in long-term follow-up of PC who had refractory hypercalcemia due to pulmonary metastases revealed with 18-Fluorocholine PET/CT and who was successfully treated with denosumab.
Case: A 49-year-old man with recurrent PC initially presented in July 2007 with diffuse bone pain at lower extremities and hypercalcemia A neck ultrasound and CT scanning revealed a 3.9x3x3.5 cm solid lesion adjacent to the lower pole of the left thyroid lobe that was shown to represent a single hyperfunctioning parathyroid lesion on 99mTc-sestamibi (MIBI) parathyroid scintigraphy. The patient underwent a left parathyroidectomy along with en-bloc left thyroid lobectomy and left lateral lymph node dissection. Histological examination revealed parathyroid carcinoma. Due to postoperatively increased calcium and PTH levels, the patient was re-operated two times during the follow-up period for local recurrences. Afterwards, local radiotherapy was applied. One year later, laboratory investigations showed significantly raised calcium and PTH levels. Intravenous bisphosphonate as zolendronic acid 4 mg/28 days was started. For last 3 years, he did not take the medication due to social problems. He had admitted to our department with severe hypercalcemia 10 years later the initial operation at June 2017. He had hypercalcemia (16.8 mg/dl). He was screened for local recurrence or metastases. In 18F-FDG PET/CT diffuse nonhomogeneous hypermetabolism in medullary bones mostly associated with metabolic bone disesase was detected. His serum calcium levels were not decreased to !14 mg/dl levels with standard therapy such as aggressive saline rehydration, intravenous bisphosphonate, hemodialysis, oral cinacalcet. He had also acute pancreatitis in hospitalised period. For detection of local recurrence, 18-Fluorocholine PET/CT which revealed high uptake on pulmonary nodules was performed. Subcutaneous denosumab of 60 mg/28 days was given. After 3 doses of denosumab, total calcium was measured as 11.4 mg/dl.
Conclusion: As in this case, imaging with 18F-fluorocholine PET/CT is feasible inrecurrent/metastatic parathyroid carcinoma. In our patient, 18F-fluorocholine PET/CT seems superior to FDG-PET/CT for detection of metastases. Denosumab is a good choice in treatment of hypercalcemia in patients who are resistant to other therapies such as hemodialysis, bisphosphonates and calcimimetics.
246 - Teriparatide treatment in a patient with atypical femoral fractures associated with long-term biphosphonate therapy - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P186, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Bisphosphonates are the most commonly used drugs for the treatment of osteoporosis and have been shown to improve bone mineral density and reduce fractures. However, approximately a decade ago, atypical femoral shaft fractures were found to be a rare complication of bisphosphonate treatment. Atypical Femoral Fractures (AFF) represent fractures located between the lesser trochanter and the supracondylar flare of a femur. An increasing pool of evidence supports their association with the prolonged use of bisphosphonates, even though a direct correlation has not been proven yet. In this report, we describe a patient who developed atypical femoral fractures after prolonged use of bisphosphonates.
Case: A 42-year-old man was referred to our out-patient clinic after operation for bilateral femoral fractures by orthopedists. The patient had the history of mild trauma. Her medical case history revealed that, for the past 6 years, he had received 70 mg/week alendronate as treatment for osteoporosis. Plain radiographs showed a transverse fracture in the bilateral femur, and cortical thickening was observed at the fracture site. His bone mineral densities (BMD) at the baseline dual-energy X-ray absorptiometry (DEXA) scan were as follows; femoral neck: 0.76 g/cm2 (T scoreK1.2), femoral total: 0.79 g/cm2 (T ScoreK1.6), and lumbar total: 0.70 g/cm2 (T Score K3.7). Blood tests indicated that his serum calcium, phosphate, and alkaline phosphatase levels were in the normal ranges. Any reason for secondary osteoporosis was not determined. The patient was diagnosed as bilateral atypical femoral fractures. The patient discontinued his alendronate regimen. The patient was treated with teriparatide 30 mg/day for osteoporosis for 18 months. After this treatment, lumbar total T-score was reduced to K2.9 (0.77 g/cm2).
Conclusion: Bisphosphonates are one of the most widely prescribed drugs for the treatment osteoporosis and the reduction of fracture risk. In this report, we presented a patient with atypical fractures associated with long-term bisphosphonate treatment. The correlation between the long-term bisphosphonate use and atypical fractures has not been conclusively established. However, the drug holiday is suggested to reduce the risk of atypical fracture after prolonged bisphosphonates use. This case confirmed that teriparatide had a rapid bone anabolic effect on unhealed atypical fractures associated with chronic bisphosphonate use.
245 - The comparison of parathyroid neoplasms evaluated by using gray scale ultrasound images and histopathological whole slide images - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P179, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Aim: The aim of this study is to correlate the histopathological cell types and morphologic features of parathyroid neoplasms with ultrasound(US) images and laboratory findings, and also gain more information about the clinical importance of these results.
Materials and methods: The parathyroid lesions of 57 patients who were operated for hyperparathyroidism were sampled on saggital plane. The slides were scanned on high resolution
and digital whole slide images were formed. The system was consisted of motorized microscope, motorized table, robotic slide loader, and a high resolution camera. The slide on the motorized table was automatically scanned with the chosen objective and a high resolution image was formed. This image was opened with the help of an interface and then examined. These images can be archived. The US and the slide images were matched by the manufacturer software program.
Results : Forty three patients were female (73.7%). The ages of the patients were between 21-48 years and the median was 53. The study population had 47 adenomas, 7 atypical adenomas, 2 carcinomas. The median of parathormone (PTH) was 194 pg/ml (min-max: 53-2800), median of the tissue area was 96.29 (min-max: 16.01-576.05). Hypoechogenic areas on ultrasound(US) were matched with chief cells in 21 (55.3%), oncocytic cells in 2(5.0%), cyctic morphology in 8(20.0%) cases. There were less chief cells and more connective tissue in hyperechogenic areas (P!0.05). Hyperechogenic areas had less clear cells than isoechoic areas (P!0.05). Lipoic tissue ratio was significantly less in hypoechoic areas than hyperechoic areas (P!0.05). There was no significant difference between echogenicity, oncocytic cells, and haemorrhagia. There was a significant positive correlation between PTH and total neoplasm area (rZ0.377, PZ0.004). There was no significant difference between cyctic area ratio and chief cell amount in atypical and other cases(PO0.05). A moderate positive lineer relationship was found between serum calcium levels and cyctic area ratio and percentage (rZ0.416, PZ0.048).
Conclusion: The morphologies of parathyroid neoplasms taken from the digital whole slide images were compared to US projections in the study. However, hypoechogenic areas of US images were matched with chief cells, hyperechogenic areas were compatible with connective and adipose tissues in histopathology. The positive lineer relationship between serum calcium levels and cyctic areas was open to new researches. Results of this study may guide the evaluation of the clinic outcomes of detailed morphometric studies with digital whole slide method
244 - Bilateral adrenalectomy with occult Cushing’s syndrome in two patients with catastrophic hypercortisolism - 2018
Uluslararası Bildiriler 20th European Congress of Endocrinology , Barcelona, Spain, 19-22 May 2018, P52, Endocrine Abstracts, Volume 56, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Ectopic adrenocorticotropic hormone (ACTH) secretion is a less common cause of Cushing syndrome(CS) and is seen in 5 to 10% of patients with endogenous hypercortisolism. The most common types are bronchial carcinoids and small cell lung carcinoma. However, in approximately 10-20% of the cases, overt tumor cannot be found. Here, we described two patients with catastrophic hypercorticolism associated with ectopic CS and who were treated with bilateral adrenalectomy.
Case 1: A 47-year-old female patient had a history of a total abdominal hysterectomy and bilateral salpingo-oopherectomy operation due to clear cell ovary carcinoma 7 months ago. She was treated with chemotherapy. After 3rd dose chemotherapy, she had been hospitalized and treated due to sepsis associated with urinary tract infection. During the follow-up period in oncology, hypokalemia was detected and she was referred to our department due to severe muscle weakness in lower extremities and hypokalemia (serum K: 2.2 mEq/l). 24-h urinary free cortisol, ACTH measurement, dexamethasone suppression test (DST) demonstrated an ACTH dependent hypercortisolism. The inferior petrosal sinus sampling was indicative for an ectopic ACTH secretion. CT-scans of the thorax and abdomen, FDG-PET/CT scan and Ga68 DOTATATE PET/CT scans, were unable to demonstrate malignancy. Previous ovarian pathology was screened for ACTH secretion and evaluated as negative. Antifungal and metyrapone were started and then bilateral adrenalectomy was performed.
Case 2: A 71-year-old male patient who had a medical history of metastatic prostate carcinoma was referred to our department due to severe hypopotasemia, muscle weakness, refractory hypertension, peripheral edema. He had a history of second operation 3 months ago due to tumoral enlargement at the base of the urinary bladder and it was evaluated as infiltration of the prostate carcinoma. 24-h urinary free cortisol, ACTH measurement, DST demonstrated an ACTH dependent hypercortisolism. CT-scans of the thorax and abdomen, FDG-PET/CT scan and Ga68 DOTATATE PET/CT scans, were negative for malignancy. Medical therapy was started. But refractory hypertension, parenteral potasium infusion need were not suspended. Bilateral adrenalectomy was perfomed. He died due to pulmonary embolism 2 months after adrenalectomy.
Conclusion: Common treatmant options of Cushing syndrome consist of tumor management, somatostatin analogs, steroidogenesis inhibitors. Bilateral adrenalectomy is a highly effective treatment for patients with severe hypercortisolism if rapid control of hypercortisolism is desired. Mortality is high especially in patients with severe co-morbidities and mostly it depends on the prognosis of the underlying malignant tumor.
243 - Upper gastrointestınal symptoms, endoscopic and pathological features, and serum gastrin and chromogranin A levels in patients with primary hyperparathyroidism - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology, Lisbon, Portugal, 20-23 May 2017, GP49, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Upper gastrointestinal (UGI) symptoms are frequently encountered in patients with
primary hyperparathyroidism (PHPT). Some of these symptoms may improve after PHPT treatment,
while hypercalcemic state may also cause permanent effects. We aimed to evaluate UGI symptoms, UGI
endoscopic and pathologic features and determine the relationship between these features with serum
chromogranin A (CgA) and gastrin in PHPT patients.
Methods: Seventy-one patients diagnosed with PHPT were included in the study after exclusion of
patients who refused UGI endoscopy, had an UGI surgery or used drugs that affect serum chromogranin
A or gastrin. Patients were questioned regarding UGI symptoms. Serum CgA and gastrin were measured.
Endoscopy was performed and gastric biopsy specimens were taken to evaluate atrophic gastritis.
Results: There were 60 females and 11 males, and median age was 52 years. Mean serum CgA and
gastrin levels were 134.10±19.43 ng/ml (28-620) and 219.39±48.6 pg/ml (14-2255), respectively.
Dyspepsia, epigastric pain and weight loss were the most common symptoms and presented in 61, 51.7
and 46.6% of patients, respectively. Endoscopy was normal in 25(35.2%) patients. Erosive antral gastritis,
atrophic gastritis, gastric ulcers, duedonal ulcers, reflux gastritis and nodular gastritis were present in 14
(19.7%), 12 (16.9%), 6 (8.5%), 5 (7%), 4 (5.6%) and 4 (5.6%) patients, respectively. Intestinal
metaplasia, gastric atrophy, gastric neuroendocrine tumor and Helicobacter pylori infection were detected
in 29.2, 20, 1.4 and 66.2% of patients, respectively. Serum CgA was similar in patients with and without
atrophic gastritis, while serum gastrin was higher in patients with atrophic gastritis (P=0.024). Presence of
intestinal metaplasia and Helicobacter pylori infection did not affect serum CgA and gastrin levels.
Conclusion: Dyspeptic symptoms are common in patients with PHPT. The frequencies of atrophic
gastritis and peptic ulcers are increased. We think that patients with PHPT should be questioned for UGI
symptoms and evaluated with UGI endoscopy when needed.
242 - Coexistence of acromegaly and rheumatoid arthritis: presentation of three cases - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology, Lisbon, Portugal, 20-23 May 2017, EP843, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Musculoskeletal system is widely affected in acromegalic patients which might cause
difficulties in the diagnosis and treatment of inflammatory rheumatological diseases. Here, we report
coexistent rheumatoid arthritis (RA) in three acromegalic patients presenting with continuing joint and
back pain although acromegalic state was in remission.
Case 1: A 64 years old female patient with acromegaly and macroadenoma had undergone
transsphenoidal surgery 11 years ago and radiosurgery 7 years ago because of clinical and laboratory
evidence of disease. The patient got into remission 3 years after radiosurgery. Because she had morning
stiffness and symmetrical pain and swelling in interphalangeal joints, she was consultated with
rheumatology and diagnosed as seronegative RA. Her complaints improved dramatically at the second
month of methotrexate, prednisolone and indomethacin treatment.
Case 2: A 62 years old female had undergone transsphenoidal surgery for acromegaly 12 years ago. She
had been treated with conventional radiotherapy and radiosurgery 4 and 10 years after diagnosis,
respectively because remission could not be achieved by medical treatment which had been stopped about
a year after radiosurgery. She had symmetrical pain, swelling and deformities in interphalangeal and
metacarpal joints. Seronegative RA was diagnosed and methotrexate and prednisolone were started.
Case 3: Acromegaly had been detected 13 years ago in a 57 years old female. Because she had refused
surgery, she had been treated with conventional radiotherapy and cure had been achieved in a year. She
complained morning stiffness, back pain and pain and swelling in hand joints. She was diagnosed to have
seropositive RA and treated with methotrexate, sulfosalazine and indomethasine.
Conclusion: Symptoms related with RA might be confused with musculoskeletal symptoms seen in
acromegaly. Detailed rheumatological physical examination and immunological evaluation might be
helpful to display concomitant rheumatological disease in acromegalic patients with ongoing
musculoskeletal complaints despite achievement of treatment targets.
241 - Do the surgical outcomes change if the surgeon accompanies the endocrinologist during the preoperative ultrasonography examnination? - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology, Lisbon, Portugal, 20-23 May 2017, EP237, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Parathyroid surgical therapy differs because the glands are small and of variable number
and location. Although localization studies have improved greatly, we may not reliably determine the
number and location of all diseased glands preoperatively. Ultrasonography (US) is the most widely used
imaging method. In this study, we aimed to demonstrate how the surgical outcomes change when the
surgeon accompanies the endocrinologist during preoperative ultrasonography examination.
Methods: This prospective study included 50 patients with primary hyperparathyroidism (PHPT) who
underwent a minimally invasive parathyroid adenomectomy under local anaesthesia at our institution
from January 2014 to December 2015. The patients were divided in two groups. In group A, all patients
underwent neck US performed by an experienced endocrinologist and the surgeon on the day of operation
and the location of the lesion was specified by the surgeon. Group B patients were operated according to
the previous US performed by the endocrinologist only.
Results: There were 25 patients in Group A and 25 patients in Group B. The two groups were similar in
regard to demographical features, biochemical and hormonal parameters. Postoperative parathyroid
hormone (PTH), calcium and phosphorus levels didn’t differ between the groups. In group A operation
duration was significantly shorter compared to Group B (25.7 min vs 45 min, P=0.00).
Conclusion: Preoperative detection of hyperactive parathyroid glands is useful for minimizing the extent
of surgical intervention, reducing operation time and decreasing the risk of perioperative complication.
240 - Does radioactive iodine therapy affect ovarian reserve ? - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology, Lisbon, Portugal, 20-23 May 2017, EP1152, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Thyroid carcinoma is common in young women. Radioactive iodine (RAI)
therapy has been confirmed as a useful treatment in the management of differentiated thyroid
carcinoma (DTC). For women with DTC, the effect of RAI therapy on gonadal and reproductive
function is an important consideration. We aimed to evaluate effects of RAI therapy on ovarian
function.
Method: Women younger than 40 years old and diagnosed with thyroid cancer that required
RAI treatment were enrolled in this study.Patients with ovarian insufficiency were excluded.
Early follicular phase serum follicle stimulating hormone (FSH) and anti-müllerian hormone
(AMH) levels were measured before and 3-6 months after RAI therapy. Friedman test is used to
detect changes in FSH and AMH levels by RAI therapy with time.
Results: Eighteen patients with a mean age of 31.9±4.9 years were enrolled in this study.
Median AMH levels were 4.2 (2.96-17.42) ng/ml, 2.21 (0.84-3.69) ng/ml, 2.08 (0.86-6.12)
ng/ml before and 3-6 months after RAI therapy, respectively. Median FSH levels were 5.5
(3.78-15.5) mIU/ml, 5.32 (4.19-35.36) mIU/ml, 6.07 (4.24-13.69) mIU/ml before and 3-6
months after RAI therapy, respectively. AMH levels before RAI were higher than after RAI
(P=0.021).AMH levels after RAI at 3 and 6 months were not different. FSH levels were similar
before and after RAI.
Conclusion: Anti-müllerian hormone (AMH) is considered an important marker of ovarian
reserve. Ovarian reserve decreases in first 6 months after RAI therapy. Further large prospective
studies are necessary to determine its predictive interest for post-treatment residual fertility.
239 - Predictive value of CHAID Algorithm in the diagnosis of malignancy in thyroid nodules with Bethesda III (AUS/FLUS) cytology - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology , Lisbon, Portugal, 20-23 May 2017, EP1377, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: ‘Artificial intelligence’ is an information-processing technology developed and inspired
by the information processing technique of human brain. Artificial intelligence applications are used
with an increasing ratio in medicine; particularly in the fields of breast cancer, radiology, cardiology,
health management and drug effects analysis. There is not any study concerning thyroid diseases and
artificial intelligence applications in the literature. In this study, we aimed to use an artificial
intelligence application - CHAID (Chi-Squaered Automatic Interaction Detection) algorithm- to
predict malignancy risk in thyroid nodules with Bethesda III -atypia of undetermined
significance/follicular lesion of undetermined significance (AUS/FLUS)- cytology.
Methods: Data of 3300 patients (6863 nodules) evaluated by our multidisciplinary council and
operated between 2005-2016 were analysed retrospectively. There were 364 patients with 385 nodules
with AUS/FLUS cytology in. 65 parameters including clinical, laboratory, ultrasonographical,
cytological and histopathological features of each nodule were evaluated. The diagnostic value of
CHAID algorithm was determined considering histopathological diagnosis as the reference method.
Results: There were 75 male (20.6%) and 289 female (79.4%) patients. Histopathological diagnosis
was benign in 282 (73.2%) and malignant in 103 (26.8%) nodules. Analysis with CHAID algorithm
revealed that presence of thyroiditis/chronic thyroiditis ultrasonographically, and presence of nuclear
groove and intranuclear inclusions cytologically were predictive for malignancy. This algorithm had a
sensitivity of 49.5%, specifity of 96.8%, positive predictive value of 85%, negative predictive value of
16% and accuracy of 84.15%.
Conclusion: The main issue in thyroid nodules is to differentiate benign and malignant lesions. While
doing this, clinician should try to avoid unnecessary ultrasonography examinations, fine needle
aspiration biopsy and surgical approach. Superfluous interventions cause increased economical burden
for both the patient and the country. Use of artificial intelligence applications in clinical practice might
help to reduce unnecessary diagnostic procedures and surgical interventions in thyroid nodules with
AUS/FLUS. cytology.
238 - Evaluation of differentiated thyroid cancer patients according to different scoring systems: a single center experience - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology , Lisbon, Portugal, 20-23 May 2017, EP1429, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: True risk evaluation is important in the management of thyroid cancer. We aimed to
evaluate patients with differentiated thyroid cancer (DTC) according to the different staging systems.
Method: Data of patients diagnosed with DTC between 2007 and 2014 at our institution were
analysed retrospectively. TNM, MACIS, EORTC, AMES, De Groot, ETA, LATS, and ATA staging
systems were applied to patients according to their original description. In
ATA risk classification system, we classified patients into four categories considering inappropriate
postoperative thyroglobulin levels.
Results: There were 983 patients (218 male and 765 female) with a mean age of 49.4±12.5 and a
mean follow-up of 42.6±24.3 months. Distribution of patients according to the staging systems were as
follows; TNM: 81.1%, 4.7%, 12.7%, 1%, 0.3%, 0.2% of patients in stage I, II, III, IVA, IVB, IVC
respectively; MACIS: 91%, 5.9%, 2.2%, 0.8% of patients in group 1-4 respectively; EORTC: 39.4%,
36.7%, 19.8%, 4%, 0.1% of patients in group 1-5 respectively; AMES: 82.2% of patients in low risk
and 17.8% in high-risk group; De Groot: 81.6%, 4.7%, 13.3%, 0.4% of patients in stages 1-4
respectively; ETA: 35.5%, 25.9%, 12.4%, 26.1% of patients in very low, low, high and undetermined
risk groups respectively; LATS: 35.5%, 26.7%, 17.7%, 20.1% of patients in very low, low, high and
undetermined risk groups respectively. According to ATA, distribution of patients in low,
intermediate, high and undetermined risk groups were respectively 26.4, 8.7, 40.8 and 23.6% in
category 1, 39.7, 12.9, 23.8 and 23.6% in category 2, 46.7, 15.2, 14.5 and 23.6% in category 3, and
3.9, 19.2, 3.3 and 23.6% in category 4.
Conclusion: Variable scoring systems with variable risk assessments were suggested for DTC in the
literature. A standardized categorization is required to overcome confusion and help clinicians during
management of these patients.
237 - Is thyroid imaging reporting and data system useful in prediction of malignancy in thyroid nodules with persistent nondiagnostic cytology? - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology , Lisbon, Portugal, 20-23 May 2017, EP1413, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Although malignancy rate is low in thyroid nodules with nondiagnostic (ND) cytology,
it is reported as higher in persistent ND nodules. We aimed to determine the role of ultrasonography
(US) features and Thyroid Imaging Reporting and Data System (TIRADS) in the prediction of
malignancy in patients with persistent ND cytology.
Methods: 246 patients who underwent thyroidectomy with an indication of at least two ND cytologies
were included in this study. Suspicious US features (solid component, hypoechogenicity, irregular
margin, microcalcification, and taller-than- wide shape) and TIRADS categories (TIRADS category 3,
4a, 4b, 4c and 5) of each nodule were obtained from medical records.
Results: Of the 246 patients, 218 (88.6%) had benign and 28 (11.4%) had malignant final
histopathology. Of these 28 patients with malignant histopathology, 25 (89.3%) were evaluated as
papillary thyroid carcinoma, 1 (3.6%) as follicular thyroid carcinoma, 1 (3.6%) as medullary thyroid
carcinoma, and 1 (3.6%) as undifferentiated thyroid carcinoma. Frequencies of taller-than- wide shape,
solidity, hypoechogenicity, microcalcifications, and irregular margins were similar in benign and
malignant groups (P>0.05, all). TIRADS categories of 246 nodules with ND cytology were as follows;
12 (4.9%) TIRADS 3, 53 (21.5%) TIRADS 4a, 104 (42.3%) TIRADS 4b and 77 (31.3%) TIRADS 4c.
There was not any nodule with TIRADS 5 category. Malignancy rates of categories 3, 4a, 4b, and 4c
nodules were 0, 13.2, 9.6 and 14.3%, respectively. No significant differences were found in TIRADS
categories between benign and malignant nodules (P>0.05, all).
Conclusion: In the present study, malignancy rate was found as 11.4% in nodules with persistent ND
cytology. There was not any suspicious US feature that was predictive for malignancy in ND nodules.
Thyroid nodules in TIRADS 4a, 4b and 4c categories had higher malignancy rates than estimated risk
of malignancy reported by the Bethesda system in ND cytology.
236 - Differentiated thyroid cancer in patients taking lithium for bipolar affective disorder: A case series - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology , Lisbon, Portugal, 20-23 May 2017, EP1376, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Aim: Lithium bicarbonate is a drug used in the initial treatment of bipolar disorders. Lithium is an
element of alcali metal group and besides being a causative agent for goiter and hypothyroidism
primarily, it has also some antithyroid effects. Rarely, lithium may cause hyperthyroidism secondary
to thyroiditis or probably autoimmune mechanisms. The association between lithium and thyroid
cancer is very little known subject. In this case series, we presented differentiated thyroid cancer in 5
patients using lithium for the treatment of bipolar affective disorder
Cases: 3 of patients were female and 2 were male. 3 patients had hypothyroidism and were using
levothyroxine and 2 patients were euthyroid. There was a solitary thyroid nodule in 2, while multiple
nodules were present in others. Preoperatively, thyroid fine needle aspiration biopsy was performed in
all patients and cytological results were suspicious for malignancy in 3, atypical cells in 1 and atypia
of undetermined significance in 1 subject. Histopathologically, 1 patient had minimal invasive
follicular carcinoma, 2 had papillary thyroid carcinoma, and 2 had concomitant papillary thyroid
carcinoma and papillary thyroid microcarcinoma. All patients were given radioactive iodine ablation
treatment postoperatively.
Conclusion: Thyroid dysfunctions can be observed in patients using lithium due to various
mechanisms. Among these, thyroid cancers are the least known and patients with nodular goiter on
lithium therapy should be evaluated carefully for the risk of development of thyroid cancer.
235 - Prolonged iodine excess due to hysterosalpingography in a pregnant woman - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology , Lisbon, Portugal, 20-23 May 2017, EP1250, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Hysterosalphingography (HSG) is the radiographic examination of uterine cavity and
fallopian tubes. It is generally used during evaluation of infertility and radioopaque contrast is injected
through cervical duct during the procedure. Lipiodol which is the most commonly used contrast media
in HSG is a fatsoluble iodinated contrast media. This iodine is progressively cleared from the body in
a period ranging from a few weeks to a few months. Here, we present a 6 week pregnant woman who
underwent HSG 9 months ago and has very high urinary iodine excretion.
Case: A 31 years old woman at the 6th week of pregnancy was consultated for high blood glucose.
She was evaluated for infertility for 2 years, and HSG was performed 9 months before conception.
There was no history of drug or nutritional supplement use that has high iodine content and that might
affect iodine status. Iodine excretion was 10087 mcg/L (100-700 mcg/L) in random urine sample and
>450 ug/L in 24 hour urine. Her serum TSH was 2.19 uIU/mL, fT4 was 1.32 ng/dL and fT3 was 1,32
pg/mL. Thyroid autoantibodies were negative and thyroid ultrasonography was normal.
Conclusion: The optimal time for normalization of body iodine stores after exposure of iodinated
contrast media is not known exactly. Thyroid dysfunctions in the form of both hypothyroidism or
thyrotoxicosis can develop in euthyroid subjects after use of iodinated contrast media during HSG. In
our case, thyroid functions were normal but urinary iodine was very high even several months after
HSG. This suggests that females at reproductive age who underwent HSG might have excess iodine
concentration for a prolonged time and should be carefully evaluated for development of thyroid
dysfunctions.
234 - Evaluation of oxidative stres by means of thiol-disulphide homeostasisin patients with euthyroid Hashimoto’s thyroiditis - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology , Lisbon, Portugal, 20-23 May 2017, EP1320, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Aim: In this study we aimed to evaluate the oxidative stress via evaluating changes in dynamic thiol-
disulphide status in euthyroid patients with Hashimoto’s thyroiditis (HT).
Methods: Fifty euthyroid patients with HT and 50 healthy individuals were enrolled in this study.
Thyroid function tests (free triiodothyronine (fT3), free thyroxine (fT4), thyrotropin (TSH)), acute phase
reactants (C-reactive protein (CRP), high sensitive CRP (hs-CRP)) and thiol-disulphide parameters were
evaluated. Native thiol (-SH), total thiol (-SHC- S-S- ), disulphide (-S- S-) levels, calculated
disulphide/native thiol (-S- S-/- SH), disulphide /total thiol (-S- S-/- SHC-S- S-), native thiol/total thiol (-
SH/-SHC- S-S- ) ratios were compared between groups.
Results: Mean age was 38.3±10.4 years in the patient group and 37.2±10.1 years in the control group.
There were 43 (86%) females and 7 (14%) males in the patient group while there were 39 (78%) females
and 11(22%) males in the control group. Median TSH level was significantly higher in the patient group
compared to controls (P=0.04). However, fT3 levels were similar statistically between groups (P=0.347),
free T4 was significantly lower in the patient group (P=0.01). Mean native thiol and total thiol levels were
significantly higher in the patient group compared to the control group (P=0.04 and P=0.036,
respectively). There were not any statistically significant differences between groups regarding calculated
disulphide/native thiol (-S- S-/- SH), disulphide /total thiol (-S- S-/- SH+-S- S-), native thiol/total thiol (-SH/-
SH+-S- S-) ratios. The association between acute phase reactants and thiol-disulphide parameters were
evaluated and no significant correlation was found. Similarly, there was no significant correlation
between antibody positivity and thiol-disulphide parameters.
Conclusion: To our knowledge, our study is the first one that evaluated the association between HT and
thiol-disulphide status according to Erel and Neselioglu method. In conclusion native and total thiol levels
were detected to be increased in euthyroid HT patients, these results were not consisted with the literature
data using different methods.
233 - Comparison of clinicopathological features in patients with familial and sporadic papillary thyroid cancer - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology , Lisbon, Portugal, 20-23 May 2017, GP233, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Although, familial medullary thyroid cancer is a known condition, familial papillary
thyroid cancer (PTC) is a rare and less well described clinical entity. While some studies suggest more
aggressive features in familial PTC, some do not support these findings. We aimed to compare
ultrasonographical,cytopathological and histopathological results of patients with familial and sporadic
PTC.
Methods: Data of 194 patients diagnosed with PTC histopathologically between 2007-2016 were
retrospectively reviewed. PTC in ≥2 members of the family was defined as familial PTC. Thyroid
functions, ultrasonography features, cytological and histopathological findings were compared in familial
and sporadic PTC.
Results: There were 35 tumor foci in 20 familial and 253 foci in 174 sporadic PTC patients. Gender,
thyroid functions, thyroid autoantibody positivity, mean nodule number, thyroidectomy indications and
surgical approach were similar in two groups. Preoperative ultrasonography features were available in 20
familial and 112 sporadic nodules. There was not any difference in mean nodule diameter, echogenity,
texture, microcalcification, macrocalcification, presence of hypoechoic halo, taller than wide shape,
margin irregularity and vascularization pattern. Cytological results were distributed similarly in two
groups (P=0.433). In histopathological examination, mean tumor number was 1.79±0.98 in familial and
1.46±0.77 in sporadic patients (P=0.09). Mean tumor diameters were 6.26±4.10 mm and 9.87±11.62 mm
in familial and sporadic tumors, respectively (P=0.074). Multifocality, microcarcinoma rate, variants of
PTC, vascular
invasion and extracapsular extension were similar (P=0.155, P=0.239, P=0.094, P=0.617 and P=0.743,
respectively). Capsular invasion was significantly increased in sporadic group (19.8% vs 5.9%, P=0.049).
Conclusion: Whether familial PTC is more aggressive than the sporadic form of the disease is
controversial. Clinical, ultrasonographical, cytological and most of the histopathological features of
familial and sporadic PTC were identical in our study. Early detection of cases other than index patients
might cause diagnosis at an earlier stage of the disease in familial form.
232 - Resistant microprolactinoma with partial empty sella - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology , Lisbon, Portugal, 20-23 May 2017, EP1002, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Prolactinomas are the most common hormonally active pituitary tumors that account for
40-60% of all pituitary adenomas and are usually successfully treated with dopamine agonists. Surgery or
radiotherapy is reserved for drug intolerance/resistance or in neuro-ophthalmological emergencies. We
present a patient with refractory microprolactinoma with empty sella treated by transsphenoidal surgery.
Case: 42-year- old female patient admitted with a 14 years history of prolactinoma being treated with
dopamine agonists for ten years. At the end of the tenth year, the tumor was resistant to high dose
cabergoline (4 mg/week). Magnetic resonance imaging (MRI) revealed a partial empty sella with 6.5X3.5
mm pituitary adenoma. She underwent transsphenoidal surgery. Histopathologically, a pituitary adenoma
with rare mitotic figures, Ki-67 index of 2%, no expression of p53 and no other features of atypia was
identified. Immunohistochemistry showed expression of prolactin by majority of the cells. Postoperative
MRI demonstrated empty sella (height of the gland was 2 mm) and no residual mass. After operation,
cabergoline was restarted because of high prolactin levels and amenorrhea. Despite a substantial increase
in dosage there was no clinical improvement in amenorrhea and galactorrhea and there was not any
biochemical response. Her other anterior pituitary hormones were normal while serum prolactin was 255
ng/ml (4.79-25.3 ng/ml) in her last visit.
Conclusion: A minority of patients, ranging from 10-20% in different series does not achieve
normoprolactinemia and/or tumor shrinkage despite treatment with high doses of dopamine agonists.
Those tumors are usually macroadenomas with cavernous sinus invasion and rarely microadenomas.
Resistance can be documented by demonstrating the absence or poor expression of D2 receptors on the
membrane surface of tumor cells, or abnormalities at a postreceptor level. However, molecular biology
studies cannot be routinely performed in our center. Exchange of cabergoline with bromocriptine was
successful in few cases in the literature.
231 - The variation of disulfides in the progression of type 2 diabetes mellitur - 2017
Uluslararası Bildiriler KBUD Uluslararası Katılımlı Kongre Lab&Expo 2017 (Özet Bildiri/Sözlü Sunum,SS-07)
229 - Ectopic ACTH syndrome presenting with partial loss of conciousness and nonconvulsive status epilepticus in a patient with no signs of Cushing syndrome - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology , Lisbon, Portugal, 20-23 May 2017, EP856, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Ectopic adrenocorticotrophic hormone (ACTH) syndrome is associated with variable
tumor groups most commonly originating from neuroendocrine cells. Here, we reported a patient
considered to have nonconvulsive status epilepticus initially due to neurological symptoms and
diagnosed as neuroendocrine tumor with ectopic ACTH syndrome.
Case: A 85 years old woman with regulated hypertension admitted with partial loss of conciousness.
She had cachectia and body mass index was 16.7 kg/m 2 . There was no acute pathology in cranial
imaging. Because electroencephalography revealed findings compatible with nonconvulsive status
epilepticus, levatiresatam was started. In laboratory examination she had hypokalemia (2.5 mg/dL)
resistant to replacement. Her serum cortisol was 126 mcg /ml (5-20 mcg/ml) and ACTH was 331.7
pg/mL (0-60 pg/mL). Hypophysial MRI showed a 6x3 mm lesion in right hypopysis. She did not any
physical signs of Cushing syndrome. In thoracal CT, a 16 mm solid irregular lesion extending to the
parencyma and costal pleura in right lung was observed. Abdominal CT revealed a 125 mm
heterogenous mass and satellite lesions in the liver and hypertrophic adrenal glands. A tru-cut biopsy
from the lesion was reported as metastasis of neuroendocrine tumor. The lesion was diffusely positive
for TTF-1, cytokeratin 7, synaptophysin and chromagranin. Ki67 proliferation index was 10-15% and
primary tumor was suggested to be atypical carcinoid tumor of lung according to the
immunohistopathological findings. The patient died at the 20 th day of intensive care unit due to sepsis.
Conclusion: Ectopic ACTH syndrome is a rare cause of ACTH dependent Cushing syndrome. It can
be easily included in the differential diagnosis in a patient with classical signs of Cushing syndrome
and without adenoma in hypophysis. However, like ours, well-known physical appearance and signs
of Cushing syndrome might not be seen in all patients, and the only clinical presentation might be
neurocognitive dysfunctions.
228 - The rare cause of primary hyperparathyroidism: Parathyroid Carcinoma - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology , Lisbon, Portugal, 20-23 May 2017, EP331, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Parathyroid carcinoma (PC) is a rare endocrine malignancy which accounts for 0.005%
of all cancers and less than 1% of primary hyperparathyroidism cases. This uncommon tumor usually
occurs during the fifth decade of life, with equal frequency in both sexes, and has an indolent but
progressive course. It’s frequently symptomatic and patients may have high values of serum calcium
and parathyroid hormone (PTH) with a palpable cervical mass. PC generally occurs as a sporadic
disease, and less frequently in the setting of genetic syndromes such as hyperparathyroidism-jaw
tumor syndrome and multiple endocrine neoplasia. In this study we present five different PC cases
followed in our clinic.
Cases:There were 2 female and 3 male patients with PC. The mean age of the patients was
50.4±13.7(38-65). They had presented with weakness, headache, nausea and vomiting, and widespread
bone pain. One of the patients had bone fracture and one other patient had nephrocalcinosis.The mean
serum calcium, phosphorus and PTH levels were 15.3±2.7 mg/dL (ranging between 11.6 and 18.9
mg/dL), 2.4±0.8 mg/dL and 869.4±991.9pg/mL (ranging between 87pg/mL and 2500pg/mL),
respectively. Histopathologically, mean tumor size was 29.2±11.1 (15-44) mm. Plasma calcium,
phosphorus and PTH levels were in the normal range and 36 months after surgery in 2 patients. Local
recurrence was observed in 2 patients and reoperation was performed. One other patient withlung and
bone metastasis had still high serum Ca and PTH levels despite recurrent surgeries for six times.
Conclusion. PC is usually that of a slowgrowing neoplasm and indicates progressive end-organ
damage from disturbed calcium homeostasis. While some patients present with mild increases in
serum calcium and PTH levels, some might have very severe hypercalcemia and hyperparathyroidism.
Similarly, prognosis varies from cure to life threatening unresectable and metastatic disease depending
on the presentation and surgical success.
227 - Early diagnosis of primary biliary cirrhosis during follow-up for Graves’ disease - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology , Lisbon, Portugal, 20-23 May 2017, EP1264, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Introduction: Hepatic dysfunction in hyperthyroidism may occur due to high thyroid hormones,
medications or associated autoimmune liver disease. Autoimmune hepatitis or primary biliary cirrhosis
(PBC) has rarely been reported in Graves’ disease. We report a patient presenting with pruritus and
diagnosed as accompanying PBC and Graves’ disease.
Case: A 50 years old female patient applied with progressive pruritus for at least 4 months.
Laboratory investigations showed normal alanine aminotransferase and aspartate aminotransferase.
Serum alkaline phosphatase (ALP) was 125 IU/l (≤105 IU/l), gamma glutamyl transferase (GGT) was
132 IU/l (≤42), and total serum bilirubin and conjugated bilirubin were within normal ranges. She had
low TSH (<0.005 U/l) and high serum free T4 (4.6 ng/dl) and free T3 (14.71 pg/ml). Thyroid
peroxidase antibody and thyroid stimulating hormone receptor antibody were also positive. She was
afebrile and had regular pulse rate of 110/min and normal blood pressure. There was no exophthalmus,
goiter, hepatomegaly or splenomegaly in physical examination. Ultrasonographically, the thyroid
gland was enlarged with increased vascularity. Technetium-99m scintigraphy showed increased
activity throughout the gland with cold nodules in an enlarged thyroid gland. She was started on
methimazole and propranolol. After a week of treatment, her ALP and GGT levels raised to 160 and
151, respectively that we discontinued methimazol. Serology tests for viral hepatitis, human
immunodeficiency virus and cytomegalovirus were negative; laboratory tests excluded copper, iron-
related metabolic disorders and autoimmune liver diseases. Anti-mitochondrial antibody was found
positive and PBC was diagnosed with clinical and laboratory findings. She was started on
ursodeoxycholic acid and underwent bilateral total thyroidectomy.
Conclusion: PBC is often associated with other autoimmune diseases. When a cholestatic pattern of
liver enzymes is observed during follow-up for Graves’ disease, PBC should be considered in the
differential diagnosis.
226 - Which cytologic or architectural characteristics are associated with malignancy in AUS/FLUS cytologies according to subgroups? - 2017
Uluslararası Bildiriler 19th European Congress of Endocrinology , Lisbon, Portugal, 20-23 May 2017, EP1326, Endocrine Abstracts, Volume 49, ISSN 1479-6848 (online)
ABSTRACT
Aim: Atypia/follicular lesion of undetermined significance(AUS/FLUS) is a category of thyroid
cytology with features that are neither definitely benign or malignant. We aimed to determine whether
specific cytologic or architectural features are associated with malignancy in AUS/FLUS category of
Bethesda system according to subgroups.
Methods: The specimens of patients who underwent surgery with preoperative thyroid fine neeedle
aspiration (FNA) biopsies of Bethesda Category III (AUS/FLUS) were reanalyzed. An experienced
cytopathologist who blinded to original cytology and final histopathology was reevaluated the
specimens and numerated the cytology from 1 to 7 according to Bethesda system as follows; Group 1:
cells producing microfollicles, Group 2: containing predominantly Hurthle cells with rare cells and
colloid, Group 3: difficulty in evaluation of atypia due to smear artifacts, Group 4: cellular smears
containing benign Hurthle cells, Group 5: focal cells with nuclear changes like papillary carcinoma but
generally benign appearance, Group 6: cells with atypic features but generally benign appearance,
Group 7: rare follicular cells with nuclear enlargement and frequently apparent nucleoli.
Results: Specimens of one hundred and ninety five patients (153 females, 42 males) with a mean age
of 47.87±12.18 years were included to the study. Of these 195 patients, 148 had AUS and 47 had
FLUS cytology. Nuclear groove formations are found as higher in malignant group in overall study
population and in also AUS subgroup (P=0.005 and P=0.023, respectively), but not in FLUS subgroup
(P=0.164). Nuclear enlargement, overlapping, elongation, inclusions, and papilleroid features were
similar between malignant and benign groups in all patients, AUS and FLUS subgroups. Furthermore
cytologic groups distributions are similar between benign and malignant groups in all patients, and in
AUS and FLUS subgroups (P>0.05, for all).
Conclusion: Patients in Bethesda Category III particularly in AUS subgroup with cytologic
interpretation of nuclear grooves are at higher risk of malignancy and should undergo surgery.
225 - Different Clinical Presentations in Three Patients with Adrenocortical Cancer - 2016
Uluslararası Bildiriler Endobridge 2016, Antalya, Turkey, 20-23 October 2016, Oral presentation-25
ABSTRACT
Introduction: Adrenocortical carcinoma (ACC) is a rare disease with poor prognosis. About 42% to 57% of patients with ACC present with symptoms of hormonal excess such as Cushing syndrome or virilization. Non-functional tumors usually present with abdominal or flank pain, varicocele and renal vein thrombosis. In addition, a growing proportion of these patients (>15%) is initially diagnosed incidentally. Here we report 3 ACC cases with different clinical presentations.
Case 1: A 38-year-old female patient admitted to our clinic with low back and abdominal pain, weight loss, and hirsutism. On physical examination, her body mass index was 17.3 kg/m2 and Ferriman-Gallwey score (FGS) was 10. She had a history of vena cava inferior (VCI) thrombosis and a filter was put in another center 6 months ago. Abdominal ultrasonography (US) revealed invasion and thrombosis in VCI and multiple metastatic lesions with the biggest diameter of 58 mm in the liver. In computerized tomography (CT), a 200x95 mm lesion in the left adrenal gland was observed. Basal cortisol and ACTH levels were 11.4 mcg/dL and 4.6 mcg/dL, respectively. Overnight 1 mg and 2 days 2 mg dexamethasone suppression tests (DSTs) showed no suppression in the morning fasting cortisols. DHEAS was 907 mcg/dl (normal limits: 0-340 mcg/dl) (Table 1). The percutaneous biopsy of metastatic mass in the liver revealed ACC and the patient was evaluated as inoperable.
Case 2: A 57-year-old female patient admitted to internal medicine clinic with fatigue, abdominal pain and high blood pressure. She was referred to our clinic due to low potassium (3.1mEq/L) concentration. In further laboratory examination, basal cortisol was 11.8 mcg/dL, ACTH was 2.6 mcg/dL, DHEAS was very high (1000 mcg/dl) and plasma aldosteron/renin ratio was normal. Abdominal CT revealed a 110x88 mm mass in the right adrenal gland. There was no suppression in overnight 1 mg and 2 days 2 mg DSTs (Table 1). Patient underwent right adrenalectomy and pathology was consistent with ACC.
Case 3: A 52-year-old female patient admitted to our clinic with hirsutism in the last 6 months. On physical examination, her body mass index was 31 kg/m2 and plethora, moon face, abdominal obesity, abdominal blue-purple striae, and buffalo hump were present. Basal cortisol and ACTH were 23.0 mcg/dl and 1.0 pg/ml, respectively. DHEAS was 884 mcg/dl. Overnight single dose of 1 mg and 2 days 2 mg DSTs showed no suppression (Table 1). Adrenal Cushing’s syndrome was diagnosed. A 80x60 mm mass in the left adrenal gland was observed in abdominal CT. Right adrenalectomy was performed and the histopathological diagnosis was ACC.
Conclusion: ACC is seen more commonly, diagnosed at a younger age and more often functional in females compared to males. The clinical presentation varies in a wide spectrum ranging from asymptomatic/mild disease as in case 3 to symptoms related with hormone overproduction as in case 2 and to severe life threating metastasis as in case 1.
Table 1. Clinical, laboratory and radiological findings of patients
.
Case 1 | Case 2 | Case 3 | |
Age /sex | 38/Female | 57/Female | 52/Female |
Presentation | Abdominal pain, weight loss, hirsutism, inferior vena cava thrombosis | Fatigue, abdominal pain high blood pressure, hypokalemia | Hirsutism, moon face, blue-purple striae, buffalo hump |
Basal cortisol (mcg/dl) | 11.4 | 11.8 | 23 |
ACTH (pg/ml) | 4.6 | 2.6 | 1 |
Overnight DST (mcg/dl) | 10.2 | 12.4 | 24 |
Low dose DST (Liddle) (mcg/dl) | 13.1 | 12.9 | 25.8 |
8 mg DST (mcg/dl) | 12.6 | 13.2 | 23.2 |
24 hour urinary catecholamines | Normal | Normal | Normal |
Aldosterone/renin | Normal | Normal | Normal |
DHEAS04 (0-340mcg/dl) | 907 | 1000 | 884 |
17-OH progesterone (0.27-1.99) (ng/ml) | 6.2 | 2.5 | 0.8 |
Adrenal imaging | 200x95 mm heterogeneous necrotic hypodense solid lesion in the left adrenal gland, metastatic lesions (max 58 mm) in the liver | 110x88 mm heterogeneous necrotic solid lesion in the right adrenal gland | 80x60 mm heterogeneous solid lesion in the left adrenal gland |
ACTH: Adrenocorticotrophic hormone, DST: dexamethasone suppression test
224 - A case with adrenal cyst hydatid mimicking malignant tumour in MRI and PET-CT - 2016
Uluslararası Bildiriler Endobridge 2016, Antalya, Turkey, 20-23 October 2016, Oral presentation-38
ABSTRACT
Introduction: The adrenal gland is considered as an exceptional localization of a hydatid cyst. Adrenal hydatid cysts are usually secondary to generalized echinococcosis. The reported incidence of adrenal hydatid cysts is 0.5%. We present here a case of an adrenal hydatid cyst mimicking a malignant tumour in the imaging techniques such as magnetic resonance imaging (MRI) and positron emission tomography (PET)- computerized tomography (CT).
Case: A 70-year-old woman was admitted to our hospital for abdominal pain. She had undergone surgery for liver hydatid cysts 4 years ago. No hypertension was present in medical history. In her physical examination; blood pressure, temperature, and heart rate were 130/90 mmHg, 36.9ºC, and 88/min, respectively. Tenderness in the epigastrium and right hypochondrium were observed on palpation. Other physical examination findings were normal. Blood tests revealed leukocytes and eosinophils within normal values except anemia (Hb:11.2 gr/dL). Erythrocyte sedimentation rate was 93 mm/h. Abdominal ultrasonography revealed 71x91 mm and 61x65 mm hypoechoic masses containing internal cystic components in the liver. Abdominal MRI showed that there were cystic masses with 8 cm and 9 cm in diameter in the right lobe of the liver, and a 65x40 mm heterogenous probably malignant mass with internal cystic components in the right adrenal localisation which was showing diffusion limitation and contrast enhancement in early and delayed phases (Figure 1). Indirect hemaglutination test of echinococcus granulosus was positive. Renin, aldosterone, plasma metanephrine and normetanephrine, fractionated urinary catecholamine and dehydroepiandrosterone sulfate levels were normal. One mg dexamethasone suppression test was evaluated as negative. In PET-CT, increased 2-[fluorine-18]-fluoro-2-deoxy-D-glucose (FDG) involvement was observed in the right adrenal mass (SUVmax 8.3), and cystic lesions of liver (SUVmax 4.8). She underwent an open laparotomy, and drainage of hepatic cysts and right adrenalectomy were performed. Histopathological examination revealed a cuticular layer and germinative membrane.
Conclusion: Hydatid cystic disease of the adrenal glands is rarely observed in clinical practice. Most hydatid cysts arising from the adrenal gland are part of a disseminated disease. These are mostly asymptomatic and found incidentally by imaging or during surgery for other abdominal pathologies. Treatment of adrenal hydatid cysts is mostly surgical (pericystectomy or resection of the entire adrenal gland). The adrenal cyst hydatids can mimic malignant adrenal lesions in imaging techniques as in our case. Adrenal hydatid cysts should be considered in patients with incidentally discovered adrenal masses especially with a history of hydatid cystic disease.
Keywords: adrenal gland, liver, hydatid cystic disease, imaging techniques
223 - Primary thyroid lymphoma presenting with subacute thyroiditis - 2016
Uluslararası Bildiriler Endobridge 2016, Antalya, Turkey, 20-23 October 2016, Oral presentation-05
222 - Discordance in tumor diameter determined by preoperative ultrasonography and postoperative histopathology in differentiated thyroid cancer - 2016
Uluslararası Bildiriler 39th Annual Meeting of the European Thyroid Association 3-6 Sept 2016 Eur Thyroid J Vol. 5, Suppl. 1, 2016 P3-05-04 sayfa 159
221 - Comparison of ultrasound-guided fine needle non-aspiration and aspiration technique in evaluation of patients with neck lymph nodes in terms of cytological diagnositicity - 2016
Uluslararası Bildiriler 39th Annual Meeting of the European Thyroid Association 3-6 Sept 2016 Eur Thyroid J Vol. 5, Suppl. 1, 2016 P3-05-01 sayfa 158
ABSTRACT
Objective: Recent studies concerning fine needle cytology of lymph node (FNCLN) have shown that
non-aspiration (NAS) technique is superior to aspiration (AS) in terms of obtaining easily
interpretable material without significant difference between two methods. We aimed to compare NAS
and AS technique in evaluation of FNCLN in point of cytological diagnositicity.
Method: Of 134 patients, 123 LNs in 75 patients who underwent NAS- and AS-FNCLN in the same
visit were evaluated in this retrospective study. Ultrasonographic and cytopathologic features of all
LNs were noted. Cytopathologic results were categorized in 5 groups as insufficient, benign, atypia of
undetermined significance (AUS), suspicious for malignancy, and malign. However, all of results
except insufficient cytology were accepted as diagnostic, the insufficient results were categorized as
non-diagnostic.
Results: The numbers of LNs located in Level (L) 1, L2, L3, L4, L5, L6, and L7 were 2, 28, 29, 26, 6,
30, and 2, respectively. Median LN volume was 0.41(0.07-20.08) ml. Ultrasonographic features of
LNs were heterogen echogenicity in 82.8%, solid texture in 82.9%, presence of
micro/macrocalcification in 29.3 %, spheric shape in 11.5%, coalescence feature in 6.5%, absence of
hilum in 74.8%, and presence of irregular hilum in 5.7%. The rates of malignancy were 13.8% in AS
vs 16.3% in NAS technique, whereas benign cytology was detected in 32.5% and 43.1%, respectively.
The diagnositicity rates were 56.9% in AS and 74.8% in NAS technique (p<0.001) (Table 1).
Conclusion: Diagnositicity rate in NAS-FNCLN was significantly higher than AS-FNCLN. Lesser
degree of cellular trauma and degeneration, and better maintained architecture because of the lack of
vacuum pressure may be the reasons of increase in the rate. To reduce non-diagnostic cytology results,
we suggest NAS-FNCLN technique which is easier to perform and causes less worry in the patient.
220 - Clinicopathological features of thyroid carsinomas in geriatric patients - 2016
Uluslararası Bildiriler 39th Annual Meeting of the European Thyroid Association 3-6 Sept 2016 Eur Thyroid J Vol. 5, Suppl. 1, 2016 P2-07-04sayfa 142
ABSTRACT
Objective: Biological aggressivity, and recurrence and mortality rates of thyroid cancer are known to
be higher in geriatric patients. We aimed to determine clinicopathological features of thyroid cancer in
patients ≥65 years old.
Methods: Data of 933 patients diagnosed with thyroid cancer histopathologically between January
2009-December 2014 in our clinic were retrospectively reviewed. Malignant nodules in patients ≥65
and <65 years old were taken as Group 1 and Group 2, respectively. Thyroid functions,
ultrasonography(US) features and cytological and histopathological findings were compared.
Results: There were 109 (11.7%) patients ≥65 and 824 (88.3%) <65 years old. Thyroid functions,
thyroid autoantibody positivity and thyroidectomy indications were similar. There were 153 (11.4%)
and 1185 (88.6%) malignant foci in Group 1 and 2, respectively. Among nodules with available
preoperative US features, mean nodule diameter was significantly higher in Group 1 (p=0.008).
Echogenity, texture, micro and macrocalcifications, margin irregularity and vascularization pattern
were similar in two groups. Hypoechoic halo was observed in 16.4% and 28.6% of nodules in Group
1 and 2, respectively (p=0.034). Cytological results were distributed similarly in two groups
(p=0.433). Histopathologically, tumor diameter, rates of microcarcinomas and incidentality were
similar (p=0.605, p=0.759 and p=0.605, respectively). Of all cancer types, 88.8% in Group 1 and
93.9% in Group 2 were papillary thyroid cancer (p=0.028). Hurthle cell cancer constituted 3.9% of
Group 1 and 1.1% of Group 2 carcinomas (p=0.015). 2.0% and 0.2% of tumors in Group 1 and 2 were
anaplastic, respectively (p=0.012). There was not any significant difference in capsular and vascular
invasion and extracapsular extension between groups.
Conclusion: Rates of Hurthle cell cancer which is known to have worser prognosis among other
DTCs and anaplastic cancer are increased in geriatric ages. Cytological evaluation of thyroid nodules
should strongly be considered due to increased tendency for agressive tumor types in these patients.
219 - Is there any difference between female and male gender in terms of tumor histopathology and tnm stages in patients with thyroid cancer? - 2016
Uluslararası Bildiriler 39th Annual Meeting of the EuropeanThyroid Association 3-6 Sept 2016 Eur Thyroid J Vol. 5, Suppl. 1, 2016 P2-07-05sayfa 142-143
ABSTRACT
Objectives: Previous studies have reported that patients with differentiated thyroid cancer (DTC) are most frequently females whereas incidences of aggressive type thyroid cancer, anaplastic thyroid cancer (ATC), and medullary thyroid cancer (MTC) are not different in both sexes. In this study, we aimed to evaluate the distribution of gender in patients with thyroid cancer, and also to compare the histopathologic features and tumor stages of patients according to gender.
Methods: In this retrospective study, we evaluated 1009 thyroid cancer patients who were followed-up in our clinic. The demographics, postoperative histopathologic features, and tumor stages (TNM) were reviewed.
Results: There were 224 (22.2%) male and 785 (53.5%) female patients. Mean ages of male and female patients were 51.18±12.88 and 8.96±12.51 years, respectively (p=0.020). Among the 1425 carcinoma foci, 304 (21.3%) were detected in males and 1121 (78.6%) were in females (F/M=3.7). The rate of incidental carcinoma was similar in two sexes (p=0.730). The most frequent cancer type was papillary thyroid carcinoma (PTC) (n=1331, 93.4%), followed by the follicular thyroid carcinoma (FTC) (n=31, 2.2%), thyroid tumor of uncertain malignant potential (TT-UMP) (n=24, 1.7%), hurthle cell cancer (HCC) (n=21, 1.5%), ATC (n=5, 0.4%), and MTC (n=13, 0.9%). PTC was seen more frequently in females (p=0.010), while the rate of FTC, TT-UMP, HCC, and MTC were similar in two groups (p>0.05, all parameters). ATC was more prevalent in males (1.0% vs 0.2%, p=0.034). The incidence of PTC variants was similar in both sexes (p=0.424). There was no difference in both groups according to TNM stages (p=0.392).
Conclusions: In our study, we found that ATC was more frequent in males. However, there was no difference between the two groups according to other aggressive type cancers and PTC variants with probable aggressive course. Furthermore, male and female patients had similar TNM stages.
Table 1. Comparison of histopathologic features and TNM stages of groups according to gender
Male (n=224) | Female ( n=785) | p | |
Age (years) | 51.18±12.88 | 48.96±12.51 | 0.020 |
n=304 | n=1121 | ||
PTC (n,%) Classical variant Follicular variant Oncocytic variant Tall cell variant Diffuse sclerosing variant Encapsulated follicular variant Other variants | 274 (90.1) 224 (81.8) 30 (10.9) 2 (0.7) 3 (1.1) - 8 (2.9) 7 (2.5) | 1057 (94.3) 824 (78.0) 143 (13.5) 23 (2.2) 15 (1.4) 2 (0.2) 18 (1.7) 32 (3.0) | 0.010 0.424 |
FTC (n,%) | 11 (3.6) | 20 (1.8) | 0.052 |
TT-UMP (n,%) | 9 (3) | 15 (1.3) | 0.051 |
HHC (n,%) | 3 (1.0) | 18 (1.6) | 0.427 |
MTC (n,%) | 4 (1.3) | 9 (0.8) | 0.404 |
ATC (n,%) | 3 (1.0) | 2 (0.2) | 0.034 |
TNM Stage(n,%) Stage 1 Stage 2 Stage 3 Stage 4a Stage 4b Stage 4c | n=219 169 (72.2) 14 (6.4) 23 (10.5) 10 (4.6) - 3 (1.4) | n=766 594 (77.5) 46 (6.0) 95 (12.4) 16 (2.1) 2 (0.3) 13 (1.7) | 0.392 |
Incidentality (n,%) | 149 (49.0) | 531 (47.4) | 0.730 |
PTC: papillary thyroid cancer, FTC: follicular thyroid cancer, TT-UMP: thyroid tumors of uncertain malignant potential, HHC: hurthle cell cancer, MTC: medullary thyroid cancer, ATC: anaplastic thyroid cancer
218 - Evaluation of ultrasound scoring and thyroid imaging reporting and data system (tirads) in prediction of malignancy in patients with BETHESDA category III (AUS/FLUS) - 2016
Uluslararası Bildiriler 39th Annual Meeting of the EuropeanThyroid Association 3-6 Sept 2016 Eur Thyroid J Vol. 5, Suppl. 1, 2016 P2-07-01 sayfa 141
ABSTRACT
Objectives: Thyroid Imaging Reporting and Data System (TIRADS) is a simple and reliable reporting
system which uses the number of suspicious ultrasound (US) features and US risk scores in estimation of
malignancy risk. In this study, we aimed to determine the role of TIRADS in prediction of malignancy in
nodules with atypia of undetermined significance (AUS) and follicular lesion of undetermined
significance (FLUS).
Methods: 318 nodules with AUS and 121 with FLUS cytology were included. US features and
postoperative histopathology (benign/malignant) results were documented. Thyroid nodules without any
suspicious US features were classified as TIRADS category 3. Nodules representing one, two, three or
four, or five suspicious US features were determined as category 4a, 4b, 4c, and 5, respectively. Every
suspicious US feature was scored according to presence or not as 1 and 0, respectively.
Results: In AUS group, TIRADS categories of histopathologically benign nodules were significantly
different compared to malignant nodules (p = 0.028). Malignant group had more frequent TIRADS 4c
category nodules than benign ones (p = 0.027). The rates of microcalcification and hypoechogenicity
were higher in malignant group (p = 0.015 and p = 0.007) and there was no difference in solid nodule
texture and marginal irregularity between groups (p > 0.05). Malignant group had higher nodule
anteroposterior diameter/transverse diameter ratio (p = 0.009). In FLUS group, there was no difference
between malignant and benign groups with respect to TIRADS categories and US features (p > 0.05, all).
In AUS nodules, the cut-off value of US score at maximum sensitivity and specificity were calculated as
≥3 (AUC: 0.596).
Conclusion: Preoperative prediction of malignancy is very important for appropriate treatment and
prevention of unnecessary surgeries in patients with AUS/FLUS cytologies. Combinations of suspicious
US features seems to be helpful in prediction of malignancy in these nodules.
215 - Thyroid malignancy risk in different clinical thyroid diseases - 2016
Uluslararası Bildiriler 39th Annual Meetingof the EuropeanThyroid Association 3-6 Sept 2016 Eur Thyroid J Vol. 5, Suppl. 1, 2016 P2-05-02sayfa 135-136
ABSTRACT
Objectives: We aimed to evaluate malignancy risk and compare tumoral features in different clinical
thyroid diseases classified according to functional and nodular status.
Methods: Patients who underwent thyroidectomy between June 2007 and June 2014 were classified as
euthyroid nodular goiter (ENG), euthyroid multinodular goiter (EMNG), hypothyroidism with single
nodule, hypothyroidism with multiple nodules, toxic nodular goiter (TNG), toxic multinodular goiter
(TMNG), Graves’, Graves’ with solitary nodule and Graves’ with multiple nodules according to
preoperative functional status, etiology of hyperthyroidism and presence of solitary/multiple nodules.
Postoperative malignancy rates and tumoral characteristics were compared.
Results: There were 2203 (76.8%) female and 667 (23.2%) male patients. 1719 (59.9%) were euthyroid,
962 (33.5%) were hyperthyroid and 189 (6.6%) were hypothyroid. Overall malignancy was detected in
980 (34.1%) patients and 47.9% was incidental. Malignancy rates were 42.1%, 42.9% and 18.3%% in
euthyroid, hypothyroid and hyperthyroid patients, respectively (p < 0.001). 41.4% of ENG and 46.3% of
EMNG patients had malignant histopathology (p = 0.169). Mean tumor size, capsular invasion and
vascular invasion were lower in EMNG than ENG (p < 0.001, p = 0.003 and p = 0.015, respectively).
Among hypothyroid patients, 45.7% of patients with solitary and 42.2% of patients with multiple nodules
were malignant (p = 0.705). Sex distribution, mean age and tumoral characteristics were similar.
Malignancy rates were similar in all subgroups of hyperthyroidism, exceptionally Graves’ had lower
malignancy rate compared to others (p ≤ 0.01 for each). When TMNG and TNG were analysed together,
malignancy rate was 24.7% (104/421), and when Graves’ with nodule/nodules were considered, it was
19.7% (59/299).
Conclusion: In hypothyroid or euthyroid patients who underwent thyroidectomy for various reasons,
malignancy rate was higher than 40%. Although prevalence of malignancy was lower in hyperthyroid
patients, it does not confer protection against thyroid cancer. Patients with multiple nodules carry a
similar risk of malignancy as patients with solitary nodule independent of the functional status.
213 - Following long term follow-up, safe excision of metastatic focus after arterial embolisation in a patient with bone metastases of papillary thyroid carcinoma: case report - 2016
Uluslararası Bildiriler 39th Annual Meetingof the EuropeanThyroid Association 3-6 Sept 2016 Eur Thyroid J Vol. 5, Suppl. 1, 2016 P1-07-10 Sayfa 119
ABSTRACT
Background: Differentiated thyroid cancer is a slowly progressive malignancy and have a low metastatic potential. The most common sites of distant metastases are lungs and bones. Sternum, ribs and spine are being the most frequent sites of osseous metastases. Here, we presented a female patient with uncommon metastasis to pelvis during 3 years associated with papillary thyroid carcinoma.
Case: A 52-year-old female patient was examined in our department 3 years after she had undergone total thyroidectomy of papillary thyroid carcinoma (PTC). She presented with severe pain in her left buttock radiating to her lower leg. After total thyroidectomy, radioactive iodine whole-body scan revealed iodine uptake in left sacroiliac region. A positron emission tomography scan revealed hypermetabolic mass in left iliac fossa (SUV max: 10,7). Magnetic resonance imaging scan of the patient revealed a 12x11 cm lesion in the posterior region of left sacroiliac joint. Fine-needle aspiration cytology showed follicular variant of PTC. Patient was referred to the oncology center for palliative radiotherapy and completed 13 cycles. Patient received a total dose of 750 mCi radioiodine-131. Post-therapy scani demonstrated no change of uptake in mass and high serum thyroglobulin titer was sustained. The sciatic nerve could not be identified throughout its trajectory due to the close proximity of the mass to the sciatic nerve. In addition this hypervascular mass had particular challenge for the surgeon and it represented a significant danger of massive blood loss during surgery. The patient had undergone preoperative transcatheter arterial embolization. After reduction of vascularity, mass excision was performed safely in 3rd day of embolization. The patient's postoperative course was symptom free.
Conclusion: Bone metastases may cause severe complications that need multidisciplinary approach.
Preoperative transcather arterial embolization for hypervascular bone metastasis is widely accepted as
a safe procedure for reducing intraoperative blood loss and surgical morbidity.
212 - Is thyrotoxicosis associated with more aggressive variants of papillary thyroid cancer? - 2016
Uluslararası Bildiriler A single center study. 39th Annual Meetingof the EuropeanThyroid Association 3-6 Sept 2016 Eur Thyroid J Vol. 5, Suppl. 1, 2016 P1-06-08 Sayfa 115
ABSTRACT
Introduction: There are studies suggested that TSH can stimulate the development of thyroid
malignancy, and that elevated serum TSH levels are also associated with a higher incidence of thyroid
cancer and advanced tumor stage. In contrast, some have suggested that clinical hyperthyroidism
might be associated with aggressiveness of tumors, because thyroid hormone can act as a tumor
growth factor mediated by integrin αvβ3 in solid tumors, including thyroid cancer. There is scarce data
in the literature searching whether the incidence of PTC variants differ between patients with normal
or suppressed TSH.
Methods: Between January 2007 and December 2004, 2910 thyroid surgeries were performed at our
institution. Of these, 960 patients with histologically confirmed PTC were involved in the study.
Patients were divided in two groups as “euthyroid” or “toxic” according to their thyroid function tests
performed preoperatively at the time of first admission to the endocrinology clinics. Euthyroid status
was defined as normal levels of serum TSH, free T4, and T3, and thyrotoxicosis was defined as a
decrease in serum TSH level below the reference range, with normal or elevated serum free T4 and T3
concentrations. Those two groups were compared according to the frequency of different variants of
PTC.
Result: There were no statistical differences between the 2 groups with respect to age, gender,
primary tumor size and lymph node metastasis at the time of initial diagnosis. Follicular variant PTC
was significantly more prevalent in patients with thyrotoxicosis (15.9% vs 4.8%, p<0.001).
Conclusion: In our study, patients with subclinical hyperthyroidism had greater proportion of FVPTC
compared with patients with the euthyroid state. If we consider that FVPTC is more akin to minimally
invasive follicular thyroid cancer, a lesion that is known to be of low risk than to classical PTC, we
can conclude that thyrotoxicosis is not associated with worse prognostic subtypes of PTC.
210 - Adequacy of pathology reports of patients with differentiated thyroid cancer operated in a high volume tertiary endocrine center - 2016
Uluslararası Bildiriler 39th Annual Meetingof the EuropeanThyroid Association 3-6 Sept 2016 Eur Thyroid J Vol. 5, Suppl. 1, 2016 P1-05-02 sayfa 110
ABSTRACT
Introduction: Differentiated thyroid carcinoma is the most common endocrine malignancy. It usually
has an excellent prognosis with low rates of recurrence and metastasis. Risk scoring and initial
treatment plan depends on the histopathology of the tumor. This study aimed to investigate the
adequacy of the pathology reports of patients operated in our institution and diagnosed with
differentiated thyroid carcinoma (DTC).
Method: This is a cross sectional study of DTC patients operated between January 2007 and
December 2014.We performed the retrospective analysis of the pathology reports. Data collected from
the pathology reports of patients with DTC were: (1) histological type and subtype, (2) maximum
diameter of the tumor, (3) whether the tumor was uni-or multifocal, (4) information regarding
lymphovascular invasion, (5) extrathyroid extension of the tumor, (6) completeness of excision, and
(7) site ,size and number of lymph nodes involved, if they were excised. In the case of FTCs, data
regarding invasiveness [minimal invasion (either capsular and/or vascular) or wide invasion] were also
recorded.
Result: 960 pathology reports of DTC patients were analyzed. Size of the tumor was reported in 100%
of the patients. Extrathyroidal invasion, vascular invasion, completeness of the surgery were missing
in 2% of the patients. Variant of PTC was reported in 85% of the patients and the missing cases were
mostly microcarcinomas. The most missing items were the information about the capsule invasion of
the involved lymph node, the size of the metastasis within the lymph node and number of invaded
vessels in follicular cancers.
Conclusion: The pathology reports of DTC specimens frequently miss some of the information
considered necessary to provide a comprehensive patient care.
207 - Higher thyrotropin can be used as an additional risk factor in prediction of malignancy in euthyroid thyroid nodules evaluated by cytology based on Bethesda system - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, GP209, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
ABSTRACT
Introduction: Recently, it has been suggested that thyrotropin (TSH) concentration can be used as a
marker for prediction of thyroid malignancy. However, the association between the cytology results and
TSH levels is not clear. In this study, we aimed to investigate the relationship between TSH levels and
Bethesda categories and determine the role of TSH levels in prediction of malignancy in patients with
different Bethesda categories.
Methods: The data of 1433 euthyroid patients with 3206 thyroid nodules who underwent thyroidectomy
were screened retrospectively. The preoperative cytology results, thyroid function tests, thyroid
autoantibodies and presence of histopathological Hashimoto’s thyroiditis (HT) were recorded.
Results: Of the 1433 patients, 585 (40.8%) had malignant and 848 (59.2%) had benign histopathology.
Malignant group had smaller nodule size, elevated TSH levels, a higher rate of presence of HT compared
to benign group (p<0.001, all). Cytology results of 3206 nodules were as follows; 832 nondiagnostic
(ND), 1666 benign, 392 atypia of undetermined significance/follicular lesion of undetermined
significance (AUS/FLUS), 68 follicular neoplasm/suspicious for follicular neoplasm (FN/SFN), 133
suspicious for malignancy (SM), and 115 malignant. Both SM and malignant cytology groups had
significantly higher TSH levels than other 4 Bethesda categories (p<0.05, all). Benign cytology group had
significantly lower TSH levels compared to other cytology groups (p<0.05, all). TSH was significantly
lower in ND cytology group compared to AUS/FLUS, SM, and malignant cytology groups (p<0.001, all).
Patients with malignant final histopathology in ND and AUS/FLUS cytology groups had significantly
higher TSH levels compared to patients with benign final histopathology (p<0.05, all). As Bethesda
category proceeded towards cytologies with higher estimated risk of malignancy, TSH levels tended to
increase gradually.
Conclusion: In addition to cytology, TSH levels can be used as a supplementary marker in prediction of
malignancy in certain Bethesda categories.
206 - Evaluation of preoperative ultrasonographic and biochemical features of patients with aggressive parathyroid disease: Is there any reliable predictive marker? - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, GP 43, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
205 - Hyalinizing trabecular tumor of thyroid in a patient with suspicious for papillary cancer in fine needle aspiration biopsy: a case report - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 1158, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
ABSTRACT
Introduction: Hyalinizing trabecular tumor is a very rare neoplasm of thyroid and can be
misinterpreted as papillary or medullary cancer in fine needle aspiration biopsy (FNAB).
Case report: Multinodular goiter was detected in a 65 years old woman using metformin and L-
thyroxine for impaired blood glucose and Hashimoto thyroiditis, respectively. FNAB was performed
in two nodules and reported as suspicious for malignancy and benign. She underwent total
thyroidectomy and a lesion with fragmented thin fibrous capsule was detected. The lesion was not
including colloid and was characterized by eosinophilic, polygonal and elongated cells with wide
cytoplasm and oval, elongated and irregular nucleus. There was also straight nuclear notchs and
pseudoinclusions. Narrow hyalinized stroma including thin vascular structure was present between
trabecules. There was no capsular or vascular invasion. Cytokeratin 19, HBME-1 and calcitonin were
negative and TTF-1 was highly positive with immunocytochemical staining. Ki 67 proliferation index
was 1-2%. No staining with BRAF VE-1 antibody was observed. The lesion was diagnosed as
hyalinizing trabecular tumor depending on morphological and immunocytochemical findings.
Conclusion: It is difficult to differentiate hyalinizing trabecular tumor of thyroid and papillary thyroid
cancer due to similarities in morphology and origin of two tumors, and FNAB may be misinterpreted
as papillary thyroid cancer. Diagnosing hyalinizing trabecular tumor of thyroid which is benign or has
low malignant potential and which can be treated by lobectomy will certainly prevent patient from
overtreatment.
204 - Preoperative predictors of malignancy in lesions classified as BETHESDA IV - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 1148, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
ABSTRACT
Background: Differential diagnosis of a thyroid nodule is difficult if it is a follicular lesion. Follicular
lesions include follicular adenoma (FA) or a malign neoplasm (follicular cancer (FC) or follicular
variant of papillary thyroid carcinoma (FVPTC)). Cytology can’t separate benign from malignant
condition in follicular lesions. Differential diagnosis is important because patients often undergo less
than ideal interventions, such as a total thyroidectomy for a benign lesion or require completion
thyroidectomy after a lobectomy for a malignant nodule. Herein we aimed to search whether there is a
clinical or ultrasonographic marker discriminating malign lesions from benign ones.
Method: Eighty consecutive patients with an operated follicular thyroid neoplasm at a tertiary hospital
from 2007 to 2014 were reviewed. Age, gender, symptoms, history, physical findings, nodule size,
sonographic, cytologic, and final pathologic results were recorded. Malignant and benign groups were
compared according to preoperative clinical and imaging features
Results: 34 of 102 nodules were malignant where as 68 were benign. Gender distribution, baseline
thyroid function tests and thyroid autoantibody positivity were similar between the benign and
malignant groups. Family history of differentiated thyroid cancer (DTC) was significantly higher in
the malignant group (p=0.002). Regarding to ultrasonographic parameters, nodule volume and
vascularity were significantly greater in the malignant nodules (p=0.04 and 0.008, respectively)
Presence of microcalcification/irregular macrocalcification was also higher in the malignant group
compared to benign group (p=0.017). When we subdivided malignant nodules as FVPTC (18 lesions)
and FC (16 lesions), microcalfication was significantly more common in FVPTC (p=0.022).
Conclusion: Family history and certain ultrasonographic parameters might be helpful in preoperative
differentiation of benign and malignant follicular neoplasms. A combination ofthose with both FNA
and molecular results may help us to decide management of patients with follicular thyroid lesion.
203 - Can ratio of primary tumor diameter to total tumor diameter be a new parameter in the differential diagnosis of agressive and favorable multifocal papillary thyroid microcarcinoma? - 2016
Uluslararası Bildiriler 18 th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 1135, Endocrine Abstracts, Volume 41, ISSN 1479-6848
ABSTRACT
Introduction: In this study, we aimed to evaluate the usefulness of ratio of primary tumor diameter to
total tumor diameter as a new parameter for the differentiation of agressive and favorable papillary
thyroid microcarcinomas (PTMC).
Methods: The diameter of the largest tumor focus was taken as the primary tumour diameter (PTD).
For multifocal tumors, total tumor diameter (TTD) was calculated as the sum of the maximal diameter
of each lesion. A ratio was obtained by dividing PTD to TTD and defined as tumor diameter ratio
(TDR) (PTD/TTD=TDR). Positive (PPV) and negative predictive values (NPV) and sensitivity and
specifity of TDR to predict capsular invasion, extrathyroidal extension (ETE) and lymph node
metastasis (LNM) were determined.
Results: Mean TDR significantly decreased as number of tumor foci increased. In multifocal PTMCs,
the sensitivities of TDR for the detection of LNM, ETE and capsular invasion were 100%, 100% and
94.2%, respectively, the specifities were 86.2%, 88% and 94.7%, respectively. TDR had a PPV of
99.3% and NPV of 100% for LNM; PPV of 58.5% and NPV of 100% for ETE; and PPV of 89.1% and
NPV of 97.3% for capsular invasion. In patients with multifocal PTC>10 mm, mean TDR was
signficantly lower in patients with LNM compared to ones without LNM (0.76±0.12 vs 0.44±0.10;
p<0.001).
Conclusion: Decreased TDR was associated with capsular invasion, ETE and LNM in patients with
multifocal PTMC. It was also predictive for LNM even in patients without capsular invasion or ETE.
This new parameter might be particularly helpful for the detection of aggressive behavior in multifocal
PTMCs.
202 - Ultrasonographic scoring index can be useful in the prediction of thyroid malignancy in subcentimeter and supracentimeter thyroid nodules - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 1132, Endocrine Abstracts, Volume 41, ISSN 1479-6848
ABSTRACT
Introduction: The increased rate of thyroid malignancy as well as incidental and subcentimeter
thyroid nodules have been attributed to increasing use of high-resolution US which can detect the non-
palpabl or subcentimeter (maximum diameter 1 cm) thyroid nodules. We aimed to evaluate the
sonographic features of the tyroid nodules between 1 cm and > 1cm according the histopathology
results and to determine the ultrasonographical predictive factors for malignancy and an
ultrasonographic score according the sonographic features to avoid unnecessary fine-needle aspiration
biopsy (FNAB).
Methods: We retrospectively evaluated 2233 nodules of 1118 patients who underwent thyroidectomy.
Predictive factors for distinguishing between malignant and benign histopathologic results according
the ultrasonographic features were evaluated by multivariate logistic regression analysis. Multiple
binary logistic regression with the forward logistic regression method was used to develop the formula
for recommending sonographically guided biopsy.
Results: Among the 2233 nodules 337 nodules were in the 1 cm (group 1), 1896 were in the >1cm
(group 2). According the histopathological results, in group 1; 173 nodules were in the benign, 164
nodule were in the malignant group. Whereas in group 2; 1423 nodules were in the benign, 473
nodules were in the malignant group. In group 1, AP/T 1, the presence of microcalcification,
macrocalcification and hypoechoic pattern were significantly higher in the malignant group and in
group 2, the presence of microcalcification, macrocalcification, hypoechoic and iso-hypoechoic
pattern, solid texture, peripheral and intranodular vascularization pattern were significantly higher in
the malignant group. In group 1, the best ultrasonographic index score was found >2, whereas in group
2 the it was found >4.
Conclusion: Our US scoring may lead to clinicians and surgeons to diagnose thyroid malignancy
more accurately and to select the nodules for FNAB especially in subcentimeter nodules.
201 - Association of multifocality, tumor number and total tumor diameter with clinicopathological features in papillary thyroid cancer - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 1117, Endocrine Abstracts, Volume 41, ISSN 1479-6848
ABSTRACT
Introduction: In this study, we aimed to evaluate impact of multifocality, tumor number and total
tumor diameter on clinicopathological features of PTC.
Methods: Medical records of 912 patients who underwent thyroidectomy and diagnosed with PTC
were reviewed retrospectively. Patients were grouped into 4 according to number of tumoral foci; N1
(1 focus), N2 (2 foci), N3 (3 foci) and N4 (≥ 4 foci). The diameter of the largest tumor was considered
as the primary tumor diameter (PTD) and total tumor diameter (TTD) was calculated as the sum of the
maximal diameter of each lesion in multicentric tumors.
Results: Capsular invasion, extrathyroidal extension and lymph node metastasis were significantly
higher in patients with multifocal tumors compared to patients with unifocal PTC. As the number of
tumor increased, extrathyroidal extension and lymph node metastasis also increased (p=0.034 and
p=0.004, respectively). The risk of lymph node metastasis was 2.287 (OR=2.287, p=0.036) times
higher in N3 and 3.449 (OR=3.449, p=0.001) times higher in N4 compared to N1. Capsular invasion,
extrathyroidal extension and lymph node metastasis were significantly higher in multifocal patients
with PTD ≤ 10 mm and TTD 10 mm than unifocal patients with tumor diameter ≤ 10 mm (p<0.001,
p<0.001 and p=0.001, respectively). There was no significant difference in terms of these parameters
in multifocal patients with PTD ≤ 10 mm and TTD 10mm and unifocal patients with tumor diameter
> 10 mm.
Conclusion: In this study, increased tumor number was associated with higher rate of capsular
invasion, extrathyroidal extension and lymph node metastasis. In a patient with multifocal papillary
microcarcinoma, TTD 10 mm confers a similar risk of aggressive histopathological behavior with
unifocal PTC greater than 10 mm
200 - Markers predicting the contralateral lobe involvement in patients with multifocal papillary thyroid carcinoma: An instutional case series of 914 patients - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 1114, Endocrine Abstracts, Volume 41, ISSN 1479-6848
ABSTRACT
Background: The characteristics of multifocal PTC remain controversial. Surgical approach to
multifocal tumor changes between centers. In cases that the initial procedure was lobectomy, most
clinicians would suggest for completion thyroidectomy since the risk of PTC in the contralateral lobe
is significant. This study aimed to evaluate the incidence of bilateral involvement, predictive factors
for bilaterality and whether or not bilaterality was related with more aggressive histopathologic
features in patients with multifocal PTC.
Method: Medical records and pathologic data of 914 patients who underwent total thyroidectomy and
diagnosed with PTC were retrospectively reviewed. The patients with multifocal disease were detected
and subdivided into two subgroups as unilateral-multifocal PTCs and bilateral multifocal PTCs. These
two groups were compared to each other regarding demographic, clinical and histopathological
features.
Result: Multifocal disease was detected in 294 patients (32.7 %).Of all, 102 patients (36.7%) had
unilateral whereas 192 cases (65.3%) had bilateral involvement. As a result of univariate analysis,
bilaterality was significantly associated with the number of tumor foci (p<0.001), tumor size
(p=0.008), TSH (p=0.002) and capsule invasion (p=0.018). Multivariate analysis demonstrated that the
number of tumor foci and TSH level were independent risk factors for bilaterality in multifocal PTC
(p<0.001 and p=0.006, respectively).
Conclusion: Incidence of bilateral tumors is high and increases with the number of tumor foci in
multifocal PTC. Bilateral involvement in multifocal PTC is not associated with worse
histopathological futures.TSH can be taken as a preoperative indicator able to predict multifocal
cancers and guide clinical decision making and surgical management.
199 - Ultrasonographical, clinical and histopathological features of 1264 nodules with papillary thyroid carcinoma and microcarcinoma based on tumor size - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 1108, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
ABSTRACT
Introduction: In recent years, due to the improvements in ultrasonography (US), it has become
possible to gain more information about the papillary throid carcinoma (PTC) and papillary tyroid
microcarcinoma (PTMC). However, whether PTC and PTMC exhibit the same ultrasonographic
features and behave same features is controversial. We aimed to evaluate the patients diagnosed with
PTC and PTMC in terms of clinical, ultrasonographical (US) and histopathological features and their
relationships with tumor size.
Methods: We retrospectively evaluated 881 patients who underwent thyroid surgery between 2007
and 2014 in our clinic and diagnosed with PTC histopathologically were enrolled the study.
Demographic characteristics, US findings and histopathological features were evaluated.
Results: In total, 1264 nodules were identified in the 881 patients. The incidentality rates were higher
in the PTMC group and also in the 5 mm group. In total multifocality rate was 32.9%, and it was
significantly higher in PTMC group than the PTC group. PTC and 5 mm PTMC groups compared to
PTMC and 5 mm groups respectively, were more aggresive histopathological features
Conclusion: Since the incidentality rates were found significantly more common in our patients with
PTMC and those with 5 mm, ultrasonographic features of the nodules should be evaluated carefully
and for cases which are suspicious with US, US-guided fine needle aspiration biopsy (FNAB) should
be considered in order to make the correct treatment strategy. Also our study revealed that PTC and 5
mm PTMC groups compared to PTMC and 5 mm groups respectively, have more aggresive
histopathological features.
198 - Are there any differences between demographic characteristics, preoperative ultrasonographic findings, and cytological results of patients with thyroid tumors of uncertain malignant potential and papillary thyroid carcinoma of classical and non-encapsulated follicular variants? - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 1099, Endocrine Abstracts, Volume 41, ISSN 1479-6848
ABSTRACT
Introduction: Thyroid tumors of uncertain malignant potential (TT-UMP) has been accepted as a
subgroup of follicular-patterned thyroid tumors for which benignancy or malignancy cannot be assessed
exactly. We aimed to evaluate demographic characteristics, ultrasound (US) findings, and cytological
results of patients with TT-UMP and compare these findings with the classical variant of papillary thyroid
carcinoma (CV-PTC) and non-encapsulated follicular variant of PTC (NEFV-PTC) patients, and also to
evaluate the immunohistochemical characteristics of patients with TT-UMP.
Methods: Twenty-four patients with TT-UMP, 672 with CV-PTC, and 132 with NEFV-PTC were
included to the study.
Results: Mean longitudinal nodule size and median nodule volume were higher in TT-UMP group
compared to CV-PTC and NEFV-PTC groups (p<0.001 and p<0.001 for CV-PTC; p<0.001 and p=0.008
for NEFV-PTC). Presence of halo and peripheral vascularization were observed more frequently in TT-
UMP group compared to CV-PTC group (p=0.002 and p=0.024). Nodule localization, texture,
echogenicity, presence of microcalcification, and presence of macrocalcification were similar in TT-UMP
and CV-PTC groups. US findings and cytological results were similar in TT-UMP and NEFV-PTC
groups (all, p>0.05). Benign and follicular neoplasm/suspicious for follicular neoplasm cytological results
were higher in TT-UMP group compared to CV-PTC group (p=0.030 and p=0.001). Median tumor size
was higher in TT-UMP group than CV-PTC and NEFV-PTC groups (25 mm vs 6 mm, p<0.001 and 25
mm vs 14.4 mm, p=0.006, respectively). In TT-UMP group, positive expression of HBME-1, CK-19 and
Gal-3 was found as 50%, 33.3% , and 25%, respectively.
Conclusion: This study demonstrated that patients with TT- UMP had higher nodule and tumor size
compared to CV-PTC and NEFV-PTC patients. Moreover, we found that US features and cytological
results were similar in NEFV-PTC and TT-UMP patients.
196 - Hemithyroidectomy seems to be a reasonable initial surgical approach for patients with cytologically Bethesda Category III (AUS/FLUS) thyroid nodules - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 998, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
ABSTRACT
Introduction: Atypia of undetermined significance/follicular lesion of undetermined significance
(AUS/FLUS) termed as Bethesda Category III constitute 15-30% of thyroid cytology. However, the
risk of malignancy in this heterogenous category is estimated as 5-15%. The recent studies has been
reported the malignancy rate in the wide range of 6-48%. This causes surgical approach variability
between different centers. We aimed to evaluate the initial malignancy rate, indication of
complementary thyroidectomy, and malignancy rate in contralateral thyroid lobe in patients with
AUS/FLUS thyroid nodules who underwent hemithyroidectomy .
Methods: We reviewed the medical records of 47 (7 male, 40 female; mean aged 40.3±13.3) patients
with cytologically 48 AUS/FLUS nodules who underwent hemithyroidectomy operation at our
institution. The patients with tumor size <10 mm (microcarcinoma), papillary carcinoma with
follicular, oncocytic, clear cell variants were accepted as low risk group. Patients with tumor size ≥ 10
mm, papillary carcinoma with columnar, tall cell, insular, solid, diffuse sclerosing variants, follicular
carcinoma with widely invasive variant were accepted as high risk group.
Results: The preoperative cytology was evaluated as AUS in 32 (66.7%) nodules and FLUS in 16
(33.3%) nodules. Histopathology was reported as benign in 34 (72.3%) patients and as malignant in
13 (27.7%) patients. However, 9 (19.2%) patients was in high risk group, 4 (8.5%) patients was in
low risk group. Of 13 patients, complementary thyroidectomy was performed in 11 (23.4%) patients.
Of 11 patients who underwent contralateral lobectomy, 9 (81.8%) patients had benign histopathology
and 2 (18.2%) patients had malignant histopathology.
Discussion: Malignancy rate in patients with AUS/FLUS nodules who underwent hemithyroidectomy
was found as 27.7%. Moreover, malignancy rate in contralateral lobe was demonstrated as 18.2%. It
seems that lobectomy is a reasonable initial surgical approach for these patients. Further studies with
larger sample size are needed.
195 - Neck lesions located outside the thyroid bed with similar echogenity of thyroid tissue - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 991, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
ABSTRACT
Introduction:We aimed to determine demographical, hormonal, ultrasonography(US) and cytological
features of cases with neck lesions that are located outside the thyroid region and have similar
echogenity with thyroid tissue.
Method:Neck US reports of patients who underwent fine needle aspiration(FNAB) under US
guidance in our clinic in a period of one year were reviewed retrospectively. Lesions having similar
echogenity with thyroid tissue and defined as ectopic or outside the thyroid bed were enrolled.
Demographical, hormonal, US and cytological features were obtained from medical records.
Results:There were 76 patients(69 female, 7 male) with a mean age of 51.07±12.81. 64(84.2%) of
patients had a history of thyroid surgery and 12(15.8%) were not operated before. 85.5%of lesions
were located at the level of hyoid bone, 9.2% inferior to thyroid lower pole and 5.3% in other sites.
Localization of lesions did not differ between patients with and without previous
thyroidectomy(p=0.083). Median lesion volume was 0.57 ml(0.06-24.13). Ultrasonographically,
93.4% of lesions were isoechoic and 6.6% were hypoechoic. 89.5%of lesions were solid and 10.5%
had mixed texture. Marginal irregularity was observed in 13.2%of lesions. US features were similar in
patients with and without thyroidectomy. 62(81.6%) lesions were positive with Tc99m pertechnetate
scintigraphy and avidity rate was significantly higher in operated patients(p=0.001). Cytological
diagnosis was benign in73,7%, atypia of undetermined significance/follicular lesion of undetermined
significance in 2.6%, nondiagnostic in22.4% and acute supurative infection in1.3%. There were no
differences in cytopathological results between patients with and without thyroidectomy(p=0.649).
Conclusion:In patients with a history of thyroid surgery, US examination should be extended to
outside the thyroid bed to detect possible ectopic tissue. We showed that such lesions might also occur
in patients without surgery and US features and cytopathological findings were similar in
thyroidectomized and nonthyroidectomized patients.
194 - Malignancy is associated with microcalcification and AP/T ratio in ultrasonography, but not with Hashimoto’s thyroiditis in histopathology in patients with thyroid nodules evaluated as Bethesda Category III (AUS/FLUS) in cytology - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 988, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
ABSTRACT
Purpose: The predictors of malignancy are important for decision of appropriate management in
nodules with atypia of undetermined significance/follicular lesion of undetermined significance
(AUS/FLUS). Our aim was to determine the ultrasonographical, clinical and biochemical predictors of
malignancy in these patients.
Methods: A total of 427 patients with Bethesda Category III (AUS/FLUS) thyroid nodules were
included in this retrospective study. We divided the nodules into two subgroups according to the
histopathology as benign and malignant, and compared the preoperative ultrasonographical, clinical
and biochemical findings.
Results: In overall, 427 patients with 449 AUS/FLUS nodules that went on surgery, the rate of
malignancy was 23.4% (105/449). When evaluated seperately, the rate of malignancy was 25.8% in
nodules with AUS (82/318) and 17.6% in nodules with FLUS (23/131) (p=0.061). The vast majority
of malignant specimens in histopathology consisted of papillary thyroid carcinoma (PTC) (n=91,
86.7%). Preoperative ultrasonographic features of 105 malignant nodules in histopathology were
compared with the 344 benign nodules. AP/T ratio was significantly higher in malignant group
compared to benign group (p=0.013). In multiple logistic analyses, we found that AP/T ratio, and
microcalcification were independently correlated with malignancy (p<0.05). Although, in univariate
analysis, presence of thyroid autoantibodies and Hashimoto’s thyroiditis in histopathology were higher
in malignant group significantly, we did not find any correlation between malignancy and
Hashimoto’s thyroiditis in histopathology in multivariate analysis (p>0.05).
Conclusion: In Bethesda Category III nodules with higher AP/T ratio and microcalcification, surgery
might be considered as the first theurapeutic option instead of repeat FNAB or observation.
193 - Evaluation of TSH receptor antibodies and histopathological features in patients with toxic multinodular and toxic nodular goiter - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 987, Endocrine Abstracts, Volume 41, ISSN 1479-6848
ABSTRACT
Introduction: Association between high thyrotrophin receptor antibodies (TRAb) and relapse of thyroid
cancer in Graves’ patients was reported previously. In this study, we aimed to investigate possible relation
between TRAb and thyroid malignancies in patients with toxic multinodular (TMNG) and toxic nodular
goiter (TNG).
Methods: Thyroidectomized patients with a preoperative diagnosis of TMNG, TNG and euthyroid
multinodular or nodular goiter (MNG/NG) were retrospectively recruited for the study. Preoperative
TRAb measurements were available in 221 patients with TMNG/TNG and 43 patients with euthyroid
MNG/NG. Results were compared in these two groups.
Results: Histopathology was malignant in 71 (32.1 %) and benign in 150 (67.9 %) of TMNG/TNG
patients. In euthyroid group, malignancy was observed in 18 (41.9 %) and benign histopathology was
observed in 25 (58.1 %) patients. In TMNG/TNG group, TRAb was positive in 7 (9.9%) patients with
malignant and 17 (11.3%) patients with benign histopathology (p=0.742). In euthyroid group, TRAb was
positive in 1 (5.6%) patient with malignant and 2 (8.0%) patients with benign histopathology (p=0.756).
TRAb positivity did not change between TMNG/TNG and euthyroid patients with malignant and benign
histopathology (p=0.569 and p=0.620, respectively).
Conclusion: TRAb positivity seems to have no effect on malignant histopathology in patients with
TMNG and TNG. Limited number of cases and lack of TRAb measurement in all TMNG/TNG patients
undergoing thyroidectomy might contribute to this finding.
192 - Tolosa Hunt syndrome involving the pituitary: a case report - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 378, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
ABSTRACT
Introduction: Tolosa Hunt syndrome (THS) is described as unilateral orbital pain associated with paresis
of one or more of the third, fourth and/or sixth cranial nerves caused by a granulomatous inflammation in
the cavernous sinus, superior orbital fissure or orbit. Pituitary gland is rarely involved in this syndrome.
Herein we represented a case with hypophysitis with Tolosa Hunt who was operated with the suspicion of
pituitary adenoma.
Case: A 63-year- old female patient with diabetes history admitted to our clinics with the complaints of
weight gain and headache. In the physical examination, BMI was 40 kg/m 2 and there was buffalo hump,
central obesity and acanthosis nigricans. With the suspicion of Cushing syndrome, biochemical screening
was performed with low dose dexamethasone suppression test and free cortisol in 24-hour- urine
collection. Serum cortisol after 1 mg dexamethasone suppression was 2.2 whereas free urinary cortisol
was normal. For exclusion of pseudocushing, we performed 2 days 2 mg dexamethasone suppression with
CRH and the result was equivocal (cortisol after CRH: 1.5). Her ACTH value was 20, and high dose
dexamethasone test result was consistent with Cushing’s disease. In the CRH test there was %300
increase in ACTH and %100 increase in cortisol after the administration of CRH. In the pituitary MRI, a
lesion 1.8 cm in size was reported. While the evaluation was going on, the severity of headache was
increased and ophtalmoplegia developed. The patient underwent endoscopic transsphenoidal surgery. The
histopathology of the lesion was consistent with granulamatous reaction with caseous necrosis.
Tuberculosis and sarcoidosis was excluded by PPD, thorax CT, lumbar puncture and analysis of the
cerebrospinal fluid, mycobacterium tuberculosis PCR and the culture of the pathology specimen. The
final diagnosis was Tolosa Hunt.
Conclusion:Tolosa Hunt is a very rare cause of hypophysitis and panhypopituitarism. It should be
considered in the differential diagnosis of a sellar mass.
191 - Safely operated two patients in pregnancy with primary hyperparathyroidism - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 378, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
ABSTRACT
Introduction: Tolosa Hunt syndrome (THS) is described as unilateral orbital pain associated with paresis
of one or more of the third, fourth and/or sixth cranial nerves caused by a granulomatous inflammation in
the cavernous sinus, superior orbital fissure or orbit. Pituitary gland is rarely involved in this syndrome.
Herein we represented a case with hypophysitis with Tolosa Hunt who was operated with the suspicion of
pituitary adenoma.
Case: A 63-year- old female patient with diabetes history admitted to our clinics with the complaints of
weight gain and headache. In the physical examination, BMI was 40 kg/m 2 and there was buffalo hump,
central obesity and acanthosis nigricans. With the suspicion of Cushing syndrome, biochemical screening
was performed with low dose dexamethasone suppression test and free cortisol in 24-hour- urine
collection. Serum cortisol after 1 mg dexamethasone suppression was 2.2 whereas free urinary cortisol
was normal. For exclusion of pseudocushing, we performed 2 days 2 mg dexamethasone suppression with
CRH and the result was equivocal (cortisol after CRH: 1.5). Her ACTH value was 20, and high dose
dexamethasone test result was consistent with Cushing’s disease. In the CRH test there was %300
increase in ACTH and %100 increase in cortisol after the administration of CRH. In the pituitary MRI, a
lesion 1.8 cm in size was reported. While the evaluation was going on, the severity of headache was
increased and ophtalmoplegia developed. The patient underwent endoscopic transsphenoidal surgery. The
histopathology of the lesion was consistent with granulamatous reaction with caseous necrosis.
Tuberculosis and sarcoidosis was excluded by PPD, thorax CT, lumbar puncture and analysis of the
cerebrospinal fluid, mycobacterium tuberculosis PCR and the culture of the pathology specimen. The
final diagnosis was Tolosa Hunt.
Conclusion:Tolosa Hunt is a very rare cause of hypophysitis and panhypopituitarism. It should be
considered in the differential diagnosis of a sellar mass.
190 - A case with atypical parathyroid lipoadenoma presented with severe hypercalcemia and skeletal deformities - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 367, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
ABSTRACT
Introduction: Parathyroid lipoadenoma(PLA) is a rarely seen, benign variant of parathyroid
adenoma(PA). However, PA usually consists of uniform, polygonal chief cells with a few nests of
oxyphil cells, PLA consists of similar histologic features, but with an abundance of fat cells.
Additionally, PLA may be functional with the secretion of parathyroid hormone (PTH) or non-
functional. Here, we present a case of atypical PLA presented with severe hypercalcemia and skeletal
deformities.
Case: A 41-year old male referred to emergency department due to the cranial trauma following the
syncope episode. In his cranial magnetic resonance imaging no pathology was found. He had no
chronic disease except hypertension. His laboratory evaluation revealed elevated creatinine and
calcium (Ca) levels (1.7 and 14.3 mg/dl, respectively). PTH level was found 735 pg/ml , urinary
calcium excretion was found 348 mg/24 hour. Neck ultrasound (US) revealed an isoechoic mass with
18.5X29.5X38.7 mm in size in the left inferior part of the thyroid gland which was consistent with
parathyroid scintigraphy. Grade I hypertensive retinopathy was detected in ophtalmological
examination. Bone mineral densitometry revealed severe osteoporosis , especially in lumbal
vertebraes. Pathologic fracture was not determined in vertebral graphics. He had severe scoliosis and
pectus excavatum. Ca levels were regressed to 12 mg/dl with intravenous hydration and diuretic
treatment. He had underwent left hemithyroidectomy and parathyroidectomy and pathology was
revealed atypical PLA and benign thyroid disease. Also the surgical specimen was revealed a large
size mass with a 5 cm in diameter and neoplastic cells were seen in one area in the capsule.
Conclusion: Although PLAs are benign lesions, our case had atypical features. He had severe
osteoporosis and skeletal anomalies in addition to severe hypercalcemia. However, there has been no
known malignant PLA, the cases which show atypical features should be followed closely.
189 - Case report: endoscopic ultrasonography can be used as an adjunctive procedure in atypically localized and conventional ultrasound negative parathyroid adenoma - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 366, Endocrine Abstracts, Volume 41, ISSN 1479-6848
ABSTRACT
Introduction: Ectopic and atypically localized parathyroid adenomas such as in the anterior
mediastinum, paraesophageal or retrotracheal position, although rare, can be seen in clinical practice.
Ultrasound (US) which is a frequently used and one of the best conventional imaging modality
sometimes fails to identify the lesion especially in atypically localized adenomas. Endoscopic US
(EUS) is a new technique that can be used for localization of parathyroid lesions. We reported a case
with paraeosophageal parathyroid adenoma which was localized accurately with EUS.
Case: A 55-years old woman with papillary thyroid microcarcinoma (PTMC) (0.8 cm in size) was
operated 5 years ago. After the thyroid surgery her Ca levels (10.5-11 mg/dl) were found as elevated.
She had been evaluated for hypercalcemia and PTH level was also found elevated. In her neck
ultrasound (US) and parathyroid scintigraphy no pathology was found. Since she had no operation
indication for asymptomatic hyperparathyroidism she had been followed for 5 years. Bone mineral
densitometry revealed osteoporosis in lumbal vertebraes. Neck US found no pathology. Recent
parathyroid scintigraphy revealed parathyroid adenoma in the posterior of the trachea in the inferior
thyroid region. Neck and upper mediastinal computerised tomography showed heterogenous solid
nodular lesion in the superior right paraeosophageal region 11 mm in size. In order to determine the
exact localization of the parathyroid adenoma EUS was performed and detected a hypoechoic lesion
close to esophagus on the right parathyroid localization. The patient underwent parathyroidectomy
with minimally invasive procedure, parathyroid adenoma was detected and excised.
Conclusion: Preoperative localization of parathyroid pathology is important in appropriate cases of
minimal invasive surgery. EUS can be accepted as a tool for detection of parathyroid adenoma. When
the other imaging methods are negative or conflicting, EUS can be considered in these patients
188 - Bilateral large adrenal lesions in a patient with undertreated congenital adrenal hyperplasia - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 317, Endocrine Abstracts, Volume 41, ISSN 1479-6848
ABSTRACT
Introduction: Congenital adrenal hyperplasia (CAH) is a group of autosomal recessive diseases
characterized by enzyme deficiencies in cortisol secretion. The most common form is 21-alpha
hydroxylase deficiency. Here, we report a patient with undertreated CAH and bilateral large adrenal
masses.
Case report: 34 years old male patient diagnosed with CAH and testicular anorchia at the age of 7
admitted to our clinic for general weakness. Hydrocortisone treatment was started at the diagnosis but
he never used it regularly and was not taking glucocorticoid replacement for 10 years. In physical
examination, blood pressure was 100/70 mmHg, there was diffuse hyperpigmentation, and no
testicular tissue could be palpated. In laboratory examination, fasting blood glucose was 97 mg/dL,
sodium 143 mmol/L, K 4.5 mmol/L and renal, liver and thyroid functions were normal. His serum
cortisol, adrenocorticotrophin hormone (ACTH) and 17-OH progesteron levels were 4.8 mcg/dL, 366
pg/mL and 217 ng/mL, respectively. Serum aldosteron was low and and renin was high. In abdominal
MRI, there were hypertrophied adrenal glands with solid nodular lesions of 47x44 mm in right and
22x24 mm in left glands. Pheochromocytoma was excluded by normal 24 hour urinary
catecholamines. 17-OH progesteron decreased to 40.8 ng/mL after 2 months of 0.5 mg/day
dexamethasone treatment.
Conclusion: Although, adrenal enlargement is an expected finding in untreated CAH due to excessive
ACTH secretion, adrenal lesions are rarely observed. CAH should be included in the differential
diagnosis of large bilateral adrenal lesions to avoid unnecessary adrenalectomies.
187 - Acromegaly in a male patient with Kleinfelter syndrome - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP301, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
ABSTRACT
Introduction: Klinefelter syndrome is known as the set of symptoms that result from two or more X
chromosomes in males. There is no known association of this syndrome with GH hypersecretion. The
most remarkable symptom is gigantism and it can also be observed in androgen deficient states as such as
the Klinefelter syndrome and some more genetic syndromes such as the Sotos syndrome, the Marfan
syndrome, the homocystinuria, and the fragile X-syndrome. Herein we presented a case with both
Kleinfelter and acromegaly.
Case: A 40-year- old male with previously known hypergonadotropic hypogonadism due to Kleinfelter
syndrome (47, XXY) was referred to our clinics with the symptoms of increased ring size, arthralgia,
excessive sweating and headache. Physical examination revealed multiple skin tags, mild coarsening of
the facial features, soft fleshy hands and interdental separation. He was 186 cm in height and 82 kg in
weight. In the hormone panel, basal gonadotropins were elevated with low plasma testosterone, spot
growth hormone (GH) was 4.22 μg/ L serum and insulin like growth factor-1 (IGF1) level was 611 μg/ L
which was above the age matched reference range (105-280 μg/L). We performed OGTT with 75 mg
oral glucose and the nadir GH was 1.0 μg/L.MRI scan of the pituitary revealed an adenoma 12 mm in
size. Adenoma was resected with endoscopy guided transsphenoidal approach and the histopathology was
consistent with adenoma stained positive with GH. His IGF-1 was normalized and spot GH was < 1 μg/ L
three months after the operation.
Conclusion: Acromegaloidism was reported in Kleinfelter syndrome which was recognized as a
condition which resembles acromegaly by its clinical manifestations without excess secretion of GH and
somatomedins. Ours was the first Kleinfelter case in the literature diagnosed with acromegaly that means
clinical tests are indicated in the presence of suspicious findings.
186 - A patient with radiological dilemma: hemorrhagic pituitary adenoma or rathke’s cleft cyst? - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016, EP 295, Endocrine Abstracts, Volume 41, ISSN 1479-6848.
ABSTRACT
Introduction: Rathkes cleft cyst is one of the pituitary non-adenomatous tumors that found in about
20% of pituitary glands at autopsy. Symptomatic Rathke’s cleft cysts are rarely, but these cysts can
cause serious medical problems associated with compression of the pituitary gland, pituitary stalk,
optic nerve or hypothalamus. Here, we report a rare case of 73 years old man with sudden onset
headache due to Rathke’s cleft cyst present with symptoms and radiological features like apoplexy of
pituitary adenoma.
Case: A 73-year- old man admitted to our hospital with weight loss and sudden onset headache. His
body mass index were 31.8 kg/m 2 , blood pressure: 120/84 mmHg and 68/min with a regular rhythm.
Neurologic examination was normal. Laboratory findings were as follows: CBC was normal, Serum
sodium: 138 mmol/L, potassium: 4.8 mmol/L, urea nitrogen: 35 mg/dL, creatinine: 1.1 mg/dL, fasting
plasma glucose: 102 mg/dL, hemoglobin A1c: 7.3%. Anterior pituitary function tests were as follows:
morning serum cortisol 0.99 μg/dL, Adrenocorticotrophic hormone (ACTH) 14.2 pg/mL, free T3 1.82
μg/dL, free T4 1.32 μg/dL, thyroid stimulating hormone (TSH) 2.36 mIU/mL, luteinizing hormone
(LH) 1.18 mIU/mL, follicle stimulating hormone (FSH) 2.47 mIU/mL, serum testosterone 0.0025
ng/dL and serum prolactin of 12 ng/mL. His laboratory tests revealed panhypopituitarism. Brain
magnetic resonance imaging (MRI) showed a 20x15 cm sized sellar cystic lesion, which consisted of a
Rathke’s cleft cyst. On the basis of these results, supplementation with thyroid hormone and
glucocorticoid was started. After 1 month of supplementation treatment control MRI showed a 8.7x4.3
cm Rathke’s cleft cyst which was regressed compared to initial imaging.
Conclusion: The neurologic symptoms of endocrinopathies can be associated with Rathke’s cleft cyst
and hemorrhagic pituitary adenoma. The radiological evaluation can be spurious in these patients.
Longer follow-up must be needed in order to confirm the exact diagnosis.
185 - Chronic lymphocytic leukemia in an acromegalic patient. - 2016
Uluslararası Bildiriler 18th European Congress of Endocrinology 2016, Munich, Germany. 28-31 May 2016,EP 271, Endocrine Abstracts, Volume 41, ISSN 1479-6848
ABSTRACT
Introduction: Acromegaly patients are known to have an increased risk of malignancies. This may be
as a result of the effect of insulin-like growth factor I (IGF-I) on cellular proliferation and apoptosis
inhibition. Although there are various reports related with hematological malignancies in children who
treated with growth hormone (GH), few data are available about hematological malignancies in
acromegaly patients. Here, we report a patient with acromegaly who has been developed chronic
lypmhocytic leukemia (CLL) in the follow-up period.
Case: A 30 years old woman who was at 25 th weeks gestation were consulted for gestational diabetes
mellitus 9 years ago. Physical examination, random GH, IGF-I levels and glucose suppression test
results were consistent with acromegaly. She reached full term without treatment, and had a caesarian
section and delivered a 4200-gr- baby boy with Apgar score of 9. After 1 year delivery transsphenoidal
surgery was performed and 3 months after the operation long-acting somatostatin analog treatment
was begun. Since she had residual adenoma and biochemical remission was not achieved with medical
treatment, she had underwent second operation after 1 year later the first surgery. Since the remission
was not achieved despite the medical treatment, after 1 year later the second operation gamma-knife
therapy has been performed. After 5 years later the radiotherapy, GH and IGF-I levels were decreased
gradually, somatostatin therapy was lowered and finally discontinued. However, the patient had
progressive leukocytosis with 90% lymphocytes. Flowcytometric analysis of the peripheral blood was
consisted with CD5+, CD19+, CD20+, CD22+, CD79b+, CD43+, CD200+ lymphocytes with surface
anti-kappa monoclonality. Fluorescent in situ hybridization analysis of bone marrow aspiration
revealed 20% deletion 17p13.1(TP53). Her findings were consistent with CLL-stage II.
Conclusion: Occurrence of CLL in the course of acromegaly may have been caused by excessive
endogenous GH or may be a coincidental situation.
183 - Hypocalcaemia development in patients operated for primary hyperparathyroidism: can it be predicted preoperatively? - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, GP 1102, Endocrine Abstracts, Volume 37, ISSN 1479-6848
ABSTRACT
Introduction: Primary hyperparathyroidism (PHP) is a highly prevalent disease, which is treated most
effectively by surgery. Postoperative hypocalcemia, a morbidity of surgical treatment of
parathyroidism, can prolong the hospital stay. The aim of this study was to identify the factors
predictive of hypocalcemia and hungry bone syndrome (HBS) in patients who undergo
parathyroidectomy due to PHP.
Materials and methods: Preoperatively and on days 1 and 4, and month 6 postoperatively, the
patients’ laboratory data including parathyroid hormone (PTH), calcium, phosphorus, 25-hydroxy D 3
(25-OHD), albumin, magnesium, alkaline phosphatase (ALP), blood urea nitrogen (BUN), and thyroid
stimulating hormone (TSH, free T3 and free T4 levels; and neck ultrasonography (US) and bone
densitometry findings were recorded.
Results: Hypocalcemia was observed in 63 (38.4%) of 164 patients on day 1 following
parathyroidectomy. On the postoperative 6 th month, permanent hypocalcemia was present in 10 (6.1%)
patients. HBS was observed in 22 (13.4%) of the patients who underwent parathyroidectomy due to
PHP. Among the PHP-related parathyroidectomy patients, postoperative hypocalcemia was observed
more frequently among patients with parathyroid hyperplasia and those with osteoporosis. On the
other hand, PTH, ALP and BUN values were higher among patients who developed HBS.
Additionally, HBS was observed more frequently among osteoporosis and parathyroid hyperplasia
patients and those who had thyroidectomy simultaneously with parathyroidectomy.
Conclusion: As a result, a more thorough preoperative follow-up is recommended for patients with
risk factors for hypocalcemia and HBS development.
181 - The evaluation of demographic features and histopathological results in patients with reoperative thyroid surgery - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 924, Endocrine Abstracts, Volume 37, ISSN 1479-6848
ABSTRACT
Objective: Reoperative surgery for thyroid disease is rare. It is sometimes indicated for nodular
recurrence after partial surgery for initially benign thyroid disease or for a completion total
thyroidectomy when a final diagnosis of thyroid cancer is confirmed on a permanent section of a
partially removed thyroid gland. We aimed to investigate the demographic features and reoperation
indications in patients with reoperative thyroidectomy.
Material and Method: Thirty-six patients reoperated between 2008-2011 were included into the
study. Demographic features, indications of reoperation and histopathological results of patients were
evaluated retrospectively.
Results: After reoperative thyroidectomy, the results of histopathological evaluation of 24 patients
were malignant (19 papillary thyroid carcinomas, 3 follicular thyroid carcinomas, 1 Hurthle cell
neoplasm and 1 neoplasm with undetermined malignant potential) while 12 patients were benign. Of
36 patients, 11 (30.5%) went to reoperation due to giant thyroid nodule (>4 cm), 5 (13.9%) due to ≥ 2
nondiagnostic fine needle aspiration biopsy (FNAB), 3 (8.3%) due to toxic multinodular goitre, 5
(13.9%) due to malignant cytology, 2 (5.6%) due to suspected malignancy, 2 (5.6%) due to suspicion
for a follicular neoplasm, 3 (8.3%) due to follicular lesion of undetermined significance, 1 (2.8%) due
to atypia of undetermined significance, 1 (2.8%) due to suspected Hurthle cell neoplasm and 3 (8.3%)
due to cytology of cellular adenomatoid nodule and ultrasonography suggesting malignancy.
Conclusion: Thyroid surgery may lead to regional scars and some degree of fibrotic process. This
may result in problems in collecting thyroid FNAB samples and assessing cellular abnormalities. Our
study findings demonstrated that histopathological evaluation of 14 patients whose cytological results
showed no malignancy, was consistent with malignancy. We consider that decision for reoperative
thyroidectomy should not be made with cytological findings, but patients’ symptoms and ultrasound
findings should also be taken into account.
180 - Ratio of lymph node aspiration washout thyroglobulin levels to whole blood and serum washout thyroglobulin levels in patients with differentiated thyroid carcinoma: a new approach for standardisation of measurements and increased accuracy - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 908, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Introduction: High values of fine needle aspiration washout thyroglobulin (FNA-Tg) are diagnostic
for metastatic lesions of thyroid cancer. However, there is not a consensus on cut-off for high Tg level.
The most important confounding factor for FNA-Tg is inability to calculate Tg per unit volume
because residual aspiration material in the needle cannot be known exactly. Another problem is
possible contamination of whole blood during lymph node aspiration. In this study, we aimed to
determine a more accurate and standardised parameter for FNA-Tg.
Methods: Ultrasonographically suspicious 155 lymph nodes in 120 patients with histopathologically
confirmed differentiated thyroid cancer and suspicious for malignancy/malignant thyroid nodule FNA
result in cytology were evaluated. Tg was measured in samples obtained by aspiration (FNA) and non-
aspiration (FNNA) biopsy. The highest value obtained by these methods from the same lymph node
was defined as FNB-Tg. Simultaneous venous blood sample was taken. Tg was measured from whole
blood and serum washouts which were obtained by using syringes and needles identical to ones used
for lymph node biopsy.
Results: Data of 16 lesions in 14 patients who underwent lymp node dissection were analysed.
FNNA-Tg, FNB-Tg/whole blood washout-Tg, FNB-Tg/serum washout-Tg, FNB-Tg/serum Tg were
significantly higher in malignant lymph nodes compared to benign ones. Areas under the ROC curve
for FNNA-Tg, FNNATg/whole blood washout-Tg, FNNA-Tg/serum washout-Tg were statistically
significant for the discrimination of benign and malignant lymph nodes. Best cutoff values for FNNA-
Tg and FNB-Tg were 15.86 and 31.8 ng/ml. respectively. Among ratios, best cut off values to
discriminate benign and malignant lymph nodes were 5.44 for FNB-Tg/whole blood washout-Tg and
3.95 for FNBTg/serum washout-Tg.
Conclusion: Determining ratio of FNB-Tg to whole blood washout-Tg and/or serum washoutTg
might be a promising method for increasing accuracy and providing standardization of lymph node
aspiration to detect malignant lymph nodes.
179 - Simultaneous occurrence of different follicular neoplasms within the same thyroid gland: a retrospective study - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 876, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Introduction: Neoplasms of the thyroid gland are classified according to the cell that it originates and
commonly they originate from follicular or parafollicular C cells. The most common differentiated
thyroid cancers (DTC) are papillary and follicular carcinomas. Coexistence of two different
histological types of primary follicular thyroid neoplasm is a rare condition. There are previous reports
of concomitant medullary and papillary thyroid cancers .However there is scarce data about the
simultaneous two different histological types of primary follicular thyroid tumors and this is the first
study on that subject.
Method: From January 2007 to September 2014 , our instutional database was reviewed for patients
who underwent thyroid surgery for various indications. Medical records and cytopathology reports of
those patients were examined retrospectively. Simultaneous neoplasms of follicular origin were noted.
Results: A total of 3700 patients were operated. Histopathological examination result was benign in
2686 (73%) patients while it was malignant in 1014 (27%) patients. Among the patients with the
diagnosis of DTC only 20 (1.9%) had accompanying second neoplasia within the same thyroid gland.
PTC had thyroid capsule invasion in seven patients (35%) while capsule was intact in thirteen (65%).
In seventeen (85%) patients there wasn’t vascular invasion whereas in three patients (15%) vascular
invasion was detected in PTC. Second neoplasm was follicular carcinoma in 10 patients, Hurthle cell
carcinoma in 2 patients, Hurthle cell adenoma in 5 patients and follicular adenoma in 3 patients.
Conclusion: Such simultaneous tumors may be part of a familial tumor syndrome or an unidentified
novel gene mutation playing role in the pathogenesis of more than one type of tumor. Based on the
current evidence the synchronous occurrence of those neoplasms in a given patient is likely
coincidental in the literature. Further study is required using a larger patient population with
standardized genetic characterization.
178 - Association of hormonal changes with disease severity and mortality rate in critically ill patients - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 771, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
INTRODUCTION: Endocrinological and metabolic changes can occur in critically ill patients, which
may affect the prognosis and outcome. The hypothalamic-anterior pituitary axis (HPA) plays a crucial
role in the endocrine regulation of metabolic and immunological homeostasis. In this prospective
study, we evaluated the pituitary-adrenal-gonadal-thyroid axis in the adult ıntensive care unit (ICU)
patients ,their outcome, the association between these hormonal changes and “The Acute Physiology
and Chronic Health Evaluation II score (APACHE II)”, Sequential Organ Failure Assessment (SOFA),
length of hospitalization and mortality.
METHODS: Patients hospitalized in adult ICU (not for trauma or operation) between January 2014
and January 2015 were enrolled in this study. Severity of illness was assessed by APACHE II and
SOFA on admission to the ICU and 15 days later. Blood samples were collected within the first 4
hours of ICU admission and 15 days later for measurement of anterior pituitary and end organ
hormones.
RESULTS: Total patient number was 157. Eighty five patients were in survival (S), 72 patients were
in the non-survival (NS) group. In the NS group, patients’ mean age, APACHE II and SOFA scores at
the admission were significantly higher. In the NS group median GH, E2, cortisol levels were
significantly higher whereas median FSH, LH, fT3, fT4 were lower. Fifteen days after admission,
there was significant increase in median IGF-I and ACTH levels and decrease in median cortisol and
SOFA scores compared to baseline values. Strongest predictors for mortality were found to be
hospitalization length, SOFA score, deltaTSH and age. None of the other endocrine parameters had an
effect on mortality.
CONCLUSION: In critical illness, activation of the HPA and the cortisol response are essential for
survival. Combinations of endocrine parameters may provide better indices than measurement of a
single hormone or an APACHE II-based score.
177 - Differentiated thyroid cancer in patients with prolactinoma - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 740, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Introduction: Increasing evidence is available for the role of prolactin in the development of various
cancers. The purpose of this study is to evaluate the frequency of thyroid cancer in patients with
prolactinoma followed up at a single site.
Materials and methods: Medical records of 182 patients, diagnosed with prolactinoma, were
reviewed retrospectively. Out of these patients, 114 patients (103 female patients,11 male patients,
mean age 35 ±10.4), who had undergone thyroid ultrasonography (US), were included in the study.
Serum prolactin, anti-thyroglobulin (antiTg), anti-thyroid peroxidase antibody (anti TPO),thyroid
stimulating hormone (TSH), free T4 (fT4), free T3 (fT3) values, and pituitary gland magnetic
resonance imaging (MRI) and US reports were evaluated.
Results: It was found that 45(39.5%) patients had thyroid nodule (13 solitary, 32 multiple). 10 patients
were administered thyroidectomy, and differentiated thyroid cancer (DTC) was detected in 6 of these
patients (5.3%).1 patient had lung metastasis. Control group consisted of 113 individuals (101
females, 12 males, mean age 32.1±9.1).In US, 28 of these individuals (24.8%) had thyroid nodule (5
solitary, 23 multiple). 1 individual (0.8%) had DTC.
Conclusion: When compared to control group, thyroid volume and thyroid nodularity were
significantly higher in patients with prolactinoma (respectively, p<0.001, p=0.018), however, no
statistically significant difference was available for the incidence of thyroid cancer (p=0.196).
176 - Mean platelet volume in patients with prolactinoma - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 739, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Introduction: Prolactin is a multifunctional pituitary hormone. The effect of prolactin on platelet
activation is not well understood. Prolactinomas are the most common type of pituitary adenomas, and
they are medically responsive to dopamine agonists. Mean platelet volume (MPV) is a marker of
platelet function and activation. The aim of this study was to evaluate MPV values before and 6
months of cabergoline treatment when normoprolactinemia was achieved.
Methods: A total of 101 newly diagnosed prolactinoma patients and 102 healthy control subjects were
included in the study. Patients with hematological disorders that affect MPV and those on medications
were excluded. Prolactin, platelet count and MPV levels were recorded before and 6 months after the
initiation of cabergoline treatment (0.5 to 1 mg, two times a week).
Results: There was no significant difference in platelet count and MPV before and after 6 months of
treatment with cabergoline in patients with prolactinoma compared with the control group (p>0.05).
Conclusion: Our results showed that MPV, a marker of platelet function, was unchanged in patients
with prolactinoma.
175 - Urinary metanephrine levels can be spurious in the diagnosis of patients with phaeochromocytoma: preliminary results from a single centre - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 65, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Introduction: Pheochromocytomas (PHEO) are catecholamine producing tumors that are mostly
adrenal in origin. PHEO is diagnosed with classic findings and symptoms but biochemical
confirmation must be made and followed by anatomical localization. PHEO can also be associated
with adrenal incidentalomas (AI). All of the patients with AI must be evaluated for PHEO
biochemically. Either urinary or plasma chatecholamines and metanephrines can be used for
biochemical evaluation. Normal values rule out the diagnosis, whereas four fold increase above the
upper limit of normal confirm the diagnosis. But value of borderline or less than 4 fold elevations in
the diagnosis is not clear. We aimed to determine the urinary fractionated metaneprine and
catecholamine levels in patients with PHEO.
Material and Methods: Thirteen patients who underwent adrenalectomy and finally diagnosed as
PHEO and 10 age- and sex- matched AI patients who underwent to adrenalectomy based on size
criteria, preoperative hormonal test results and finally diagnosed as benign neoplasm between January
1, 2008, and January 1, 2015 were evaluated retrospectively.
Results: Of the 13 patients with a pheochromocytoma on final pathologic diagnosis, VMA levels
were as follows: 3 (23.1%) patients had borderline elevations, 1 patient (7.7 %) had 2 fold elevations,
1 patient had 3 fold (7.7%), 1 (7.7%) had 4 fold , and 3 (23.1%) patients had 6 fold elevations above
the upper limit of normal. However, 4 (30.8%) patients had normal VMA values. For non-PHEO
group 4 (40%) patients had borderline elevations, and 6 (60%) patients had normal values. There was
no statistically significant difference between PHEO and non-PHEO groups (p=0.42). For PHEO-
group urinary HVA values were as follows: 2 (16.7%) had borderline elevations, 10 (83.3%) had
normal values. In 1 patient it was not evaluated. For non-PHEO group, 1 (10%) had 2 fold, 1 (10%)
had 6 fold elevations, and 8 (80%) had normal values. There was no significant difference for HVA
(p=0.70). Urinary metaneprines were as follows: 3 (25%) had borderline elevations, 9 (75%) had
normal values in PHEO-group, however 1 (10%) had borderline elevation, 1 (10%) had 6 fold
elevations, 8 (80%) had normal values. The difference was evaluated as statistically insignificant
(p=0.19). Normetanephrine values were as follows: borderline elevation in 5 (41.7%), 2 fold elevation
in 1 (8.3%), 6 fold elevation in 1 (8.3%) and normal values in 5 (41.7%) patients in PHEO-group;
borderline elevations in 2 (20%) , 2 fold elevation in 1 (10%), normal values in 7 (70%) patients in
non-PHEO group. This was also statistically insignificant (p=0.39). There were also no statistically
significant differences in urinary adrenalin and noradrenalin levels between groups.
Conclusion: Patients with borderline -elevated urinary metanephrine levels can also have PHEO. In
patients with AI who are candidate for surgery and have borderline elevated metaneprines should be
evaluated carefully. In this group of patients, we advocate either routine preoperative preparation as
patients possessing PHEO or further diagnostic tests in order to prevent the serious complications.
173 - Evaluation of clinical and biochemical features of patients with atypical parathyroid adenoma: a retrospective study 1 - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 304, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Introduction:Primary Hyperparatyhyroidism (PHPT) is usually caused by single or multiple
adenomas and cancer is rare accounting for less than 1 % of all presentations. The presence of certain
cytological, and architectural features such as adherence to adjacent organs, a solid growth pattern,
broad bands of fibrosis, cytological atypia, and an irregular growth contour do not indicate malignancy
but are recognized as atypical features encountered more commonly in malignant than benign tumors.
Tumors that demonstrate these atypical features and do not fulfill criteria for carcinoma can be
classified as atypical adenomas. Herein we aimed to evaluate the clinical and biochemical features of
the patients histopathologically diagnosed with an atypical parathyroid adenoma.
Method:Our endocrine database was searched retrospectively for the patients with operated PHPT and
diagnosed with atypical adenoma. Demographic, clinical and biochemical data of the patients were
recorded. A control group was formed from the patients who were also operated with the diagnosis of
PHPT and classical parathyroid adenoma was detected histopathologically.
Results:There were sixteen patients in the atypical adenoma group and thirty patients in the control
group. Age and gender distribution of the patients were similar in between groups with female
predominance. Serum Ca and P levels were also similar where as preoperative serum PTH, ALP and
urinary Ca excretion were significantly higher in patients with atypical adenoma (p<0.001, p<0.001
and p=0.021, respectively). Adenoma size was significantly higher in the atypical adenoma group
compared to controls (p=0.006) and cystic degeneration and isoechoic appearance on USG were more
prevalent among the atypical adenomas (p=0.016).
Conclusion:Preoperatively high PTH, ALP and urinary Ca levels may be predictive for atypical
adenoma or carcinoma within a patient being evaluated for PHPT. The surgeon might prefer enbloc
parathyroidectomy instead of minimal invasive surgery in such cases with more strict postoperative
follow up.
172 - The diagnostic value of parathyroid hormone washout in primary hyperparathyroidism patients with negative or unequivocal 99mTc-MIBI results - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 279, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Introduction: Primary hyperparathyroidism (pHPT) is a common endocrine disease mainly caused
by single or multiple hyperfunctioning parathyroid lesions. In 2% to 7% of cases, surgery is not
curative at first operation and reoperation is required. Ultrasonography and sestamibi scan are the most
widely used methods for identification of the the culprit parathyroid gland with the disadvantage of
high false positives caused by other cervical pathologies. Herein we aimed to search the diagnostic
value of measurement of parathyroid hormone (PTH) concentration in the needle washout of
suspicious lesions suggestive for parathyroid adenoma with negative or unequivocal MIBI results.
Methods: Our endocrine database was searched retrospectively for the patients with PHPT who
underwent PTH washout. There were 100 lesions of 70 patients. Among them, 21 lesions in 16
patients were operated and data of these lesions were analyzed. All patients had at least one suspicious
parathyroid lesion detected by ultrasonography and all patients were evaluated by 99mTc-MIBI.
Result: The mean age of the patients was 53.3±10.6 years with the majority of them being female
(87.5%). The mean preoperative serum calcium level was 11.04±0.33 mg/dl. The median serum PTH
level was 140 pg/ml (ranging from 55 to 371) and the median serum PTH washout level was 3316
pg/ml ranging from (13 to 5000 ). Preoperatively 99mTc-MIBI scan was negative or unequivocal in
15 of 21 operated lesions while it was positive in 6. For the lesions that the MIBI failed to localize, the
sensitivity of PTH washout was 91% and the specifity was 66%.
Conclusion: PTH washouts can contribute significantly in establishing the parathyroid nature of
cervical lesions that has conflicting preoperative sestamibi results and also might help the surgeon to
perform a more succesful operation.
171 - A case of a mitochondrial myopathy with multiple endocrinopathy - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 270, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Introduction: Mitochondrial diseases usually occur by mutations of mitochondrial or nuclear DNA.
Mitochondrial cytopathy is a disease affecting many systems including endocrine system. We present
a case diagnosed as mitochondrial myopathy previously accompanying multiple endocrinological
pathologies.
Case : Fifty-two years old female patient admitted in another center with a complaint of drooping of
upper eyelids 25 years ago. Acetylcholine receptor antibodies were negative and her EMG was
compatible with progressive external ophthalmoplegia. She was diagnosed as mitochondrial myopathy
by left biceps muscle biopsy. Coenzym Q 10 and L-carnitine treatments were started. She admitted to
our center with numbness and spasm in her hands. Serum calcium was 6.1 mg/dl, phoshorus was 6.9
mg/dl, magnesium was 1.5 mg/dl and parathyroid hormone level was 8.9 pg/ml. There were common
symmetric calcifications at basal ganglions, bilateral cerebellar hemispheres, thalamus and
periventricular white matter in cranial CT. EEG was normal. Creatine kinase was 507 U/l, LDH was
435 U/l and plasma lactate level was 2.4 mmol/l. Calcium carbonate and calcitriol were administered
to the patient with diagnosis of hypoparathyroidism. Thyroid autoantibodies were positive. Thyroid
hormone levels were normal. Thyroid ultrasound was compatible with chronic thyroiditis. In eye
examination bilateral ptosis and cataract were detected. Retina examination was normal. Her
audiometry was normal. She was diagnosed as type 2 DM.
Conclusion: Mitochondrial myopathies can be together with various endocrinological problems. Our
patient had adult onset pure mitochondrial cytopathy and primary hypoparathyroidism, chronic
autoimmune thyroiditis and type 2 DM were accompying endocrinological pathologies. Associations
with hypoparathyroidism, autoimmune thyroiditis, DM and GH deficiency have been reported in
patients with Kearns Sayre syndrome in the literature. Also mitochondrial myopathy, encephalopathy,
lactic acidosis, stroke (MELAS) and adrenal insufficiency’s association was reported. Because of
probability of affecting multisystem, cases with mitochondrial myopathies should be evaluated for
various endocrinological pathologies.
170 - Evaluation of most common symptoms and findings in Turkish adolescent girls with polycystic ovary syndrome - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 179, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Objective: Polycystic ovary syndrome (PCOS) is a complex endocrinopathy affecting 5-10% of
women in reproductive period. Our goal is to determine which symptoms and findings are the most
common in Turkish adolescents with PCOS.
Material and method: Ninety three adolescents (15-19 years old) who admitted to our outpatient
clinic with at least one of the complaints (acne, obesity, menstrual irregularities and hirsutism) were
enrolled in the study. All patients were evaluated due to both Rotterdam and NIH criteria.
Results: Due to Rotterdam and NIH criteria 40 (43.01%) and 32 (34.40%) of patients were diagnosed
as PCOS respectively. Due to Rotterdam menstrual irregularities were 90%, hirsutism was 45%,
obesity was 25% and acne was 32.5% in patients diagnosed as PCOS. Due to NIH these ratios were
96.9, 50, 25 and 31.3% respectively. Patients were divided into 12 subgroups due to combinations of
complaints. Due to Rotterdam, PCOS diagnosis were 100% for menstrual irregularities and hirsutism
together, 75% for menstrual irregularities and acne together, 66.7% for menstrual irregularities and
obesity together, 66.7% for only hirsutism, 50% for hirsutism and acne together, 40% for only
menstrual irregularities, 3.7% for only acne and 0% for only obesity. Due to NIH, PCOS diagnosis
were 100% for menstrual irregularities and hirsutism together, 66.7% for menstrual irregularities and
acne together, 44.4% for menstrual irregularities and obesity together, 33.3% for only hirsutism,
26.7% for only menstrual irregularities, 0% for only acne or only obesity. Eight patients were
diagnosed as PCOS only due to Rotterdam.
Conclusion: The most common complaints in Turkish adolescents with PCOS were menstrual
irregularities, hirsutism, acne and obesity in our study. According to guidelines PCOS in adolescents is
based on clinical and/or laboratory hyperandrogenism together with persistent oligomenorrhoea.
Polycystic ovarian morphology can be a part of reproductive changes in adolesce
169 - 47,XYY syndrome and hypogonadotropic hypogonadism: is this coincidence or a diverse spectrum of the syndrome? - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 174, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Introduction: 47,XYY syndrome is characterized by an extra copy of the Y chromosome in each cells
of a male. It occurs in about 1/1,000 of newborn boys and most males with this syndrome have normal
sexual development and fertility. They tend to have tall stature and mild motor and language
developmental problems. Testosterone levels are normal. Increased rate of criminal activity in XYY
males was related to a lack of judgement and lower socioeconomic status due to a lower mean IQ
score.
Case report: A 21 year-old- man applied to our clinic with complaints of small testis and penis and,
lack of beard and ejaculation. He had normal libido and erection. There was no family history of
infertility. He hadn’t commited any crime. In physical examination, he had eunuchoid habitus, his
height was 178 cm, weight was 66.6 kg, and BMI was 21 kg/m 2 . His testes were palpable in the
scrotum. Axillary and pubic hair development was consistent with Tanner stage 4. Penis length was
6.5 cm. His neurocognitive development and functions were normal. Hormonal tests revealed
hypogonadotropic hypogonadism. Other hypophyseal hormons were normal. Bone age was
compatible with 14 years and epiphyseal plates were open. In testicular ultrasonography, volumes
were 8 ml on the right and 7.5 ml on the left. Hypophyseal MRI showed partially empty sella. In
chromosomal analysis, 47,XYY karyotype was detected. After administration of human chorionic
gonadotropin treatment, androgen levels increased and ejaculation started although in small amounts
(<0.5 ml).
Conclusion: Men with 47,XYY syndrome have a diverse spectrum of clinical presentation and
because of the heterogeneous phenotype and lack of spesific symptoms, its diagnosis may be difficult.
As presented in our case, hypogonadotropic hypogonadism might be a presenting feature in patients
with 47,XYY genotype.
References:
1. Kim IW, Khadilkar AC, Ko EY, Sabanegh ES Jr. 47,XYY Syndrome and Male Infertility. Rev
Urol. 2013;15(4):188-96. Review.
2. El-Dahtory F, Elsheikha HM. Male infertility related to an aberrant karyotype, 47,XYY: four
case reports. Cases J. 2009 Jan 8;2(1):28. doi: 10.1186/1757-1626- 2-28.
3. Visootsak J, Graham JM Jr. Social function in multiple X and Y chromosome disorders:
XXY, XYY, XXYY, XXXY. Dev Disabil Res Rev. 2009;15(4):328-32. doi: 10.1002/ddrr.76.
4. Ceylan GG, Ozbey U, Yüce H, Elyas H. 47,XYY Sendromlu Bir Olgu. Fırat Tıp Dergisi
2007;12(3): 239-242
168 - Clinical and hormonal characteristics of a series of patients affected by inappropriate TSH syndrome: insights into the differential diagnosis - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 1277, Endocrine Abstracts, Volume 37, ISSN 1479-6848
ABSTRACT
Introduction:Normal or elevated TSH level in the presence of elevated T4 is defined as
“inappropriate TSH syndrome”.Two main clinical conditions that can lead that syndrome are TSH
secreting adenoma (TSHoma) and resistance to thyroid hormone (RTH). Making the correct diagnosis
is crucial in order to decide the most appropriate treatment option. Herein we presented clinical and
laboratory data of seven patients who were hospitalized for the differential diagnosis of the two
clinical entities.
Method:Our database was reviewed for the patients diagnosed with inappropriate TSH syndrome at
our hospital between 2010-2014. After exclusion of the other rare causes of inappropriate TSH
syndrome, seven patients who were hospitalized for the differential diagnosis of TSHoma and RTH
were included in this report
Result:Age of the patients was changing between 20 and 52 years. Clinically two patients were
asymptomatic, three had tachycardia and weight loss and one had goiter. Final diagnosis was RTH in
four patients, TSHoma in two and unequivocal in one. Two patients diagnosed with TSHoma were
operated and had positive staining with TSH. Both of the TSHoma cases had macroadenoma on
pitiutaryMRI and visual field defect while two of four patients with RTH had microadenoma. Alpha-
subunit/TSH molar ratio was above 1 in all patients diagnosed with TSHoma while it exceeded 1 in
two patients with the final diagnosis of RTH. TRH stimulation test revealed a blunted response in all
patients with TSHoma and a positive response (increase >100%) was observed in all with THR. TSH
was suppressed after T3 supression test in all patients with the final diagnosis of RTH.
Conclusion:Differential diagnosis of RTH and TSHoma can be a clinical challenge and requires
complex hormonal tests and imaging methods. Since incidental pituitary tumors are not rare, presence
of an adenoma should not rule out diagnosis of RTH.
166 - Successful systemic treatment of Xanthoma disseminatum with cyclophospamide: an interesting case with endocrine and gastrointestinal involvement. - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 1228, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Introduction: Xantoma disseminatum (XD) is a rare non-Langerhans cell histiocytosis (NLCH)
which is often resistant to treatment.In this report, we presented a case with extensive cutaneous,
hypothalamohypophysial, cerebral and gastrointestinal system involvement, which responded well to
cyclophosphamide.
Case: A sixteen-year- old female patient admitted to our hospital with the complaints of amenorrhea,
weight gain, polidipsia, poliuria, yellow-brownish papular lesions on the cervical, periorbital, axillary
and genital regions. Lesions first appeared 18 months ago and increased in amount and size in time.
Hormonal evaluation was done including dynamic tests and secondary hypothyroidism,
hypogonodothropic hypogonadism, growth hormone deficiency and central diabetes insipidus were
detected.Pituitary MRI demonstrated a mass 15x8 mm in diameter at hypothalamohypophysial tract
together with multiple cerebral lesions. Her visual and neurologic examination was normal. A biopsy
was performed on skin and duodenal lesions and the result of pathologic analysis was coherent with
NLCH. In the light of those findings, she was diagnosed with XD. Hormonal replacement therapies for
hypothyroidism, hypogonadism and DI were initiated. For hypothalamic mass and skin lesions 60
mg/day methyl prednisolone was started and its dosage was gradually reduced to maintenance dose of
4 mg/d. MRI screening performed at 6th month of therapy didn’t show any regression in mass sizes.
Hence, medical therapy was changed with cyclophosphamide 100 mg/d. No complete remission was
achieved but significant regression in cutaneous, hypothalamohypophysial, cerebral and
gastrointestinal lesions was obtained in 24 months. No side-effects were noticed related with
cyclophosphamide. The skin lesions did not relapse after discontinuation of cyclophosphamide.
Conclusion: The coexistence of XD with hypopituitarism is a rare condition. There are various
systemic treatments such as radiotherapy, cryotherapy, corticosteroids, and antiblastic chemotherapy
but no single treatment is universally successful.In rare cases complete remission was obtained with
low-dose oral cyclophosphamide in adults as it occurred in our case.
165 - A case of pleomorphic adenoma and acromegaly: a coincidence or a pathophysiological association? - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 1210, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Introduction: Acromegaly is a chronic disease caused by excessive secretion of growth hormone
(GH), and as a result, of insulin-like growth factor -1 (IGF-1). Although controversial, frequency of
both benign and malignant neoplasm formation is thought to be increased in acromegalic patients.
Pleomorphic adenoma is the most common arising tumor from the parotid salivary gland. Here we
report the case of a 33-year- old woman with acromegaly and also who presented with a swelling on
the left neck and diagnosed as pleomorphic adenoma arising from parotid gland after excision of the
tumor.
Case report: Thirty three-year- old woman admitted to the hospital complaining of a two-weeks
history of visual loss and headache. She also determined weight gain, menstrual irregularity, libido
loss, galactorrhea, and a slowly growing swelling on the left neck during the last year. Hypophyseal
MRI revealed a mass of 20x32 mm occupying the sellae and invasing right cavernous sisternae and
extending to the optic chiasm. Hormonal evaluation demonstrated that the patient had acromegaly and
secondary hypothyroidism. Parotid ultrasound (US) revealed a 42x28x45 mm heterogenous,
hypoechoic intraglandular lobulated solid mass occupying left parotid gland superficial lobe and
extending to the deep lobe. Hypohpyseal adenoma was excised by transsphenoidal route and
immunohistochemical analysis showed extensive GH positivity. She had residual tumor after the
operation and somatostatin analogous therapy was started in the follow-up period. After eight months
from the hypophyseal operation the parotid tumor was excised and pathology showed that it was a
pleomorphic adenoma.
Conclusion: It seems that this is the first case of a coincidence between an acromegaly and
pleomorphic adenoma of parotid gland in the English literature. We don’t have still enough knowledge
about an association between salivary gland tumors and acromegaly. If present or not this association
must be evaluated with the further studies.
164 - Positive MIBG scan in a patient with adrenal failure secondary to lymphoma: a coexistent paraganglioma or false positive involvement - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 1174, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
162 - Intraocular pressure, corneal, and retinal thickness in patients with euthyroid autoimmune thyroiditis - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 1080, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Aim: Ocular changes and ocular symptoms may be encountered in patients with hypothyroidism and
hyperthyroidism. However, the data concerning the effects of thyroid disorders on intraocular pressure
(IOP), central corneal thickness (CCT) and retinal thickness (RT) are very rare. Here, we aimed to
evaluate the alterations in IOP, CCT and RT in patients with euthyroid autoimmune thyroiditis (AIT).
Material- Methods: Twenty-five subjects with euthyroid AIT were included into the study. The
patients were compared with age and sex-matched 40 healthy subjects. A detailed ophthalmologic
examination including the IOP, CCT and RT was performed in both groups.
Results: There was no statistically significant difference in mean right RT, left RT, right CCT and
left CCT between two groups (p>0.05 for all parameters). Also, no significant difference was found
between groups concerning right and left IOP (p>0.05 for all parameters). In patients groups, left RT
was significantly higher in patient with TSH>2.5 µIU/mL than those of TSH< 2.5 µIU/mL
(294.85±23.58 vs 261.50 ±21.70, p=0.003). A positive correlation was observed between left RT and
thyrotropin levels (r=0.269, p=0.033). No significant correlation was found between free
triiodothyronine levels, and right CCT, right RT, right IOP, left CCT, left RT and left IOP levels
(p>0.05 for all parameters). Also, free tetraiodothyronine levels were not significantly correlated with
right CCT, right RT, right IOP, left CCT, left RT and left IOP levels (p>0.05 for all parameters).
Conclusion: An increase in IOP in Graves ophthalmopathy (GO) is a well-known entity. In literature,
hypothyroidism seems to cause a reversible increase in CCT and IOP. In this study, we observed no
significant difference between groups concerning IOP, CCT and RT. So, further studies with larger
sample size are needed to evaluate IOP, CCT and RT in patients with euthyroid AIT.
161 - Ultrasonographical and cytological features of exophytic thyroid nodules: do exophytic nodules pretend to be malignant? - 2015
Uluslararası Bildiriler 17th European Congress ofEndocrinology 2015, Dublin, Ireland. 16-20 May 2015, EP 1075, Endocrine Abstracts, Volume 37, ISSN 1479-6848.
ABSTRACT
Aim: Exophytic nodule refers to a nodule that sticks out of the normal thyroid boundary/outline. Other
definition is a nodule with an acute angle between the lesion and adjacent thyroid capsule. Exophytic
configuration is not known risk factor for thyroid cancer. We aimed to compare ultrasonographical
features and cytopathologic results of exophytic and non-exophytic thyroid nodules.
Material and method: Fourty-four exophytic and 34 non-exophytic thyroid nodules in which fine
needle aspiration biopsy was indicated throughout 3 months were evaluated prospectively. Mean
nodule size was similar in two groups (18.83±8.71 mm and 15.28±7,57 mm, p=0.173). The ratio of
presence of peripheral hypoechoic halo and marginal irregularity was also similar in both group
(p=0.512 and p=0.153, respectively). Microcalcification was present in 21.4% and 29.4% of exophytic
and non-exophytic nodules, respectively (p=0.424). Macrocalcification was detected in 4.5% of
exophytic and 11.8% of non-exophytic nodules (p=0.111). 47.6% of exophytic nodules was
hypoechoic and 52.4% was isoechoic. 47.1% of non-exophytic nodules was hypoechoic and 52.9%
was isoechoic. Color flow doppler pattern was defined as non-vascular, peripheral, central, or of
mixed type and was similar in both groups (p=0.138). Cytopathologic results of exophytic nodules
were 75% benign, 4.3% follicular lesion or atypia with undetermined significance, 2.3% suspicious for
malignancy, 2.3% malign, and 15.9% non-diagnostic. In non-exophytic group, 79.4% was benign and
20.6% was non-diagnostic (p=0.497).
Conclusion: Exophytic configuration of thyroid nodules was rarely investigated as a possible
predictive feature for malignancy in the literature. In the literature, only one study evaluated exophytic
feature of thyroid nodules in neck CT (1). They reported malign thyroid nodules had more frequently
exophytic configuration than benign ones without statistical significance. In our study, we did not find
any difference in terms of ultrasonographical features and cytological results between exophytic and
non-exophytic thyroid nodules. However, more comprehensive studies with larger sample sizes are
needed to clarify any possible relation between exophytic configuration and malignancy.
References:
1.Kim DW, Jung SJ, Baek HJ. Computed tomography features of benign and malignant
solid thyroid nodules. Acta Radiol. 2014 Oct 7. pii: 0284185114552216. [Epub ahead of print]
159 - The association of NIS and BRAFV600E Mutation in classical variant papillary carcinoma - 2015
Uluslararası Bildiriler USCAP 104th Annual Meeting 21-27 Mar 2015, Boston USA. Poster No: 562 (Modern Pathol Vol 28, Suppl 2, Feb 2015)
ABSTRACT
Background: Functional expression of sodium iodide symporter (NIS), a membranetransporter of iodine is essential for postoperative radioiodine treatment in papillary thyroid cancer (PTC). It is reported that BRAFV600E mutation was correlated with worse clinicopathologic features due to impaired NIS expression. In this study we evaluated the relationship of the BRAF mutation and functional NIS expression in patients with classical variant (CV) PTC.
Design: BRAF mutation was analyzed by RT-PCR in 106 consecutive cases withCV-PTC and immunohistochemical staining of NIS protein was evaluated in 96 cases. Localisation (intracellular or membraneous), intensity were characterized semiquantitatively. The density of cytoplasmic staining was also noted. Clinicopathologic features such as extrathyroidal invasion, lymph node metastesis were correlated with BRAF mutation and functional NIS expression. 88 patients who completed at least 24 months follow up were used for the outcome.
Results: Mean age was 46,2±13,7. Gender F/M: 79/17. 75/96 (78.1%) cases had BRAFmutation. Functional (membranous) NIS was higher in BRAF mutation positive group (78.7%) than in BRAF negative group (57.1%) (p=0.047). Nonfunctional (cytoplasmic) NIS was lower in BRAF mutation positive group (21.3%) than in BRAF negative group (42.9%) (p=0.047). Those with moderate and intense cytoplasmic staining had 6.43 times higher BRAF mutation (90%) than those with weak staining (58.3%) (95% CI=2.20-18.80,p=0.001). There was no association between NIS expresion patterns and lymph node positivity, extrathyroidal extension ans surgical margin positivity. Extrathroidal extension was present in 54.7% of cases with BRAF mutation and 33.3% without (p=0.084). Surgical margin positivity was present in 85.7% of cases with BRAF mutation and 14.3% without (p=0.084). There was no association for lymph node involvement (p=0,625). 7/88 patients without remission had BRAF mutation; 5 had functional NIS expression.
Conclusions: Functional NIS expression is higher among CV-PTC with BRAFmutation. But the clinical features were not found to be associated with NIS expression. There may be different mechanisms determining the outcome of therapy.
158 - Assessment of thyroid function and volume in hypogonadal patients - 2014
Uluslararası Bildiriler P- 1065, 16th European Congress of Endocrinology, 3 -7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
Background: Hypogonadism is related to additional endocrine abnormalities. Thyroid abnormalities may be common in hypogonadism patients, although this association is not clear.
Objective: In this study, we examined the incidence of thyroid disorders in hypogonadisms.
Methods: A case-control study of 68 hypogonadal patients and 74 age-matched healthy controls from the general population was conducted. Thyroid function, thyroid volume measurements, and presence of thyroid autoantibodies were examined.
Results: The mean BMI and age of the patient and control groups were similar (P=0.43 and P=0.407 respectively). The thyroid status differed significantly between the patient and control groups (P=0.002). In the patient group, 55 (80%) patients were euthyroid, 10 (14%) patients were hypothyroid, and 3 (6%) patients were hyperthyroid. In the control group, 71 (95%) subjects were euthyroid, and 1 (5%) was hypothyroid. Serum TSH levels were significantly higher in hypogonadal patients than in controls (P=0.018); however, serum free T4 and free T levels did not differ significantly between the two groups (P=0.29 and P=0.63 respectively). The presence of thyroid autoantibodies (anti-TPO and anti-TG) did not differ significantly between the patient and control groups (P=0.49 and P=0.89 respectively). There were no differences observed by ultrasonography between the patient and control groups. The thyroid volumes of the right and left lobes were measured. There were no significant differences in thyroid volumes of the patient and control groups (59.67±30.34 and 68.02±43.45 ml respectively;P=0.22).
Conclusion: A high incidence of hyperthyroidism and a high incidence of hypothyroidism were observed in hypogonadal patients.
157 - Comparison of aspiration vs with-out aspiration fine-needle biopsy of thyroid nodules for adequacy of cellularity according to Bethesda system - 2014
Uluslararası Bildiriler P-987, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Fine-needle aspiration (FNA) is a simple, minimalinvasive,cost-effective and widelyused diagnostic tool for evaluating thyroid nodules. Recent times a technique called fine-needle sampling non-aspiration (FNNA) or fine-needle capillary thyroid biopsies (FNC) has been more preferred. This technique prevents the use of suction so there is no aspiration crush and therefore nondiagnostic outcomes are reduced.The aim of this prospective study was to compare the FNA and FNNA with reference to diagnostic adequacy and diagnosisaccording to Bethesda System.
MATERİALS AND METHODS: Ultrasonography-guided FNA and FNNA biopsy were performed successively on 100 nodules. Both techniques were performedonthe same nodule and assessed by the same pathologist, beginning with the first (FNA) on half of the patients (randomly selected) and vice versa. The pathologist was unaware of the sampling method employed (FNA/FNNA) for any particular set of slides to avoid individual bias. The final cytopathologic finding was reported by using the Bethesda criteria, in which a sample is considered adequate if it contains a minimum of 6 groups of well observed follicular cells, with at least 10 cells per group.
RESULTS: During this study interval, FNA and FNNA were performed on 100 thyroid nodules of99 patients (78 patients were female,21 were male). The patients’ age range was 19-75 yearsold. The sizes of the thyroid nodules which biopsy samples were taken, areranged from 6 to 59 mm in mean diameter. A significant difference between FNA and FNNA examination was found ininadequate results (42% vs 22%, p=0.02).
There was no significant differences innodule features including;echogenicity, calcification and nodul size between the two techniques.
Table1: The cytopathologic results of FNA and FNNA sampling | |||
FNA | FNNA | p | |
Nondiagnostic | 42 | 22 | 0.02 |
Benign | 55 | 75 | |
Suspiciuos malignancy | 1 | 0 | |
Cytologic atypia or follicular lesion with undetermined significance | 2 | 2 | |
Malignant | 0 | 1 |
CONCLUSION: FNNA is an easier technique to perform with better patient compliance. We think our study will lead a further suggestion to prefer FNNA toreduce nondiagnostic results.
156 - Hyperthyroidism in a pregnant woman who had hypothroidism due to Hashimoto disease before - 2014
Uluslararası Bildiriler P-981, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Pregnant women with known hypothyroidism must have monthly follow up with thyroid function tests. Appropriate L-thyroxin replacement dose can be given due to trimester specific thyroid stimulating hormone (TSH) levels. We will discuss about a hyperthyroid pregnant woman who was taking L-thyroxin replacement before and during the first trimester of pregnancy for hypothyroidism.
CASE: A 24 year old woman admittedto our out-patient clinic for fatigue and weight gain. She had a family history of Hashimoto thyroiditis. Her TSH was 10.13 uIU/mL (0.27-4.2), free T4 was 1.27 ng/dL (0.9-1.7), free T3 2.98 pg/mL (1.8-4.6), anti thyroid peroxidase antibody (TPO Ab) was 11.8 IU/mL (0-34) and anti thyroglobulin was 17.27 IU/mL (0-115). Her thyroid ultrasonography was compatible with chronic thyroiditis. L-thyroxin replacement was started after Hashimoto disease diagnosis. After euthyroidisim achieved she became pregnant. With monthly follow up L-thyroxine dose adjusted. On the 20th week of pregnancy thyroid function tests revealed thyrotoxicosis. Despite cessation of L-thyroxin treatment thyrotoxicosis persists and when we take the titer of thyrotropin receptor stimulating antibody (TSHR Ab) it was 405 u/L (0-14). There was no ophtalmopathy on physical examination. Propylthiouracil treatment was started. And she had a healthy boy baby with no obvious thyroid dysfunction.
Table. Thyroid hormone levels of patients
TSH | fT4 | fT3 | |
Prepregnancy | 10,13 | 1,27 | 2,98 |
11 th week (while taking L-thyroxin) | 3,13 | 1,46 | 2,89 |
20 th week (L -thyroxin stopped) | 0,02 | 1,89 | 6,23 |
26 th week (PTU started) | 0,006 | 3,24 | 12,13 |
CONCLUSION: TSHR Ab is responsible for two distinct clinical syndromes. Stimulating antibodies (TSAb) cause thyrotoxicosis when blocking antibodies(TBAb) cause hypothyroidism. Antibody switch can occur during some periods one of which is pregnancy. The etiology of this process remains unknown but hemodilution of TBAb titer can be one of the possible mechanisms. This is at least one of the important issues that close follow up is mandatory during pregnancy.
155 - An ectopic thyroid tissue presenting as anterior mediastinal mass in a breast cancer patient - 2014
Uluslararası Bildiriler P-980, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Ectopic thyroid tissue is the result of abnormal gland migration from the foramen caecum to its normal pretracheal position. An ectopic thyroid can be lingual (at the base of the tongue), sublingual (below the tongue), prelaryngeal (in front of the larynx), or can be found at other rare sites. The most frequent noncervical location for ectopic thyroid tissue is the thoracic cavity. Here we discuss about a rare case of mediastinal ectopic thyroid tissue presenting with a superior mediastinal mass compressing the brachiocephalic truncus without any symptom in a patient with breast cancer.
CASE: An 61-year-old nonsmoker female patient with an incidental finding of a mediastinal mass on Thorax computerized tomography (CT)scan for following up of breast cancer had consultated us from medical oncology department. Her previous medical history included chronic obstructive pulmonary disease, hypertension, type 2 diabetes mellitus. She had two operation for breast cancer and multinodular goiter before.Thyroid stimulating hormone (TSH), free thyroxine (fT4) and the titers of serum thyroid auto-antibodies were within the normal range.She had history of chest radiation and chemotherapy because of breast cancer.
Her thyroid was not palpable, and there was no evidence of cervical lymphadenopathy.An ultrasound of the remnant thyroid identified only two solid nodules. A CT scan of the thorax revealed a 4.7x3.0cm heterogeneously enhanced mass in the superior mediasten. The mass was located at the intersection of the caudal margin of the left brachiocephalic vein and assendan aorta, and it compressed the brachiocephalic truncus. However, there were no symptoms related to the compression. Tc-99m pertechnetate thyroid and mediastinal scintigraphy revealed a mass which was 4 cm and increased uptake in superior mediasten (Ectopic thyroid or metastatic lesion?). As it can the mediastinal metastasis of the breast cancer that can uptake technesium, total body scanning with I-131 revealed which showed increase uptake of iodide in the superior mediastinal mass with 4.5x4.0x5.5 cm dimensions. The mass was resected totally. Histopathological examination revealed nodular colloidal goiter.
Picture. Radioiodine anterior and posterior whole body images
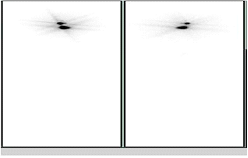
CONCLUSION: Ectopic thyroid is a rare condition, and its location in the mediastinum is even rarer. Although entirely intrathoracic ectopic thyroids are rare, they must be considered in the differential diagnosis of all mediastinal masses. Thoracotomy or sternotomy is required for resection of the mass and prognosis is excellent following a successful excision.
154 - Lanreotide-induced bradycardia and supraventricular extrasystoles - 2014
Uluslararası Bildiriler P-916, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
CASE: A 63-years-old acromegalic woman admitted to our hospital for lassitude and dizziness. She has been diagnosed acromegaly ten years ago and had two transsphenoidal operations. Since remission has not achieved she started to use Lanreotide (somatostatin analogue) and for seven years she has been treated with it. Laboratory examinationrevealed that, basal plasma growth hormone (GH) level 1.21 ng/mL (normal range:0-5); nadir GH level after glucose tolerance test1.2 ng/mL (normal range: less than 1); Insulin-like growth factor-1 (IGF-1), 129.1 ng/mL (normal range: for age: 75-212); thyroid stimulating hormone (TSH), 0.824 uIU /mL (normal range: 0.27-4.2); free thyroxine (fT4), 1.26 ng/dL (normal range: 0.9-1.7); and prolactin, 6.66 ng/mL (normal rangein women: 0-20). Magnetic resonance imagining (MRI) of pituitary glandwith gadolinium contrast revealed a pituitary microadenoma. Since routine resting electrocardiograms of patient showed bradycardia (46 bpm) and supraventicular extrasystoles, lanreotide treatment stopped. After then patient’s symptoms relieved and heart rate increased (64 bpm).
Picture 1.ECG of patient using lanreotide Picture 2. ECG of patient after lanreotide
cessation

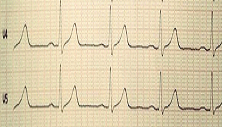
CONCLUSION: Somatostatin is a peptide hormone with a short half-life (2-3 min), which is synthesized in multiple tissues, including the hypothalamus, to inhibit GH secretion. Somatostatin analogues (Octreotide and Lanreotide) are indicated principally for the treatment of acromegaly that remains active after transsphenoidal surgery, whether or not the patient has also undergone radiotherapy. Octreotide-induced bradycardia has previously been reported as an unusual finding in different clinical situations (nonacromegalic patients) and a male patient with acromegaly.A rat study shows bilateral microinjection into the rostral ventrolateral medulla of either somatostatin or the receptor-selective agonist lanreotide evoked dramatic, dose-dependent sympathoinhibition, hypotension, and bradycardia. Our case is the first reported patient with acromegaly who had bradycardia and supraventricular extrasystoles associated with use of Lanreotide.
153 - High dose hook effect’ in a patient with invasive giant prolactinoma - 2014
Uluslararası Bildiriler P-894, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: Prolactin secreting pituitary adenomas (prolactinomas) arethe most common pituitary adenomas. The magnitude of prolactin(PRL)secretion in prolactinomas is usually proportionate to the tumor’s size. Invasive giant prolactinoma is a large prolactinoma(>4 cm in dimension) presenting with serum prolactin levels of >1000 ng/mL and mass related clinical symptoms. Giant prolactinoma is rare and usually presents in men.
CASE: A52-year-old man was admitted to our hospital with headache, decreased libido, blurred vision and diplopia existing for 6 months. Magnetic resonance imaging (MRI)showed a giant pituitary adenoma (47x35x33 mm) with extension to sylvian, suprasellar cisterns, invading to right cavernous sinus and extension from right of third ventricle to the superior, wrapping the right internal carotid and middle cerebral arteries. The hormon levels at admission showed follicle stimulating hormone (FSH), 4.48 mIU/mL (normal range;1.5-12.4); luteinizing hormone (LH), 3.75 mIU/mL (normal range;1.7-8.6); testosterone 0.736 ng/mL (normal range; 2.84-8), thyroid stimulating hormone (TSH),0.959 uIU/mL (normal range;0.27-4.2); free thyroxin index 1.28 ng/dL (normal range;0.9-1.7) and prolactin, 470 ng/mL (normal range;0-15 ). Because of apoplexy, patient was promptly operated. Postoperative prolactin level was 470 ng/mL as before. Then prolactin assay was repeated in 1 in 100 dilution of the serum, which was reported as 2060 ng/mL.
CONCLUSION: The intensity of an antigen-antibody interaction depends primarily on the relative proportion of the antigen and the antibody. A relative excess of either will impair adequate immune complex formation. This is called the ‘high dose hook effect’. The high dose hook effect often interferes with the assay result. To overcome the hook effect, the serum sample is diluted and then prolactin assayed. In our patient, a 1:100 dilution gets accurate values. We suggest that in order to accurately estimate PRL in patients with large pituitary tumors, PRL should be assayed in 1:100 or even higher dilutions of serum in order to gate an accurate estimate of serum PRL.
Picture 1. Pituitary MRI of the patient in coronal plane
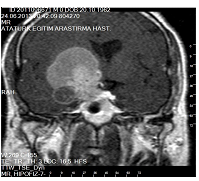
152 - A case with macroprolactinemia and gigantomastia responding to cabergoline treatment - 2014
Uluslararası Bildiriler P-878, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
Macroprolactinemia is reportedly 10-25% in patients with hyperprolactinemia (1). This condition corresponds to the predominance of higher molecular mass prolactin (PRL) forms (big-big PRL, MW > 150 kDa), that have been postulated to represent PRL monomer complexed with anti-PRL immunoglobulins or autoantibodies (2). PRL plays a major role in breast development. Factors which lead to the elevation of serum PRL such as pregnancy and administration of dopamine antagonists also lead to breast growth (3). Macromastia, gigantomastia, breast hypertrophy are used interchangeably. Patients present with typical physical, social and psychological problems associated with macromastia. They present with symptoms related to muscular discomfort such as shoulder, back, neck and breast pain as well as postural problem mainly kyphoscoliosis because of the weight of the breasts. Hygienic problem in the submammary crease leading to irritation and rashes and sometimes ulceration can be presenting symptoms (4). Its treatment include surgery, hormonal treatment or both. Most authors conclude that gigantomastia cannot be treated medically and only resolves with surgical manoeuvres (5). We report a case with gigantomastia diagnosed with macroprolactinemia and treated with cabergolin.
Case: A 44-year-old woman admitted to our clinic with 6 months history of breast enlargement, nipple discharge, mastalgia, and back pain. She requested surgical reduction. She had three children and her menstrual cycles were regular. There were no history of excessive weight gain, chronic disease or use of any drug. No known family history of mammary hypertrophy. Her body mass index was 31,2 kg/m2 . The breasts are firm to palpation and diffusely tender. The superficial veins are prominent and dilated. She had no fever, erythema, ulceration of the breast skin. Breast circumference was 116 cm. Galactorrhea was present. Hormonal assay revealed hyperprolactinemia (PRL:87 ng/mL) and macroprolactinemia. Other anterior pituitary hormons levels were in normal range. Hook effect was not detected in the diluted serum sample. MRI showed 6 mm pituitary adenoma. Breast ultrasound and mammography were normal. Cabergoline 0.5 mg per week was started. Macroprolactinemia and hyperprolactinemia were normalized within one month. Breast circumferences were 110, 108 and 106 cm in first, second and third mounths, respectively, although galactorrhea continued. Cabergoline dose was increased to 1 mg per week. Patient was satisfied with postmedical recovery and gave up operation demand.
Conclusion: The clinical significance of macroprolactinemia has been a matter of debate for many years. Some reports have associated it hyperprolactinemic symptoms whereas others have suggested that it causes no symptoms. This controversy could be explained by heterogeneity of macroprolactin structure. In the majority of cases, the high molecular form consists of complexes of PRL and anti-PRL autoantibodies predominantly of IgG , rarely IgA and IgM class (7). Macroprolactin synthesis is generally thought to be an extrapituitary postsecretory phenomenon. On the other hand, pituitary adenomas are revealed in 20% with macroprolactinemia. Additionally, galactorrhea is present in 20% and oligo/amenorrhea in 45% (6). Two explanations are possible in our case: coexistence of pituitary adenoma and macroprolactinemia or macroprolactin production by pituitary tumor itself. Literature data have provided evidence in favor of both possibilities. Leslie et al. have shown the monomeric PRL isoform in tissue samples from pituitary adenomas in patients with macroprolactinemia, This result may support the hypothesis of peripheral mechanism of macroprolactin synthesis (8). In contrast, two studies have demonstrated significantly higher concentrations of macroprolactin in extracts from prolactinoma tissue compared to those in samples from normal adenohypophysis (9, 10). Coexistence of pituitary nonfunctioning adenoma and macroprolactinemia could be suggested in patients with oligosymptomatic clinical presentation. One case report has been published in support of the thesis for the tumoral origin of macroprolactinemia. Lakatos et al. presented the history of a 80-year-old man with an intra and parasellar pituitary tumor and marked hyperprolactinemia mainly due to macroprolactinemia (11). Consequently, cabergolin treatment seems to be safe and effective in controlling gigantomastia and macroprolactinemia without surgical intervention. Although macroprolactinemia is considered to be a benign condition, pituitary imaging, dopamine agonist treatment, and prolonged follow-up should be recommended in some cases (7).
References:
1. Shimatsu A, Hattori N. Macroprolactinemia: Diagnostic, Clinical, and Pathogenic Significance. Clin Dev Immunol. 2012:167132. doi: 10.1155/2012/167132. Epub 2012 Dec 4.
2. Kasum M, Oreskovic S, Zec I, Jezek D, Tomic V, Gall V, Adzic G. Macroprolactinemia: new insights in hyperprolactinemia. Biochem Med. 2012;22(2):171-9.
3. Stringer BM, Rowson J, Williams ED. Effect of raised serum prolactin on breast development. J Anat. 1989; 162: 249-261.
4. Rahman GA, Adigun IA, Yusuf IF. Macromastia: a review of presentation and management. Niger Postgrad Med J. 2010;17(1):45-49.
5. Dancey A, Khan M, Dawson J, Peart F. Gigantomastia--a classification and review of the literature. J Plast Reconstr Aesthet Surg. 2008;61(5):493-502.
6. Melmed S, Casanueva FF, Hoffman AR, Kleinberg DL, Montori VM, Schlechte JA, Wass JA; Endocrine Society. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. JCEM. 2011;96(2):273-288.
7. Elenkova A, Abadzhieva Z, Genov N, Vasilev V, Kirilov G, Zacharieva S. Macroprolactinemia in a patient with invasive macroprolactinoma: A case report and minireview. Case Rep Endocrinol. 2013;2013:634349. doi: 10.1155/2013/634349. Epub 2013 Jan 15.
8. Leslie H, Courtney CH, Bell PM. Laboratory and clinical experience in 55 patients with macroprolactinemia identified by a simple polyethylene glycol precipitation method JCEM. 2001;86(6): 2743-2746.
9. Mounier C, Trouillas J, Claustrat B, Duthel R, Estour B. Macroprolactinaemia associated with prolactin adenoma. Hum Reproduction. 2003;18(4):853-857.
10. Ohnami S,Eto S, Ohnami S. Characterization of ‘bigbig prolactin’ in serum and tumor extract in patients with PRL-secreting tumor. Endocrinol Jap 1987;34(3):325-334.
11. Lakatos G, Szücs N, Kender Z, Czirjak S, RAcz K. Macroprolactinemia associated with pituitary macroadenoma: treatment with quinagolide. Orv Hetil. 2010 Jun 27;151(26):1072-5.
151 - Thyroid disorders in young females with polycystic ovary syndrome: is thyroid volume associated with serum IGF1 level? - 2014
Uluslararası Bildiriler P-635, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: Polycystic ovary syndrome (PCOS) is one of the most common disorders affecting at least 5 to 10% of women of reproductive age. Increased prevalance of autoimmune thyroiditis and goiter were reported in PCOS patients. This study investigated the prevalance of hypothyroidism, thyroid autoimmunity, ultrasonographic features and presence of nodules in PCOS patients and compare them with the control group. We also aimed to detect correlation of thyroid volume (TV) with serum ınsulin-like growth factor-1 (IGF-1) and the other hormon levels in patients with PCOS.
MATERIALS AND METHODS: Seventy PCOS patients and 84 age matched controls were enrolled in this study. Patient group and the control group were compared with each other according to hormonal parameters, anthropometric measures, thyroid volume, echogenicity on ultrasonography (USG) and autoimmunity. We also investigated the correlation between TV and IGF-1 levels in the PCOS group.
RESULTS: Body mass index (BMI), Ferriman Gallwey score (FGS), fasting insulin level, dehydroepiandrosterone-sulfate (DHEA-S), total and free testosterone, luteinizing hormone (LH), thyroid volume and insulin like growth factor binding protein-3 (IGFBP-3) levels were significantly higher in PCOS patients compared to the control group. Thyroid volume was similar in patients with or without insulin resistance diagnosed with HOMA-IR. There was no differences according to prevalence of hypothyroidism or ultrasonographic features, in between the groups. We have detected a positive and significant correlation between TV and BMI.
CONCLUSION: As a conclusion, we found that thyroid autoimmunity and nodularity were similar between PCOSand control subjects whereas TV was more in the PCOS group. Two parameters that were foundto be positively associated with TV were BMI and serum LH level. Oral cantraceptives which are the mainstay of PCOS treatment can reduce LH and decrease TV and the number of patientswith goiter. There is need for further studies measuring pre and post therapy thyroid volume andits association with serum LH measurements in PCOS patients receving oral contraceptives inorder to prove aforementioned hypothesis
Table 1. Correlation of different hormonal and antropometric parameters with thyroid volume
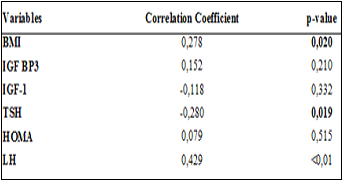
Table 2.Comparison of the groups according to ultrasonographic findings
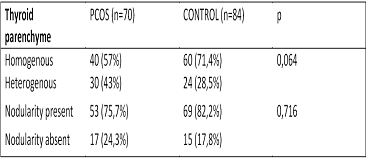
150 - Prolonged Cerebellar Ataxia after - severe hypoglycemic attack in a patient with T1DM: A rare but disturbing sequela - 2014
Uluslararası Bildiriler P-447, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: Hypoglycemia is common in people with diabetes who aim to achieve strict blood glucose control. The neurologic manifestations of hypoglycemia are mostly reversible and includes behavioral changes, difficulty in concentration, confusion, loss of fine motor functions and seizures. Herein we have presented a case who was pregnant and experienced severe hypoglycemia which led to permanent ataxia.
CASE: 26 years old female patient was brought to our emergency room by her husband because of being found unconscious. She was 10 weeks of pregnant and had history of type 1 diabetes mellitus (T1DM) for 13 years. At the time of admission her plasma glucose level was 23 mg/dl. Intravenous glucose infusion and glucagon were applied rapidly. In the initial physical examination she was lethargic, blood pressure was low with tachycardia while body temprature was normal.In the obstetric ultrasonography (USG), the fetus was alive. She had nonproliferative retinopathy in the eye examination and sensory neuropathy. In the labaratory examination, she had microalbuminuria and normal kidney and liver function tests, electrolytes, thyroid function tests and vit B12 levels. After her blood glucose returned to normal, complete neurologic examination was made. Her pupils were reactive, tendon reflexes were normal but she was dysarthric. On the second day, dysarthria continued. We realized she had gait disturbace and on cordination tests she had severe dysmetria in all 4 limbs (finger to nose and heel to shin). Cranial magnetic resonance imaging (MRI) and electroencephalography (EEG) didn’t reveal any pathology. With short acting anologue and NPH insulin, her blood glucose levels were within the target range but her dysartria and ataxia persisted upon discharge on the 12 th day. One month after discharge, she still had moderate gait disturbance and slow speech in the pregnancy and the newborn control visit.She had an uneventful labor on the 39 th week of was healthy.
CONCLUSION: The neurologic manifestations of hypoglycemia include behavioralchange, confusion, loss of consciousness, and seizures.Rarely, neuroglycopenia can present as ataxia, and prolongedand potentially irreversible deficits may occur with repeatedepisodes of hypoglycemia. Cerebellar dysfunction is a rare complication of hypoglycemia and may occur in patients with altered cerebellar glucose kinetics.In summary, glucose uptake and utilization in the cerebellumappear to be protective with regard to hypoglycemia.Hence, cerebellar dysfunction is a rare complication ofhypoglycemia, this disorder may occur in patients with alteredcerebellar glucose kinetics. It appears that the neuronal damage in our patient was severe enough to causeprolonged ataxia.Differential diagnosis involves hematoma, cerebellitis, drug or alcohol ingestion, Wernicke encephalopathy, vit B12 deficency and ataxia telengiectasia. Reconsideration of therapy and glycemic targets and supportive therapy is warrented.
Table 1. Labaratory data of the patient
Laboratory result | Normal range | |
Plasma Glucose | 40 mg/dl | 70-199 |
Urea | 35 mg/dl | 10-48 |
Creatine | 0.8 mg/dl | 0.1-1.2 |
Na | 142 mg/dl | 136-145 |
K | 3.8 mmol/l | 3.5-5 |
ALT | 29 U/L | 0-41 |
insulin | 1.54 µU/ml | 2.6-24.9 |
C- peptide | 0.3 ng/ml | 0,1-3.6 |
Anti -GAD | 14 u/ml | 0-1 |
Anti-islet | positive | negative |
TSH | 2.5 uIU/ml | 0.4-4.5 |
Anti-TPO | 149 IU/ml | 0-34 |
Cortisol | 30 µg/dl | 6-19 |
149 - Markers of endothelial dysfunction in type1 diabetics with or without microalbuminuria - 2014
Uluslararası Bildiriler P-436, 16th European Congress of Endocrinology, 3 -7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: Diabetic nephropathy (DN) is one of the important complications and is detected in almost 30-40% of the patients with type 1 diabetes mellitus (T1DM). Besides the well known risk factors, endothelial dysfunction also plays a role in the pathogenesis of DN and diabetic retinopathy. Our aim was to determine flow medaited dilation (FMD) measurements and serum soluable endothelin-1 (ET-1), intercellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1) levels in type 1 diabetic patients with or without inceased albumin excretion and compare them with the control group.
MATERIALS AND METHODS: We enrolled 73 patients with T1DM. Diabetic patients were divided into two subgroups according to microalbumin measurements in 24 hour urine collections. Patients with microalbuminuria formed Group 1 and without microalbuminuria were defined as Group 2. We have also enrolled 40 subjets with similar sex and age distrubution as control group (Group 3). Serum ET-1, ICAM-1 and VCAM -1 levels were determined and FMD measurements were done in all individuals.
RESULTS: Mean age, sex distrubition, presence of hypertension, serum low density lipoprotein (LDL) and triglyceride levels were similar in all groups. Diabetic groups were similar in regard to glycemic control and disease duration. Mean FMD measurement was lower in diabetic groups compared to the control group. FMD was negatively correlated with age. We didn’t detect any difference between groups according to serum ET-1 levels. Median serum ICAM-1 level was higher in diabetic groups compared to the control group. Median serum VCAM-1 level was higher in the group of patients with microalbuimuria compared to the normoalbuinuric and control groups. Serum VCAM-1 level was found to be posively correlated with degree of urinary albumin excretion (p>0.001).
CONCLUSION: ICAM-1 and VCAM-1 are proinflammatory molecules that play an important role in pathogenesis of endothelial dysfunction. Medical agents that reduce the serum levels of those two molecules would take place in prevention of microvascular complications. Moreover, VCAM1 may be used as a predictive marker for risk stratification of nephropathy development and progression in T1DM.
Table 1. Comparision of groups according to ICAM-1,VCAM-1 and endothelin-1 levels
Groups | Endothelin-1 Median (minimum-maximum) (fmol/l) | ICAM-1 Median (minimum-maximum) (ng/ml) | VCAM-1 Median (minimum-maximum) (ng/ml) |
Group 1 | 8.1 (0.6-16.5) | 5100 (1450-12860)a | 736.5 (419.9-1516.7)c |
Group 2 | 7.7 (3.1-23.5) | 4520 (326.1-11070)b | 975.9 (352.2-1525.5)b,c |
Group 3 | 10.5 (3.0-19.0) | 685.7 (120-14460)a,b | 680.1 (380.0-1041.9)b |
p-value | 0.066 | <0.001 | 0.002 |
Table 2. FMD measurements of the groups
Groups | FMD (%) |
Group 1 | 6.6 (3.1-10.3)a |
Group 2 | 6.4 (4.3-11.1)b |
Group 3 | 7.8 (3.1-12.0)a,b |
p-value | 0.013 |
148 - Hemostatic biomarkers in selected group of patients with type 1 diabetes: Are they associated with different degrees of diabetic retinopathy - 2014
Uluslararası Bildiriler P- 435, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: Diabetic retinopathy (DR) is the leading cause of blindness in the world. Retinopathy and nephropathy can still progress in diabetics despite optimal metabolic control. This suggests that factors other than hyperglycemia, such as abnormal hemostatic parameters, may play a role in the disease pathogenesis. Based on this hypothesis, several markers of hypercoagulation including fibrinogen, plasma activator inhibitor (PAI), and alpha-2-anti plasmin have been identified. The aim of the present study was to determine whether different degrees of DR (proliferative or non-proliferative) were associated with abnormally modulated hemostatic parameters in patients with type 1 diabetes mellitus (DM).
MATERIALS AND METHODS: 52 type 1 diabetic patients and 40 healthy controls were enrolled in the study. Patients were then subdivided into three categories. Group I was defined as those without retinopathy, group II with non-proliferative retinopathy (NPRP), and group III with proliferative retinopathy (PRP). We have compared these subgroups with each other and the control group (group IV) according to the serum fibrinogen, plasminogen, α2-anti-plasmin, and PAI.
RESULTS: We detected that PAI-1 levels were higher in the diabetic groups than control, but this was not statistically significant whereas serum fibrinogen (p=0.224) and plasminogen (p=0.224) were similar between the diabetic and control groups. Alpha-2-anti-plasmin in groups I, II, and III was higher compared to the control group (p<0.01, p<0.05, and p<0.001, respectively) and the positive correlation identified between serum α2-anti-plasmin and HbA1c levels (r=0.268, p=0.031).
Table. Biochemical and hemostatic measurements ofdiabetic patients and healthy controls
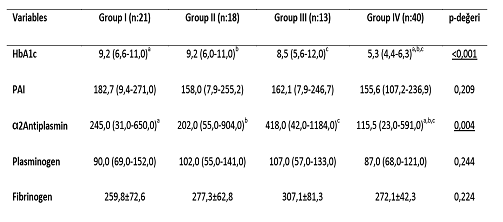
a:Difference between Grup I and Grup IV is significant (p<0,01), b: Difference between Grup II and Grup IV is significant (p<0,05), c: Difference between Grup II and Grup IV is significant (p<0,001).
Figure. Expression of α2-antiplasmin in the diabetic and control groups
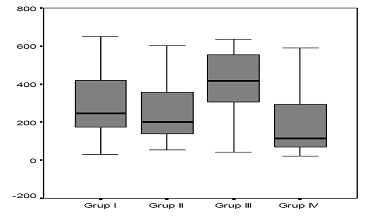
CONCLUSION: To our knowledge there are only a small number of studies measuring α2- antiplasmin levels in type 1 diabetes. A positive correlation between α2 anti-plasmin with HbA1c suggests that fibrinolytic markers may improve with disease regulation, and better glycemic control. High α2-anti-plasmin level might be a novel risk factor for development of DR. Confirmation of these data would allow a better understanding of the pathogenesis of DR.
147 - Relationship between diabetes mellitus and hemostasis: a prothrombotic condition - 2014
Uluslararası Bildiriler P-421, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
Background: Diabetes is very common disorder. Many studies have shown that patients with diabetes mellitus have incresing trombotic complications both arterial and venous trombosis. Bad control diabetes increases risk of trombosis. Recent reports have shown that shortened APTTs and increased fibrinogen indicate procoagulan situations. In this study, we aimed to evaluate whether chronic hyperglisemia or bad control diabetes causes trombosis which is reflected by shortened APTTs and increased fibrinogen.
Materials and methods: Our study included 349 patients with type 2 diabetes mellitus. They all underwent blood sampling APTT, PT, fibrinogen, fasting plasma glucose (FPG), postprandial plasma glucose (PPG), complete blood count(CBC), serum lipids and HBA1C measurements. Among 349 patients whose APTT<22 sec and PT<10.5 sec were determined. Patients were divided into two groups based on HBA1C levels as follows: regulated diabetic group (HBA1C<7.0%) and disregulated diabetic group (HBA1>7.0%).
Results: But there was no significant difference in terms of APTT<22 sec, PT<10.5 sec and fibrinogen levels between two groups.
Conclusion: APTT, PT and fibrinogen measurements are relatively inexpensive and are available. But they are not enough alone for evaluating hypercoaguable states in diabetes patients.
146 - New onset T1DM after vaccination for measles: coincidence or consequence? - 2014
Uluslararası Bildiriler P-374, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: Type 1 diabetes mellitus(T1DM)is one of the most common metabolic diseases in childhood: Epidemiological data, collected by worldwide population-based registries, shows an increasing incidence of diabetes over the past 20 years, turning the illness into the most frequent chronic disorder. It is hypothesized that genetic and environmental factors (either of toxic or viral origin) may contribute to diabetes susceptibility.The adaptive immune response genes (HLA) still provide the major contribution to the onset of Type 1 diabetes, but understanding how viral or bacterial infections, vaccines or dietary components or simply stress determine an autoimmune reaction in certain individuals is still a matter of interest. The occurrence and significance of autoimmune manifestations after the administration of viral vaccines remain controversial. Herein we have represented a case who developed type 1 diabetes one month after vaccination for measles in military.
CASE: 25-years-old male patient admitted to our clinic with the complaints of polyuria, poydipsia and weight loss. When we questioned his personal history, we have learnt that he had measles vaccination in the army, one month ago. In the initial labaratory examinations, plasma glucose was 400 mg/dl, dipstick urine test was ++++ ketone and there was metabolic acidosis with anion gap. After treatment of diabetic ketoacidosis, we skipped to intensive insulin treatment with short and long acting anologue insulins. Since he had very low c peptide level together with positive anti glutamic acid decarboxylase (Anti GAD) and Anti-islet antibodies, he was diagnosed to have T1DM. His anti thyroid peroxidase antibody (Anti TPO) was positive and had thyroiditis on thyroid ultrasonography. We have screened other components of autoimmune syndrome and found that celiac markers and Antiparietal antibodies were negative. He had adequate cortisol response to short cosyntrophin test. He was discharged after regulation of blood glucose levels.
CONCLUSION: Very few patients may develop some autoimmune diseases following viral vaccination (in particular; arthropathy, vasculitis, neurological dysfunction and thrombocytopenia). To date, there are controversial results concerning the implication of viruses in human β-cell autoimmunity. Further investigations based upon the temporal relationship between viral diseases and onset of Type 1 diabetes might help to design more accurate national and international prevention strategies. For the majority of people, vaccines are safe and no evidence linking viral vaccines with type 1 diabetes, multiple sclerosis (MS) or inflammatory bowel disease can be found. However there are rare cases in the literature reporting new onset autoimmune diabetes after vaccination. Therefore, it might be reasonable to screen patients who are prone to diabetes for the signs and symptoms of diabetes after vaccination.
Table. Labaratory data of the patient
Lab | Normal range | |
Plasma Glucose | 400mg/dl | 70-199 |
Urea | 28 mg/dl | 10-48 |
Creatine | 1 mg/dl | 0.1-1.2 |
Na | 127 mg/dl | 136-145 |
K | 4.2 mmol/l | 3.5-5 |
ALT | 29 U/L | 0-41 |
insulin | 4.54 µU/ml | 2.6-24.9 |
C- peptide | 0.2 ng/ml | 0,1-3.6 |
Anti -GAD | 50.15 u/ml | 0-1 |
Anti-islet | positive | negative |
Urine keton | +++ | 0 |
Art. Ph: | 7.28 | 3.35-7.45 |
HCO3 | 12 mmol/l | 15-25 |
TSH | 3 uIU/ml | 0.4-4.5 |
Anti-TPO | 240 IU/ml | 0-34 |
Cortisol | 5 µg/dl | 6-19 |
145 - Follicular thyroid carcinoma presenting with occipital bone and lung metastasis - 2014
Uluslararası Bildiriler P-305, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: When follicular thyroid carcinoma(FTC) is diagnosed, extrathyroidal invasion, lymphatic and distant metastasis have been determined in 25%, 5-10% and 10-20% of the patientsrespectively.The most common site of distant metastases of FTC is the lung, followed by the bone. The incidence of skull metastasis of FTC is about 2.5 to 5.8%. Skull metastasis of FTC islocated in the skull base and occipital area.
CASE: 60-years-old man was operated for total thyroidectomy in1998and histopathology of the surgical specimen was reported as follicular carcinoma of thyroid with features of vascular invasion. 150 mCi of radioactive iodine (RAI) treatmentwas givenafter the surgery. Post RAI I-131whole-body scanning(I-131-WBS) was normal.When the patient admitted to our centerin 2006, I-131-WBS was performedand revealed occipital bone and lung metastasis.
The patient was operated and occipital bone removed. Histopathology of the surgical specimen was reported as FTC metastasis. After then 200 mCi additional radioiodine dose was given. In 2008, 250 mCi additional radioiodine dose was given for recurrence.I-131-WBS revealed occipital bone and multiple defined mass, which were metastasis in both lungs in September 2012.Alsocranial magnetic resonance imaging (MRI)revealed 24x24x22 mm mass in occipital zone. He underwent F-18-FDG PET/CT scan for investigating distant metastasis. On PET scan, an increased of F-18-FDG (SUVmax: 24.1) uptake was seen in 23 mm mass which had destructed occipital bone. Also, increased FDG uptake (SUVmax: 10.8) in 26 mm masson the upper lobe ofthe right lung and in 34 mm mass on the middle lobe medial ofthe right lung(SUVmax: 2.4) was determined. There were multiple parenchymal lesions, which were in different diameters and in different metabolic activities in both lungs. The patient was given 275 mCi additional radioiodinetherapy
Picture 1.Torax CT of the patient

Picture 2.Brain CT of the patient

CONCLUSION: This is a rare case of follicular thyroid carcinoma metastasis tooccipital bone. The treatment choice of FTC is total thyroidectomy with radioiodine administration, and surgical procedure for metastatic lesionsand TSH suppressive therapy
144 - The coexistence of anaplastic thyroid carcinoma and papillary thyroid carcinoma: two case reports - 2014
Uluslararası Bildiriler P-285, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Anaplastic thyroid carcinomas (ATCs) are sometimes accompanied by well-differentiated carcinomas (WDCs), and have been speculated to be dedifferentiated from the preexisting or coexisting WDCs. We will present two cases determined with both ATC and papillary thyroid carcinoma (PTC).
CASE-1: A 82-year-old woman was investigated due to a painful neck mass. The case reported no complaints of dysphagia or dysphonia. Thyroid function tests were within normal ranges. Thyroid ultrasonography revealed isohypoechoic nodules in sizes of 19x21.2x45 mm and 6.2x11.4x13.5 mm in right lobe and a isoechoic nodule in size of 7.8x8x11.3 mm in left lobe. Fine needle aspiration biopsy was performed, and PTC was detected in both nodules on the right.Bilateral total thyroidectomy was performed, and during the operation it was observed that a tumor was invaded trachea and eusophagus. In pathological investigation, the nodule of 45 mm in the right lobe was seen to be an ATC including regions of classical variant PTC (Figure 1). Anaplastic carcinoma regions were largely with epithelioid appearance and also included squamous differentiation regions. Marked pleomorphism and frequent mitosis were determined in the tumor including widespread necrotic regions. Immunohistochemical examination revealed that pancytokeratin was positive, HBME 1 was focal positive, but TTF-1 was negative. Proliferation index of Ki-67 was 70%. Additionally, the pathology of the nodule of 13.5 mm in the right lobe was consistent with classical variant PTC (Figure 2). ATC and PTC were present in the case in the form of two different foci. PET/CT revealed the involvements of increased 18 FDG consistent with metastasis, and due to the metastatic condition in the case, radiotherapy was performed.
CASE-2: A 62-year-old male presented to our clinic complaining of a neck lump, hoarseness, and dysphagia. Physical examination revealed a 4-cm mass and cervical lymph nodes on the left side of the neck. Thyroid function tests were within normal ranges. Thyroid ultrasonography revealed hypoechoic nodules in sizes of 41 mm nodule in the left lobe. Two preoperative fine-needle aspiration biopsies were reported as non-diagnostic. He underwent a bilateral total thyroidectomy and left extended lymph node dissection. The final postoperative pathology report was a 3-cm ATC in the left lobe and a 5-mm PTC in the right lobe (Figure 3). He was given external beam radiation therapy postoperatively.
Figure 1. Microscopic photograph of anaplastic thyroid carcinoma, HE x200(Case 1)
Figure 2. Microscopic photograph of papillary thyroid carcinoma, HE x200 (Case 1)
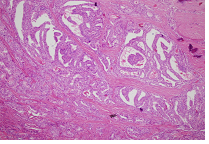
Figure 3. A: Anaplastic thyroid carcinoma, B: Papillary thyroid carcinoma, HE x200 (Case 2)
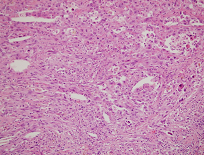
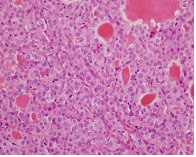
A. B.
CONCLUSION: PTC followed by poorly differentiated and follicular carcinoma are most frequently cited to coexist or as precursors of ATC. The early diagnosis of thyroid carcinoma results in decrease of the incidence of ATC.
143 - Three endocrine neoplasms: an unusual combination of pituitary adenoma, papillary thyroid carcinoma, and follicular thyroid carcinoma - 2014
Uluslararası Bildiriler P-279, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: Differentiated thyroid cancer is the most frequent thyroid tumor. Combinations of follicular and papillary carcinoma can be seen. Functional pituitary adenoma coexisting with differentiated thyroid carcinoma was reported previously in literature. We report a 47-year-old women with three different synchronous endocrine tumors; papillary thyroid cancer, follicular thyroid cancer and prolactinoma.
CASE: 47-years-old female patient was admitted to out-patient clinic with oligomenorrhea and galactorrhea. Except patient’s prolactin (PRL) rise, hormonal levels were in normal ranges (PRL: 186 ng/ml). Macroprolactin was negative. Pituitary magnetic resonance imaging (MRI) demonstrated a mass with 9x11 mm size (Image). Cabergolin 0.5 mg/ twice a week was started. She was euthyroid and thyroid autoantibodies were in normal ranges. In thyroid ultrasonography (US), 17x10 mm nodule in left lobule, 21x19 mm nodule in right lobule and 8x7mm nodule in isthmus were detected. Fine needle aspiration biopsy suggested suspicious for follicular neoplasm for nodule in right lobule, benign for the left one. She underwent total thyroidectomy. The histopathological examination revealed presence of a follicular cancer within right lobule (2 cm) and multifocal papillary cancer (0.5 cm, 0.8 cm, 1.2 cm) within left lobule. Radioactive iodine was given to patient after surgery.
Image: Pituitary MRI of patient
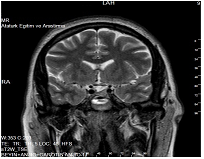
Picture 1. Papillary thyroid carcinoma Picture 2. Follicular thyroid carcinoma
CONCLUSION: Underlying pathological cause of most pituitary adenomas remains unclear despite the recent identification of a number of potential molecular genetic abnormalities. Pituitary tumor transforming gene (PTTG) initially isolated from pituitary tumor cells. PTTG protein is expressed at higher than normal levels in several tumors, including those of the pituitary, thyroid, colon, ovary, testis, breast and hematopoietic neoplasms. Co-existence of three endocrine tumors in our case may be caused from different causes. It may be releated with the potential molecular genetic abnormalities like PTTG. Or, incidental occurrence of them may be a reason, because each tumor occurs with a high prevalence in general population.
142 - Temporary adrenal failure due to tuberculosis: a rare phenomenon in recent years - 2014
Uluslararası Bildiriler P-240, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Tuberculosis is the most commonly encountered cause of Addison's disease. The exact status of adrenal reserve in tuberculosis still remains controversial, and recovery of adrenal function is unpredictable. There are few reports in the literature suggesting that adrenal insufficiency may improve with anti-tuberculosis therapy during the active phase of the disease. Herein,we presented a case of reversible adrenal failure in a patientwith activetuberculosis.
CASE REPORT: A 50-year-old female patient was admitted to our clinic with the complaints of weakness and darkening of the skin. In her history, she had receivedanti-tuberculosis treatment for the last 8 months. On her physical examination, she had hypotension and hyperpigmentation. Other systemic examinations were in normal ranges. Laboratory findings were presented in Table 1. Thyroid function tests were within normal range, and cortisol and adrenocorticotrophic hormone (ACTH)were 8 µg/dLand 802 pg/mL, respectively.There was no cortisol response to cosyntropin stimulation test, (30th minute cortisol was 10 µg/dL,and 60th minute was 11 µg/dL).Then, we started glucocorticoid therapy.In magnetic resonance imaging, thickness of both adrenal glands were increased.Anti-21 hydroxylase antibody was negative. Anti-tuberculosis treatment were stopped at the 9th month. We repeated the cosyntropin test one month after the therapy was stopped. We detected there was a positive cortisol response to ACTH (cortisol was 25 µg/dL at30th minute and 29 µg/dL at 60th minute). We stopped the glucocorticoid since we thought adrenal failure improved.
Table 1. Laboratory findings of the case
normal range | ||
Hemoglobin(gr/dl) | 12.9 | 12-16 |
Hemotocrit (%) | 37.6 | 36-45 |
Platelet (mm3) | 189000 | 150000-450000 |
Leukocyte (mm3) | 4700 | 4000-11000 |
Glucose (mg/dl) | 72 | 74-106 |
Creatinine (mg/dl) | 0.65 | 0.5-1.2 |
Sodium (mmol/L) | 132 | 136-145 |
Potassium(mmol/L) | 4.9 | 3.5-5.1 |
Aspartate aminotransferase (U/L) | 23 | 0-32 |
Alanine aminotransferase (U/L) | 8 | 0-33 |
Cortisol (µg/dl) | 8.0 | 6.2-19.4 |
Adrenocorticotrophichormone(pg/ml) | 802 | 0-60 |
CONCLUCIONS: Adrenal tuberculosis is witnessed in up to 6% of patients with active tuberculosis and is usually bilateral. Adrenal destruction via tuberculosis may cause overt or subclinical adrenal insufficiency. Adrenal cortex has a considerable capacity to regenerate with marked hyperplasia and hypertrophy of cortical cells, noted during the period of active infection. Reversal of adrenal function following anti-tubercular therapy is a controversial issue (1,2). Barnes et al. (2) reassessed adrenal function following the therapy and showed that short synacthin test returned to normal in all patients except one, suggesting adrenal dysfunction to be uncommon and antitubercular drugs that have a favorable effect on adrenal function. While some of the studies showed normalization of adrenal function following therapy in a large number of cases, others indicated a contradicted result. In their study, Prasad et al. (3) evaluated adrenocortical reserve and morphology in tuberculosis and reported that the compromised adrenal reserve and enlargement seemed to reverse with therapy. In a recent study byLaway et al. (4), adrenal cortical function and morphology before and after treatment of pulmonary tuberculosis were investigated, and it was reported that basal and stimulated cortisol is less in patients with pulmonary tuberculosis as compared with healthy controls and increases after antitubercular treatment. We suggest that patients who are diagnosed to have adrenal failure due to tuberculosis should be reevaluated after completion of anti-tuberculosis treatment with dynamic tests.
References
1) Penrice J, Nussey SS. Recovery of adrenocortical function following treatment of tuberculous addison’s disease. Postgard Med J 1992;68: 204-5.
2) Barnes DJ, Naraqi S,Temu P, Turtle JR. Adrenal functions in patient with active tuberculosis. Thorax 1989;44:422-4.
3) Prasad GA, Sharma SK, Mohan A, Gupta N, Bajaj S, Saha PK, Misra NK, Kochupillai NP, Pande JN. Adrenocortical reserve and morphology in tuberculosis. Indian J Chest Dis Allied Sci. 2000;42(2):83-93.
4) Laway BA, Khan I, Shah BA, Choh NA, Bhat MA, Shah ZA. Pattern of adrenal morphology and function in pulmonary tuberculosis: response to treatment with antitubercular therapy. Clin Endocrinol (Oxf) 2013;79(3):321-5.
141 - A huge metastatic adrenocortical carcinoma presenting with Cushing’s syndrome and inferior vena cava thrombosis: case report - 2014
Uluslararası Bildiriler P-217, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: Adrenocortical carcinoma (ACC) is a very rare but typically aggressive malignancy. About one quarter to three quarters of ACC is functioning with excess hormonal production.
CASE: A 44 years-old female patient was admitted to out-patient clinic with obesity, oligomenorrhea and abdominal pain. She had central obesity, buffalo hump, and palpable flank mass. Hypertension, transient ischemic attack and epilepsy history was present. Serum cortisol, dehydroepiandrosterone sulfate (DHEAS) and testosterone levels were elevated. Cushing’s syndrome was diagnosed by elevated urine free cortisol and a non-suppressible dexamethasone test. Serum aldosterone and renin activity, 24 hr urinary catecholamines were normal. Abdominal computerized tomography (CT) detected a 16x11 cm hypodense solid mass lesion at the right adrenal gland. It showed inhomogeneous appearance, irregular margin, neovascularization, liver invasion and inferior vena cava (IVC) thrombus extension (2.3x2.2 cm). It was adherent to the liver, kidney, and IVC (Image 1). Because of the unresectable adrenal mass, CT-guided abdominal mass biopsy was performed, and the diagnosis of ACC was made on the basis of pathology and immunohistochemistry. According to the AJCC staging system, the tumor was classified as T4NXM1, stage IV.Mitotane 4.5 gr/day and glucocorticoid was started. Also, warfarin was started due to presence of thrombus .The mean level of total testosterone and DHEAS tended to decrease during the follow-up. After 5 month, radiotherapy and chemotherapy (Cisplatin and Etoposide/3 cycle) were given to patient. Tumor regressed to 10x7.6 cm and IVC thrombus extension also regressed to 2.2x1.4 cm (Image 2). The patient showing partial remission underwent operation, but because of invasion to adjacent tissues, the tumor could not be resected.
CONCLUSION: Adrenal tumors in association with venous thrombosis are rare pathological conditions. No effective adjuvant treatment is currently available. We report a case of stage IV adrenocortical cancer with IVC thrombus extension and partial clinic response to the chemoradiotheraphy.
Image 1:Before treatment Image 2: After treatment

Table. Laboratuary parameters of patient after Mitotane, radiotherapy and chemotherapy.
Basal levels | After 12 weeks Mitotane therapy | After Chemotherapy and Radiotherapy | |
TSH (0.27-4.2mIU/mL) | 0.5 | 0.9 | 0.039 |
fT4 (0.9-1.7 ng/dl) | 0.7 | 0.6 | 0.9 |
fT3 (2-4.4 pg/ml) | 2.5 | 2 | 2.8 |
Cortisol (6.2-19.4 ug/dl) | 27 | 7.1 | 5.3 |
ACTH(0-60pg/mL) | 1 | 1 | 2 |
Totaltestosterone (0.006-0.82 ng/ml) | 0.82 | 0.55 | 0.5 |
Free testosterone (0.29-3.18 pg/ml) | 3 | 5.1 | 1.28 |
DHEAS (0-340 ng/ml) | 884 | 312 | 22.3 |
FSH(3.5-12.5mIU/L) | 10.4 | 47.3 | 65.4 |
LH (2.4-12.6mIU/L) | 4.7 | 31.1 | 36.1 |
Estradiol (12.5-166pg/ml) | 36.5 | 18.3 | 5 |
140 - The change in paratyroid hormone level by posture in primary hyperparathyroidism - 2014
Uluslararası Bildiriler P-153, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: Major factor that modulates the parathyroid hormone (PTH) secretion is serum calcium (Ca) level. Paratyhyroid gland also receives direct autonomic innervation. To date, measurement of several hormones such as cortisol, prolactin, renin and aldosteron were found to be affected by changing the posture from recumbent to the upright position. In the present study, we aimed to investigate postural change of PTH in normal individuals and patients with primary hyperparathyroidism (PHPT).
MATERIALS AND METHODS: 23 patients with PHPT and 9 age healthy controls were enrolled in our study. Blood samples were taken from all indivuduals after 12 hours of fasting. Following replacement of an intravenous catheter, the patients were requested to rest in bed in recumbent position but not sleeping for an hour and blood samples were obtained for PTH and Ca measurements at the 45 th and 60 th minutes of resting.Afterwards, the patients changed the posture to the upright position and stood up for an hour and again blood samples were obtained at the 45 th and 60 th minutes of standing. Pulses and blood pressures of all individuals were recorded in both postures.
RESULTS: In the group of patients with PHPT, mean serum PTH was measured as 75.36 pg/ml which is higher during upright position compared to recumbent position and the difference was statistically significant. In the control group mean serum PTH was measured only 3.09 pg/ml higher during the upright postion compared to recumbent position and the difference didn’t reach statistical significance. In both groups, Ca was higher when the patient was in the upright postion compared to the recumbent position.
CONCLUSION: It was reported that total calcium measurement increases in upright posture which should normally decrease the measured PTH level. However PTH secretion is autonomic in PHPT and increased in upright position regardless of serum Ca level.
Table 1. Comparisions of 45 th and 60 th minutes measurements of Ca and PTH within the control ant the patient groups
Variables | 45 th min | 60 th min | p-value |
PTH Recumbent | |||
Control Group | 42.2 (14.2-56.0) | 43.6 (14.3-57.1) | 0.314 |
Case Group | 151.5 (31.0-932.0) | 154.9 (31.3-926.0) | 0.242 |
PTH Upright | |||
Control Group | 45.9 (17.5-69.3) | 38,0 (16,5-73,0) | 0.374 |
Patient Group | 206.5 (56.4-1161.0) | 206,1 (54,1-1218.0) | 0.256 |
Ca Recumbent | |||
Control Group | 9.04±0.31 | 9.10±0.31 | 0.014 |
Patient Group | 10.92±0.94 | 10.77±0.34 | 0.429 |
Ca Upright | |||
Control Group | 9.51±0.37 | 9.56±0.30 | 0.400 |
Case Group | 11.44±1.01 | 11.54±1.12 | 0.183 |
Table 2. Other clinical parameters of the control and the patient groups
Variables | Control Group | Patient Group | p-value |
Delta PTH | 1.7 (-4.4 - 14,6) | 47.7 (5.9 - 289,3) | <0,001 |
Delta Ca | 0.46±0.10 | 0.65±0.28 | 0,065 |
PTH change(%) | 3.5 (-9.6 - 31.6) | 33.3 (6.8 - 93.7) | <0,001 |
Ca change (%) | 5.4 (3.1 - 6.7) | 5.7 (1.4 - 18.9) | 0.334 |
139 - Hypoparathyroidism and celiac disease a rare autoimmune disease combination - 2014
Uluslararası Bildiriler P-147, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
CASE: A 30-years-old man with hypoparathyroidism who has been treated with calcitriol and calcium for two years, admitted to our hospital with persisting diarrhea. An endoscopic procedureis plannedfor his complaint.But he was waiting for this examination as outpatient condition, he had a convulsion and had been taken in hospital by parents. Initial laboratory analyses revealed that he was hypocalcemic (total calcium of 6 mg/dL), and Parathormone (PTH)level was;8 pg/mL(normal range; 15-65) , phosphorus level 5,7 mg/dL(normal range; 2.5-4.5) and magnesium level was 2 mg/dL(normal range;1,5-2.5). He was treated with intravenous calcium gluconate urgently. Then treated with oral calcium carbonateand calcitriol with a stepwise increase in the dosage. An upper gastrointestinal system endoscopy has applied to the patient. Diagnosis of gluten-sensitive or celiac disease was suggested at endoscopy, due to flat mucosa and confirmed by histological findings in duodenal biopsy including absent villi, crypt hyperplasia and lymphocytic infiltration in the epithelium. Serologic examination confirmed the diagnosis. After then he was placed on gluten-free diet, which rapidly lead to the normalization of his bowel habits and improved his metabolic parameters. The needed drug dosage is decreased.
CONCLUSION: Hypoparathyroidism is an uncommon endocrine-deficiency disease characterized by low serum calcium levels, elevated serum phosphorus levels, and absent or inappropriately low levels of PTH in the circulation. Afterpostoperative hypoparathyroidism, autoimmune hypoparathyroidism is the next most common form of hypoparathyroidism in adults. Patients with hypoparathyroidism most often present with paresthesia, cramps, or tetany, but the disorder also may manifest with acute seizures, bronchospasm, laryngospasm, or cardiac rhythm disturbances. Autoimmune hypoparathyroidism may be isolated or part of an autoimmune polyglandular syndrome. Celiac disease and autoimmune hypoparathyroidism togetherness is a very rare condition but the possibility of celiac disease should be considered in patients with hypoparathyroidism that seems unduly difficult to treat.
138 - Functional parathyroid cyst: a rare cause of hypercalcemia - 2014
Uluslararası Bildiriler P-136, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: Primary hyperparathyroidism (PHPT) is usually caused by single adenoma. Functional parathyroid cysts are a rare cause of PHPT. Parathyroid cysts can be subdivided into nonfunctional, without biochemical derangement, or functional, with elevated serum calcium accompanying clinical evidence of hyperparathyroidism. Parathyroid cysts are found in the neck and anterior mediastinum. Functional parathyroid cysts are not only secretary, larger cysts can lead to compression symptoms, including dysphagia, dyspnea, cough, stridorand hoarseness. Mediastinalparathyroid cysts are usually presented as asymptomatic and identified accidentally by a routine chest X-ray or computed tomography (CT). We present a case of a patient with a functional parathyroid cyst.
CASE: A 66-year-old male patient referred to our department because of hypercalcemia and anterior mediastinal mass determined on thorax CT which is performeddue topulmoner suspicion of pulmonary embolism.He had no symptom of hypercalcemia except history of nephrolithiasis. Biochemical test revealed hypercalcemia (12.24 mg/dl; normal range:8.8-10.2), and hyperparathyroidism (parathyroid hormonelevel 140.6 pg/ml; normal range:15-65), also phosphorus level was 2.98 mg/dl(normal range:2.5-4.5), creatine 0.84 mg/dl(0,71,2), vitamin D level was 11.4 mg/Land 24-hour urinary calcium excretion was 504 mg/day. Renal ultrasonography determined 7 mm renal stone in the left kidney. Bone mineral dansitometry revealed osteopenia. Thorax CT scan revealed a 4.7x3.3 cm sized solid mass, located onanterior mediastinum. After initiating of adequate hidration and furosemide treatment for hypercalcemia, the patient referred to chest and chest surgery department because of the anterior mediastinal mass and pulmonary embolism detected on thorax CT.
The surgery decision was made because of the CT mass appearance. After removal of the mass calcium and parathyroid levels were reduced to normal levels. Pathologic examination revealed the diagnosis of a parathyroid cystic.
CONCLUSION: Mediastinal parathyroid cyst is an uncommon cause for hypercalcemia. Also it is difficult to establish a preoperative definitive diagnosis.
Picture 1. Torax CT of the patient

Picture 2. Pathology specimen of the patient
137 - The relationship between microvascular complications and vitamin D deficiency in type 2 diabetes mellitus microvascular complications and vitamin D deficiency - 2014
Uluslararası Bildiriler P-130, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
Aim: Vitamin D deficiency is reported as a risk factor for the development of diabetes in several epidemiologic studies. In this study, we investigated the frequency of 25-OH vitamin D defciency in type 2 diabetes and the relationship between 25-OH vitamin D defciency and microvascular complications.
Materials and methods: Retrospectively, medical records of 557 type 2 diabetic patients admitted to the Endocrinology Outpatient Clinic in JanuaryÐMarch period and 112 healthy
controls who were randomly selected among individuals admitted to the hospital for a check-up and had a laboratory result of 25-OH vitamin D level were screened. The level of 25-OH vitamin D in type 2 diabetes and the relationship between 25-OH vitamin D deÞciency and microvascular complications are investigated.
Results: There was not statistically signifcant difference in terms of 25-OH vitamin D levels between diabetic and control group. No correlation between HbA1c and vitamin D levels was found. 25-OH vitamin D level was lower in diabetic patients with nephropathy. Also patients not using any medication and followed by only dietary suggestion, had nephropathy in higher frequency.
Conclusion: Vitamin D deficiency is more common in diabetic patients with nephropathy. Upon evaluation of the total microvascular complications, vitamin D level was also lower. Vitamin D defciency is associated with microvascular complications of diabetic patients.
136 - Teriparatide treatment in a patient with severe pregnancy related osteoporosis - 2014
Uluslararası Bildiriler P-84, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: Pregnancy or lactation related osteoporosis(PLO) is very rare. It usually occurs in the third trimester or in the early post partum period and manifestations are severe back pain and loss of height due to vertebral fractures.Its etiology is not well understood.Classical treatment is cessation of lactation, calcium and Vit-D supplementation and biphosphanates in chosen cases.All osteoporosis drugs are approved mainly for post-menouposal osteoporosis and reports of teriparatide treatment in this group of patients is off label worldwide.Here we represented a case with severe pregnancy related osteoporosis to whom we started teriparatide treatment.
CASE: 23-years-old female patient admitted at the post partum 2nd week with complaints of severe back pain.She denoted that pain started in the last month of her pregnancy and persisted after labour despite calcium and vit-D supplementation. Her body mass index (BMI)was 24 kg/m2, she had regular menstrual cycles, and she didn’t have any risk factors for osteoporosis such as smoking, corticosteroid usage or family history.Thyroid functions, parathormone level, celiac markers, kidney and liver function tests, serum calcium (Ca), phosphorous (P)and vitamineD levels were in normal ranges. We detected multiple vertebral fractures at T5,T7,T10,T11,T12 and her total vertebrate Z score was -4.2 where as femur neck Z score was -1on bone mineral densitometry (BMD). We have initiated teriparatide therapy 20 µg/day along with 1000 mg calcium and 800 IU cholecalciferol per day.Thorocal orthosis was also prescribed. At the second month of therapy her pain was totally relieved.At the 6 th month of therapy BMD was increased15%at the lumbar spine and we continued the therapy.
CONCLUSION: Effective treatment of PLO is controversial.There are some concerns about biphosphanates in premenouposal age group because of possible adverse effects on fetus.They accumulate in bone and can cross placenta despite withdrawal.In previous reports teriparatide caused increased BMD up to36% .It can also prevent futher vertebral fractures.Therefore it can be a reasonable choice for treatment.
Table. Labaratory data of the patient
Patient Result | Normal Range | |
Serum Ca | 9 mg/dl | 8.5-10.2 |
Serum P | 4.3 mg/dl | 2.5-4.5 |
PTH | 32 pg/ml | 15-65 |
Creatine | 0.8 mg/dl | 0.1-1.2 |
TSH | 1.2 uIU/ml | 0.4-4.5 |
Vitamin D | 24 ug/L | 10-80 |
ALT / AST | 10/ 13 U/L | 0-33 |
Osteocalcine | 30.19 ng/ml | 13-46 |
N- Telopeptide | 0,76 ng/ml | 0.016-0.58 |
C- Telopeptide | 0.75 ng/ml | 0.104-1.008 |
Figure. Loss of height in the thorocal vertebrates of the patient


135 - Does testosteron have an effect on bone mineral density in post-menopausal women? - 2014
Uluslararası Bildiriler P-78, 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
Background: Osteoporosis is a common problem in postmenoausal women. There is limited data about the physiological importance of endogenous testosterone on bone mineral density (BMD) in older women is poorly understood.
Aim: The aim of this study was to evaluate association of endogeneous testosterone with BMD and BMI.
Materials-methods: This cross-sectional study included 64 patients (45-85 year) postmenopausal women; their demographic features, BMD and serum total testosteron levels and relationship between testosterone and BMD were evaluated. When the patients divided into three cathegories according to BMD; Group 1A: normal; Group 1B: osteopenic; Group 1C:osteoporotic.
Results: Serum total testosterone levels were found not to be correlated with BMD. We didn’t find any differences in serum testosterone levels between three BMD groups.
Conclusion: This study suggests that endogenous androgens are influential on bone density in postmenopausal women. However, we didn’t find any relationship. Effects of endogenous testosterone level on BMD is controversial.
134 - A difficult case of ectopic Cushing’s syndrome due to ACTH-producing pheochromocytoma presented with normal fractionated urinary catecholamines and metanephrines - 2014
Uluslararası Bildiriler 16th European Congress of Endocrinology, 3 - 7 May 2014, Wroclaw, Poland, Endocrine Abstracts May 2014 Volume 35, ISSN 1479-6848
ABSTRACT
BACKGROUND: Ectopic ACTH secretion by pheochromocytoma causing Cushing’s syndrome has been reported rarely. Here, we present a patient with ectopic ACTH-dependent Cushing's syndrome, caused by a pheochromocytoma with normal fractionated 24-h urinary catecholamines and metanephrines.
CASE: 48- year old female patient admitted to our clinics with the complaints of severe hypertension despite receiving anti hypertensive therapy. Severe headache, malaise, nausea , vomiting, proximal muscle weakness, weight loss and palpitation episodes were the accompanying symptoms. In her physical examination, she was anxious and depressive. Her pulse was 140/minute, blood pressure was 200/100 mmHg. She didn’t have any typical sign of Cushing syndrome except proximal myopathy. Labaratory tests were significant for severe hypokalemia (2.5 mmol/L), hypoalbuminemia (2.6 g/dl). Her serum cortisol concentration was 63.4 μg/dL and it wasn’t supressed after 1 mg and 2 days 2 mg dexamethasone suppression tests (DST). 24-h urinary free cortisol was extremely high (18980 μgr/day) whereas urinary fractionated catecholamines and metanephrines were normal. Her serum ACTH was measured with IRMA and was found as 289.3 pg/ml. Our initial endocrinologic diagnosis was ACTH-dependent ectopic cushing syndrome since there wasn’t any supression with high dose DST, treatment resistant hypokalemia, negative pitiutary imaging and dramatic and rapidly progressing clinics. Abdominal computed tomography (CT) scan revealed a 43x37 mm tumoral mass in the left adrenal gland and PET-CT showed a 5-cm sized lesion in the left adrenal gland with high SUVmax (18.7) and hyperplasia in the other adrenal. She was underwent right adrenalectomy with Addison and pheochromocytoma protocol. After operation pathological examination was compatible with pheochromocytoma, and immunostained with ACTH extensively
Picture 1. Abdominal CT of the patient
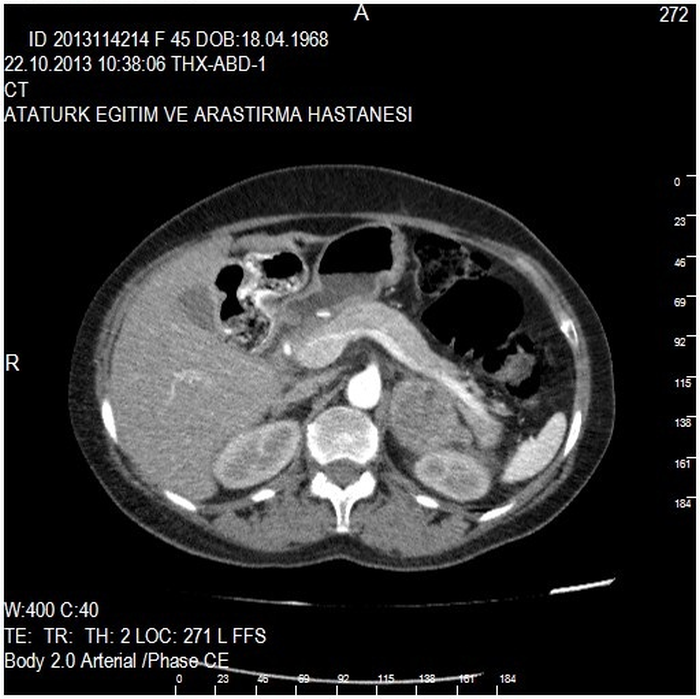 |
Picture 2. PET-CT of the patient
CONCLUSION: Ectopic ACTH-secreting pheochromocytoma is a diagnostic challenge for the clinicians. Serum or urinary metanephrines and catecholamines are very sensitive and specific tests for the diagnosis of pheochromocytoma but negative results may occur and lead to confusion in the diagnosis. |
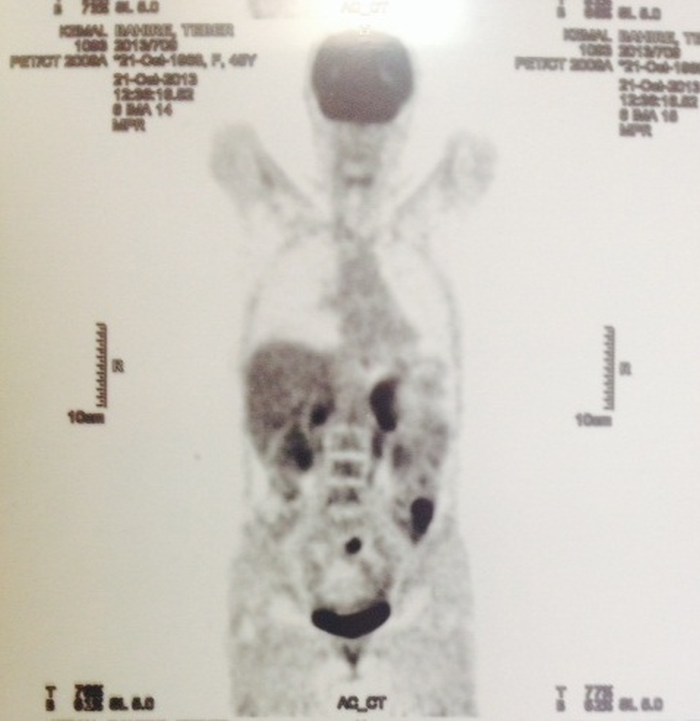
133 - Diagnostic value of endoscopic ultrasonography for preoperative localization of parathyroid adenoma - 2013
Uluslararası Bildiriler PP5, 5th European EGEUS Congress, November 21-22, 2013, Istanbul, Turkey
ABSTRACT
INTRODUCTION: Primary hyperparathyroidism (PHPT) is characterized by hypercalcemia and concomitant inappropriate secretion of parathyroid hormone (PTH) and isthe most common cause of hypercalcemia in the outpatient setting .PHPT is caused by adenomas (80-85%), four-gland hyperplasia (10-15%), and rarely due to carcinoma (0.8-2%).Conventional non-invasive imaging modalities are ultrasonography (US) and 99mTechnetium methoxyisobutylisonitrile (99mTc-MIBI) scintigraphyfor enlarged parathyroid lesions.99mTechnetium MIBI single-photon emission computed tomography (CT) and/or magnetic resonance imaging (MRI) can be used in cases of failure to detect small or ectopic tumors with those modalities. Endosonography (EUS) images lesions using a high frequency ultrasound probe, providing detailed visualization of the esophagus, stomach, and duodenum. Lesions in the mediastinum or near the esophagus can be detected with EUS, and a US-guided biopsy can be performed.A few small studies have evaluated the effectiveness of EUS for localizing parathyroid lesions before surgery. The purpose of the present study was to determine the diagnostic accuracy of EUS in terms of localizing parathyroid adenomas compared with those of US and 99mTc-MIBI scintigraphy findings. When compared to the previous reports in the literature, our study was conducted with the highest number of patients. Another outstanding and important feature of our study is inclusion of solely parathyroid adenomas.
METHODS: Forty-seven patients with a PHPT diagnosis and who were recommended for surgery were enrolled in this study. An endoscopist who was blinded to the previous US and 99mTc-MIBI scintigraphy results performed the EUS in each patient.
RESULTS: Thirty-nine female and eight male patients with PHPT were evaluated. The presence of adenoma was confirmed by subsequent postsurgical pathology results. One case was excluded because the histopathological evaluation was compatible with a lymph node, although the lesion was detected using three different imaging modalities preoperatively. Demographic data, distribution of adenomas according to location and the true positive rates of the imaging modalities are listed in Table 1. The locations of the parathyroid adenomas were correctly documented by US in 39 patients (84.7%) by 99mTc-MIBI scintigraphy in 35 (76.0%), and by EUS in 44 (95.6%) of 46 patients. EUS located all 31 adenomas detected previously with US and 99mTc-MIBI scintigraphy. EUS also successfully located three adenomas that could not be identified by US and 99mTc-MIBI scintigraphy. The positive predictive value and diagnostic accuracy of EUS, US, and 99mTc-MIBI were 97.7, 97.7, and 95.6%; 88.6, 97.5, and 86.9%; and 77.7, 97.2, 76.0%, respectively(Table 2). The location of the parathyroid adenoma was correctly documented by US in 39 (84.7%) Image of the parathyroid adenoma taken during EUS examination is shown in Figure 1.
CONCLUSION: Preoperative localization of parathyroid pathology is important in appropriate cases of MIP. When the efficacy, comfort, cost, and low complication and morbidity rates of MIP are considered, EUS facilitated identification of lesions in patients in whom MIBI and US failed but did not need bilateral neck surgery and so were candidates for MIP. Therefore, EUS was a safe and effective imaging tool for parathyroid adenomas that could not be localized by US and parathyroid scintigraphy.
Table 1. Baseline demographical, clinical, and laboratory findings in patients with PHPT
N=47 | |
Age (year) | 51.48 ± 14.49 |
Male / Female (%) | 8/39 (17/83) |
Serum calcium (8.6-10.2 mg/dL) | 11.59 ± 1.30 |
Serum phosphours (3.5- 4.5 mg/dL) | 2.48 ± 0.54 |
Serum parathyroid hormone (11-67 pg/mL) | 285.98 ± 127.96 |
25-OH vitamin D (20- 120 µg/L) | 13.79 ± 8.50 |
Volume (cm3) | 2.05 ± 2.41* |
True positive rates of imaging methods (%) | |
Ultrasonography | 39/46 (84.7) |
99mTc-MIBI scintigraphy | 35/46 (76.0) |
Endoscopic Ultrasonography | 44/46 (95.6) |
Location of adenomas after operation | |
Lower left (%) | 22/45 (48.8) |
Upper left (%) | 3/45 (6.6) |
Lower right (%) | 17/45 (37.7) |
Upper right (%) | 3/45 (6.6) |
Mediastinum | - |
Histopathology | |
Adenoma | 45/47 (95.7) |
Hyperplasia | 1/47 (2.2) |
Carcinoma | - |
Surgery failure | 1/47 (2.2) |
Table 2. Sensitivity, positive predictive value and diagnostic accuracy rates of the imaging methods
US | 99mTc-MIBI scintigraphy | EUS | |
Sensitivity (%) | 88.6 | 77.7 | 97.7 |
Positive predictive value (%) | 97.5 | 97.2 | 97.7 |
Diagnostic accuracy (%) | 86.9 | 76.0 | 95.6 |
Fig 1. Endoscopic ultrasonography image of the parathyroid adenoma, showing a well-defined hypoechoic, solid lesion
132 - Thyroid cancer rate in patients who underwent total thyroidectomy with the diagnosis of TNG - 2013
Uluslararası Bildiriler P-218, 37th Annual Meeting of the European Thyroid Association, Leiden, The Netherlands, September 7-11, 2013
ABSTRACT
AIM: Datas in literature about coincidence of toxic nodular goiter and thyroid cancer,clinical features and prognosis is debating. In this study we aimed to evaluate rate of thyroid cancer,clinical findings and tumor fetaures in patients who underwent total thyroidectomy with the diagnosis of toxic nodular goiter.
MATERIALS AND METHODS: Patients who have been applied to Endocrinology and Metabolism outpatient clinic in Ankara Ataturk Education and Research Hospital between March 2006-January 2012 with the diagnosis of toxic adenom and underwent total thyroidectomy were included to the study and they have evaluated in a multidisciplinary council consisted of endocrinologist, general surgeon, pathologist and nuclear medicine experts.
RESULTS: According to pathological findings, totally 77 nodules obtained from 77 patients were divided into two groups as benign (n=63, %81.8) and malignant (n= 14,%18.2) respectively. In malignant group, 10 (%71.4) patient’s malignant foci were inside of the adenoma and malign foci of 4 (%28.6) patients were in the parenchyma . 9 papillary microcarcinomas,3 papillary carcinomas and 2 microinvasive follicular carcinomas were identified in malign nodules. Mean tumor diameter was 8 mm in the carcinomas that located inside of adenomas. Any case of relapse , distant metastases or death did not occur among malign patients during follow up. In our study patients with toxic nodular goitre,diagnostic sensitivity of fine needle aspiration biopsy was %16.7 and specifity was %96.3 ; but it’s observed that in differantial diagnosis,fine needle aspiration biopsy doesn’t have significant determination. None of the morphological findings which established by USG, is determinating in the differantial diagnosis.
CONCLUSION: RAI and surgery may be the choices for the definitive treatment of toxic nodular goitre. It’s important to exclude malignancy while choosing appropriate treatment due to probability of incidentally discovered thyroid cancer rate. In conclusion we think that while planing definitive treatment of toxic nodular goitre ,especially surgery should be preferred.
Table 1. Histopathologic findings
Histopathology | n | % |
Benign | 63 | 81.8 |
Malign | 14 | 18.2 |
Papiller microcarcinoma | 9 | 11.7 |
Papiller carcinoma | 3 | 3.9 |
Microinvasive follicular carcinoma | 2 | 2.6 |
Malignancy in nodule | 10 | 13 |
131 - Thyroid autoimmunity in patients with hyperprolactinemia: an observational study - 2013
Uluslararası Bildiriler P-103, 37th Annual Meeting of the European Thyroid Association, Leiden, The Netherlands, September 7-11, 2013
ABSTRACT
INTRODUCTION: It has been suggested that deviations of prolactin (PRL) levels from the normal range can result in significant alterations in the immune system. We attempted to establish whether there is a relationship between hyperprolactinemia and primary thyroid disorders with the focus on patients with autoimmune features.
METHODS: The medical records of 100 patients with hyperprolactinemia (HPRL) admitted to our endocrine unit from 2005 to 2013 were retrospectively examined. Records of thyroid ultrasonography (USG), basal serum levels of thyroid stimulating hormone, circulating free thyroxine, free triiodothyronine, antithyroglobulin (anti-Tg) and antithyroperoxidase (anti-TPO) antibodies were analyzed. In 100 control subjects, matched by age and gender with HPRL patients, thyroid USG, thyroid function tests (TFTs) and autoantibody panel were obtained.
RESULTS: The median PRL in patients was 93 ng/ml(range: 37-470). Twenty-five patients (25%) and 22 controls (22%) had positive anti-Tg and/or anti-TPO titre (P=0.739). The median serum PRL was 98 (37-470) ng/ml in patients with positive thyroid autoantibodies and 92 (40-470) ng/ml in patients who tested negative for thyroid autoantibodies (P=0.975). Among the individuals with autoantibody positivity TFTs abnormalities were more frequent in HPRL patients (60%, 14 subclinical hypothyroidism and one hyperthyroidism out of 25) than in controls (9.1%, 2 subclinical hyperthyroidism out of 22) (P<0.001)Twenty-seven patients with HPRL and 31 controls had goiter (27 vs 31%, P=0.437). Forty-six patients (46%) and 50 (50%) control subjects had one or more of the features of thyroid disorder which are goiter, positive thyroid autoantibody and thyroid function abnormality (P=0.888).
CONCLUSION: HPRL may be associated with more severe thyroid dysfunction in patients with thyroid autoimmunity.
Table 1. Thyroid function tests and autoantibody panel of the patients with hyperprolactinemia (HPRL) and control subjects.
Patients (n=100) | Control (n=100) | P | |
Serum TSH | 2.2 (0.01-9.2) | 1.9 (0.01-5.7) | 0.322 |
Serum fT3 | 3.2 (1-4.6) | 3.3 (2.3-4.4) | 0.132 |
Serum fT4 | 1.1 (0.3-1.8) | 1.2 (0.8-1.7) | 0.09 |
TFTs | |||
Euthyroidism (%) | 73 | 95 | |
Hyperthyroidism (%) | 1 | <0.001 | |
Hypothyroidism (%) | - | ||
Subclinical Hypothyroidism (%) | 25 | 3 | |
Subclinical Hyperthyroidism (%) | 1 | 2 | |
Anti-Tg Positivity (%) | 16 | 10 | 0.207 |
Anti-TPO Positivity (%) | 19 | 17 | 0.712 |
Antibody Positivity (%)a | 25 | 22 | 0.739 |
Thyroid USG | |||
Normal (%) | 50 | 41 | |
Goiter (%) | 27 | 31 | 0.437 |
Thyroiditis (%) | 23 | 28 |
TSH, thyroid stimulating hormone; fT3, free triiodothyronine; fT4, free thyroxine; anti-Tg, antithyroglobulin antibody; anti-TPO, antithyroperoxidase antibody; TFTs, thyroid function tests; USG, ultrasonography. Parametric values was expressed as mean±S.D. Statistical significance was set a P value of 5%.
Normal values: fT3: 1.8-4.6 pg/ml , fT4: 0.9-1.7 ng/dl , TSH: 0.27-4.2 uIU/ml. a Positivity of anti-Tg and/or anti-TPO.
130 - Primary thyroid disorders in patients with endogenous hypercortisolism and the role of immune dysregulation: an observational study - 2013
Uluslararası Bildiriler P-101, 37th Annual Meeting of the European Thyroid Association, Leiden, The Netherlands, September 7-11, 2013
ABSTRACT
INTRODUCTION: Endogenous Cushing’s syndrome (CS) is a nonphysiological hypercortisolism state which causes a reversible state of immunosuppression. Autoimmune diseases have improved during the active phase of CS whereas there is a risk of worsening of the same conditions upon remission. CS may alter the performance of the hypothalamic-hypophyseal-thyroid axis in several ways as well [6]. In this study we attempted to establish whether there is a relationship between hypercortisolism and primary thyroid disorders with the focus on patients with autoimmune features.
METHODS: The medical records of 40 patients with Cushing’s syndrome (CS) admitted to our endocrine unit from 2006 to 2013 were retrospectively examined. Pre-surgical records of thyroid ultrasonography (USG), basal serum levels of thyroid stimulating hormone, circulating free thyroxine, free triiodothyronine, antithyroglobulin (anti-Tg) and antithyroperoxidase (anti-TPO) antibodies were analyzed. When available, data on thyroid function tests (TFTs) and autoantibody panel 6 months after surgery were also evaluated. Diagnosis of hypercortisolism had been established by an overnight low dose dexamethasone suppression test and urinary free cortisol (UFC) measured in 24-h samples. Etiological diagnosis was made by 8 mg dexamethasone suppression test, measurement of ACTH levels and imaging techniques. After treatment, all patients were cured which was established by the finding of subnormal serum cortisol concentrations and/or subnormal 24-h UFC levels. In 40 control subjects, matched by age and gender with CS patients, thyroid USG, TFTs and autoantibody panel were obtained.
RESULTS: Six patients (15%) and 7 controls (17.5%) had positive anti-Tg and/or anti-TPO titre at study entry, while 2 out of 25 patients (8%) developed positive anti-Tg and/or anti-TPO titre after disease cure (P>0.05). Sixteen patients with CS and 8 controls had nodular goiter (40 vs 20%, P<0.05). Regarding TFTs, one patient (2.5%) had subclinical hyperthyroidism and one (2.5%) had subclinical hypothyroidism whereas one control (2.5%) had hyperthyroidism. Twenty-one patients (52.5%) and 8 controls (20%) had one or more of the features of thyroid disorder which are goiter, positive thyroid autoantibody and thyroid function abnormality and the difference was significant (P=0.026).
CONCLUSION: There is a remarkably high prevalence of primary thyroid disorders in patients with CS but thyroid autoimmunity is not more frequent even during the resolution period of hypercortisolism.
Group 1A (n=40) | Group 1B (n=25) | Group 2 (n=40) | (P) Group 1A vs. 2 | (P) Group 1B vs. 2 | (P) Group 1A vs. 1B | |
Serum TSH | 1.3±1.2 | 1.6±1.2 | 2.2±1.3 | < 0.01 | 0.06 | 0.223 |
Serum fT3 | 3.1±0.8 | 3±0.8 | 3.4±0.7 | 0.09 | 0.035 | 0.814 |
Serum fT4 | 1.2±0.3 | 1.2±0.4 | 1.3±0.2 | 0.4 | 0.442 | 0.646 |
Anti-Tg Positivity (%) | 4 (10) | 4 (16) | 3 (7.5) | 0.692 | 0.253 | 0.371 |
Anti-TPO Positivity (%) | 4 (10) | 5 (20) | 5 (12.5) | 0.723 | 0.322 | 0.221 |
Antibody Positivity (%) | 6 (15) | 7 (28) | 7 (17.5) | 0.762 | 0.244 | 0.169 |
Group 1A: Pretreatment Cushing Syndrome patients
Group 1B: Posttreatment Cushing Syndrome patients
Group 2: Control patients
129 - Comparison of early total thyroidectomy with antithyroid treatment in patients with moderate to severely active graves’ orbitopathy, a randomized prospective trial - 2013
Uluslararası Bildiriler OP-83, 37th Annual Meeting of the European Thyroid Association, Leiden, The Netherlands, September 7-11, 2013
ABSTRACT
Objectives: We aimed to compare early total thyroidectomy with the anti-thyroid treatment regimens, in patients with moderate to severely active Graves' orbitopathy (GO) prospectively.
Methods: The inclusion criteria: Hyperthyroidism and GO developed in the last six months, thyroid volume ≥15 mL, no previous treatment except local interventions for GO. GO activity has been defined as clinical activity score (CAS) ≥3 and carrying at least one of the following criteria; Proptosis ≥21 mm in one eye, ≥2 mm difference between two eyes, presence of diplopia, lid aperture ≥9 mm. Initially, all the patients were made cuthyroid (TSH 0.4-1 mlU/L). Pulse methylprednisolone of total 4.5 gr were given intravenously to all patients before randomization. In the first group, patients were sent to total thyroidectomy and in the second group, patients were followed with antithyroid drugs. TSH was kept between 0.4-1 mlU/L
Results: 18 patients were randomized to total thyroidectomy (UT) group and 23 patients were randomized to medical antihyroid treatment (AT) group. There were no difference between the two groups with respect to age, gender, smoking habit, duration of hyperthyroidism and GO, thyroid volume, TSH, free T4, and TSH receptor antibody (TRAb) levels initially. The follow up period was 6-48 months. When the TT group was compared with AT group, TRAb were significantly decreased in TT group while there was no significant difference with respect to proptosis, lid aperture, CAS and diplopia between groups However in TT group additional pulse methylprednisolone treatment was given to 3 (21%) patients and urgent orbital decompression was applied to 2 (14%) of those patients. Hyperthyroidism reocurred in 3 patients in AT group after 18-24 months of antithyroid treatment.
Conclusion: Although the significant decrease of thyroid autoantibodies were achieved in TT group, this was not reflected as an beneficial effect on the course of GO.
128 - Treatment, follow up and prognostic factors of papillary microcarcinoma - 2013
Uluslararası Bildiriler P-1116, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Papillary thyroid microcarcinoma (PTMC) is the most frequent form of papillary thyroid carcinoma (PTC). İncidence rate of papillary thyroid microcarsinoma (PTMC) has almost doubled during the recent years but treatment and follow up is still a matter of debate. In this study we aimed to analyze clinical and histopathological risk factors at the time of diagnosis and to observe their implications for treatment, follow up and prognosis.
PATIENTS AND METHODS: Two hundred forty-eight patients were included in this study between january 2007 and november 2012. They were all evaluated in the outpatient clinic of Ankara Ataturk Education and Research Hospital Endocrinology Department with the diagnosis of nodular goiter. The age, sex, the method of diagnosis (incidental or with a clinical suspicion), cervical lymph node metastases and relapse and/or distant metastases during follow up were retrospectively recorded.
RESULTS: Two hundred one were female and 47 were male. Total thyroidectomy was performed in all patients. All of the patients had postsurgical radio-iodine ablation treatment. When compared according to tumor size (≤5 mm vs >5 mm), bilateral involvement, vascular invasion, capsular invasion, extrathyroidal extension and lymph node metastases were significantly more frequent in the patients with tumor size > 5 mm (p values p<0.046, p<0.021, p<0.001, p<0.003, p<0.000 respectively). Diagnosis after a clinical suspicion and thyroglobulin (TG) value were found to be associated with lymph node metastases at the end of the multiple logistic regression analysis.(Table2). The relevant TG value was 7.98 ng/ml with a sensitiviy of 57.14 % and specificity of 83.17 % [Positive predictive value (PPV): %19, negative predictive value (NPV): %96.6]. Relapse was associated with TG value and lymph node metastases at the time of diagnosis. Tumor size which predicts relapse was 6 mm with a sensitiviy of 50 % and specificity of 76.37 % [PPV: 8.2 %, NPV: 97.3 %].
Table 1. Clinical and pathological factors for worse prognosis by sizeand ratio
Group 1 ≤5 mm (n =127) | Group 2 >5 mm (n=121) | p | |
Bilateralite n, (%) | 17(13.4) | 28(23.1) | 0.046 |
Vasculer invasion n, (%) | 0 | 5(4.1) | 0.021 |
Capsüle invasion n, (%) | 10(7.9) | 27(22.3) | <0.001 |
Extratiroidal extension n, (%) | 7(5.5) | 21(17.5) | 0.003 |
lymph node metastases n, (%) | 2(1.6) | 16(13.2) | <0.000 |
Table 2. Multivariate regression analysis of factors that may affect the evaluation of lymph node metastasis
B | p | %95 CI | ||
Tumor size | 1.172 | 0.607 | 0.640 | 2.146 |
TG | 1.083 | 0.011 | 1018 | 1152 |
Diagnosiz | 0.095 | 0.043 | 0.010 | 0.928 |
Capsüle invasion | 1.359 | 0.740 | 0.223 | 8.281 |
Vasculer invasion | 0.181 | 0.317 | 0.006 | 5.146 |
Multifocality | 1.259 | 0.865 | 0.89 | 17.881 |
CONCLUSION: Local relapse and lymph node metastases are more frequent in patients with a tumor size of more than 6 mm or stimulated serum Thyroglobuline (TG) levels in post thyroidectomy period of more than 7.98 ng/ml. Local relapse is significantly associated with lymph node metastases at the time of diagnosis. Regarding the treatment of PTMC our approach is to perform total/near total thyroidectomy and than RAI treatment. We think that the low relapse in this study is related with our therapeutic approach. On the other hand, PTMC should not be regarded as a relatively benign disease when our patients with lymph node metastases, local relapse and distant metastases were taken into consideration.
127 - Incidental thyroid cancer frequency in total thyroidectomy for the graves disease patients and the effect of the presence of nodules on malignity rates - 2013
Uluslararası Bildiriler P-1107. 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Our objective for the current review was to investigate the thyroid cancer frequency rate within the patients who have had total thyroidectomy procedure for definitive Graves’ disease treatment and to evaluate the contribution of the presence of nodules to malignancy rates.
MATERIAL AND METHODS: The present study was conducted retrospectively.by scanning the data of 214 patients who were applied total thyroidectomy for permanent Graves disease treatment. The participants were separatedinto 3 subgroups;benign nodule group, malignant nodule group and nodulenegativegroup. The groups were also compared in regards to demographic characteristics and laboratory data.
RESULTS: 14 of the 214 cases were diagnosed with thyroid cancer. The malignancyprevalence was determined as 6.5%. The sex distributions were found to be statistically similar between the malignant and benign nodule groups (p=0.776). The mean age of the malignant nodule group was significantly higher than the benign nodule group (p=0.042). No significant differences was found between the benign and the malignant nodule group in regards to median Thyroid Stimulating Hormone (TSH)receptor antibody levels (p=0.134). The cases were divided into two groups regarding to nodüle presence.Pre-operational USG revealed nodules in 19 cases. Five of these patients had malignancy .The malignancy frequency was significantly higher in the nodule positive group than the nodule negative group (26.3% vs. 4.6% respectively, p=0.004). There was also no statistically significant TSH receptor antibody, Anti-thyroid peroxidase (Anti-TPO)antibody titres and thyroid functioning differencesbetween these groups (p> 0.05).
CONCLUSION: We have determined the incidental thyroid cancer frequency in Graves’ disease patients population as 6.5%.Malignancy rate was found higher when co-morbid nodules were present (26.3%). We recommend that when total thyroidectomyis performed for the treatment of Graves’ disease, especially if nodules are present, malignancyrisk must be takeinto consideration
Table 1.Comparison of benign and malignant groups according to nodule and TRAB positivity
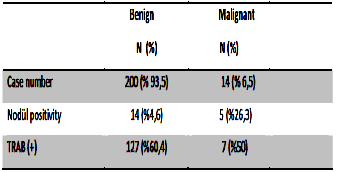
126 - The diagnostic accuracy of ultrasound-guided fine needle aspiration biopsy (FNAB) in thyroid nodules 3 cm and above in size and sonographic feature differences between malignant and benign nodules - 2013
Uluslararası Bildiriler P-1102, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
Introduction: Nodule diameter was considered to be related with thyroid cancer. Whether under ultrasound (US) guidance or not, FNAB has some limitations particularly in big nodules. In this study, we aimed to evaluate diagnostic value of US-FNAB in nodules bigger than 3 cm or more. We also compared ultrasonographical features of benign and malignant nodules.
Material and methods: Data of 267 patients operated for nodulary goiter were screened retrospectively. The study group consisted nodules with a diameter of 3 cm or more. Nodules with a diameter of less than 3 cm were considered as control group. Cytological results were classified as malignant, suspicious for malignancy, undetermined, benign and nondiagnostic.
Results: There were 144 (53.9%) patients in study group and 123 (46.1%) patients in control group. Malignancy was observed in 16% of study group and 42.3% of control group. In nodules smaller than 3 cm, US-FNAB had a sensitivity of 85.4%, specificity of 40.3%, positive predictive value (PPV) of 52.6% and negative predictive value (NPV) of 78.1%. In nodules bigger and equal to 3 cm, sensitivity of US-FNAB was 72.7%, specificity was 81.6%, PPV was 45.7%, and NPV was 93.3%. Among parameters that may be used to predict malignancy, nodule texture, margin regularity, echogenicity and presence of halo were significantly different between malign and benign nodules.
Conclusion: This study showed that increased nodule diameter is not related with limitations in diagnostic value of US-FNAB. We also found that malignancy rate was smaller in big nodules. This finding reflects the importance of true and rational diagnostic and clinical management while detecting malignancy and deciding surgery.
125 - Does a normal thyroid ultrasound image always accompany normal thyroid functions test results? - 2013
Uluslararası Bildiriler P-1055, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Nowadays, ultrasonography (USG) is being used indispensableand commonly in the diagnosis ofthyroid diseases. Heterogeneous appearance of thyroid parenchyma is associated with thyroid autoantibody positivity and hypofunctioning of thyroid gland. On the other hand, it is not determined whether thyroid parenchyma appearing quitelynormal echogenicity on USG is related to presence normal thyroid function tests or otherwise.The objective of our study was to evaluate the relationship between normal thyroid USG appearance and thyroid function tests with thyroid autoantibodies.
MATERIAL AND METHODS: Thyroid USG images of 218 patientsand laboratory tests were evaluated prospectively.The participants were classified into two groups,homogeneous/ normoechogenic and the heterogeneous group, according to thyroid parenchyma appearance on USG.
RESULTS: We acquired homogeneous images on 103 cases and heterogeneous images on 115 cases. Thyroid Stimulating Hormone (TSH)level, Anti-Thyroglobulin (Anti-Tg)and Anti-Thyroid peroxidase (Anti-TPO)titres and thyroid volume was found to be significantly higher in heterogeneous parenchyma group (p<0.001). 83 cases with normal USG images (80.5%) had normal TSH levels and 7 cases in this group had positive Anti-Tg (8.4%) and 23 cases had positive Anti-TPO (27.7%)levels. Out of the heterogeneous parenchyma group composed of 115 cases; 46 patients (40%) had high TSH level and 9 of them (19.6 %) had positive Anti-Tg and 35 (76.1%) had positive Anti-TPOlevels. We observed no differencesbetween the groups regarding tofree triiodothyronine (fT3)and free tetraiodothyronine (fT4)levels. Between age and thyroid volume statistically significant and positive correlation was found (r=0.171, p=0.012).
CONCLUSION: The thyroid gland “normal” appearing on USG imaging, probablyaccompanies normal serum thyroid function tests and negativity for thyroid antibodies.According to our results, thyroid USG is a perfect device for predicting normal thyroid functions, which could probably avoid unnecessary future laboratory tests as well.
Table 1. In USG normal and heterogeneousgroup, distribution of antibody positive cases in which TSH levels are normal
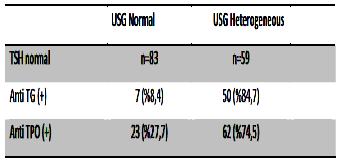
124 - Coexistent toxic adenoma and Riedel thyroiditis: a case report - 2013
Uluslararası Bildiriler P-1032, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
BACKGROUND: Riedel thyroiditis is a rare chronic inflammatory disease of the thyroidgland. It is characterized by replacement of normal parenchyma with dense fibrotic tissue. Peripheral tissues might also be affected and this may cause airway obstruction, dysphagia, recurrent laryngeal nervepalsy and hypoparathyroidism. We report a patient with toxic adenoma previously treated with radioiodineand histopathologically confirmed Riedel thyroditis.
CASE: A 61 years old male patient was referred to our clinic because of subclinical hyperthyroidism. He did not have any obstructive symptoms. In physical examination, a 3x2 cm nodule was detected in the leftthyroid lobe. Serum Thyroid Stimulating Hormone (TSH), free triiodothyronine (fT3), free tetraiodothyronine (fT4)and thyroglubulin(Tg)levels were 0.047 µIU/ml (0.4-4 µIU/ml), 2.04 pg/ml (1.57-4.71 pg/ml), 1.03 ng/dl (0.85-1.78 ng/dl) and 6.31 mg/dl (1.15-35 mg/dl), respectively. Antithyroid peroxidase, antithyroglobulin and thyroid stimulating antibodies were negative. Thyroid ultrasonography revealed a 15x20x28 mm isoechoic nodule located in superior and mid portions of the left thyroid lobe. The ultrasonographic features of the nodule were; a thin hypoechoic halo, cytic degeneration areas and macrocalcification. Thyroid scintigraphy showed an active nodule with extranodular suppression of thyroid parenchyma(Figure 1). Radioiodine uptake measurement was 10% after 4 hours and 25% after 24 hours of I-131 administration. The nodule was evalueated with fine needle aspiration biopsy and cytology was found benign. The patient was treated with 20 mCiradioiodine for toxic adenoma.In the posttreatment follow-up, since nodule diameter is increased significantly after 6 monthsof the radioiodine treatment, total thyroidectomy was performed. In histopathological examination, there was marked fibrosis in stroma and some atrophic glands in thyroid tissue. Fibrosis was extending to the surrounding fat tissue and focal chronic inflammatory cells were observed around middle sized veins. With these findings, the patient was diagnosed to have Riedel thyroiditis.
Figure 1. Active nodule in the left thyroid lobe and extranodular supression of thyroid parenchyma
Figure 2. Marked fibrosis in thyroid parenchyma, lymphoid cells and tightened atrophic thyroid follicules : Riedel thyroiditis (H/E x 50).
CONCLUSION: Riedel thyroiditis is a very rare disease of the thyroid gland. To our knowledge, this is the first case with coexistent toxic adenoma and Riedel thyroditis reported in the literature.
123 - Evaluation of QT dispersion at the time of diagnosis and at the end of follow-up in acromegaly patients - 2013
Uluslararası Bildiriler P-918, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
BACKGROUND: Cardiac rythm abnormalities are important in acromegaly patients and they can be a cause for sudden death. Establishing the clinic determinants of ventricular arrhythmias is important for the risk assesment in those patients. QT dispersion can be used to detect proarrhythmia. Increased QT dispersion is related with increased risk of arrhythmia. In this study we have aimed to calculate the QT dispersion in acromegaly patients and reveal its correlation with growth hormone (GH), insulin like growth factor-1 (IGF-1).
MATERIAL AND METHOD: 41 acromegaly patients were enrolled in the study. Another 41 patients with similar age, sex and comorbid disease distrubition have constituted the control group. We have evaluated the electrocardiograms (ECG) of the acromegaly patients at the time of diagnosis (baseline) and at the end of follow up (post follow up). Only one ECG was provided from each patient in the control group. The longest (QT max), the shortest QT (QT min), QT dispersion, corrected QT max (QTc max), QTc min and QTc dispersion were calculated.
RESULTS: Baseline QT max, QT dispersion, QTc max and QTc dispersion intervals of the acromegaly patients were significantly longer than the control group. There wasn’t any difference between the groups in terms of QT min and QTc min (Table 1). We have detected that post follow up QTc max and QTc dispersion were significantly shorter compared to baseline intervals (p=0.005 and p=0.024, respectively). There wasn’t any significant difference between baseline and post follow up QT max, QT min, QT dispersion and QTc min intervals (Table 2). There wasn’t any significant difference in between the post follow up QT intervals of acromegaly patients and the control group (Table 3). We have evaluated the relation of QT intervals with GH and IGF-1 in each group. Except the correlation of GH with QTc dispersion in post follow up acromegaly patients (r=-0.438, p=0.011), we could not show any other relation between GH, IGF-1 and the other QT parameters (for all parameters, p>0.05). QT intervals have not been found to be associated with age and BMI of the individuals (for all parameters, p>0.05). We have detected a significant positive correlation between disease duration and QTc dispersion in acromegaly patients (r= 0.440, p=0.009).
CONCLUSION: According to the findings of this study we can claim that QT intervals are beneficial in determining the arrhythmia risk in acromegaly patients and this risk can be reduced after treatment and hormonal control..
Table 1. Comparision of the baseline QT intervals of the acromegaly patients with the control group
Acromegaly (baseline) (n=41) | Control (n=41) | p | |
QT max (ms) | 387.73 ± 25.30 | 373.73 ± 26.33 | 0.016 |
QT min (ms) | 317.88 ± 22.55 | 312.46 ± 23.09 | 0.286 |
QT dispersion (ms) | 70.10 ± 10.51 | 61.76 ± 12.18 | 0.001 |
QTc max (ms) | 422.76 ± 20.82 | 408.27 ± 17.08 | 0.001 |
QTc min (ms) | 345.59 ± 17.36 | 339.51 ± 13.34 | 0.080 |
QT c dispersion (ms) | 77.07 ± 12.34 | 68.02 ± 13.13 | 0.002 |
Table 2. Comparision of baseline and post follow up QT intervals of the acromegaly patients
Baseline (n=35) | Post follow up (n=35) | p | |
QT max (ms) | 391.42 ± 24.50 | 383.20 ± 15.22 | 0.128 |
QT min (ms) | 320.88 ± 20.05 | 317.42 ± 13.55 | 0.430 |
QT dispersion (ms) | 70.82 ± 9.94 | 65.77 ± 10.59 | 0.054 |
QTc max (ms) | 422.85 ± 20.88 | 410.23 ± 15.33 | 0.005 |
QTc min (ms) | 344.88 ± 18.28 | 337.86 ± 13.64 | 0.051 |
QT c dispersion (ms) | 77.85 ± 10.83 | 71.51 ± 9.83 | 0.024 |
Table 3. Comparision of post follow up QT intervals of the acromegaly group with the control
Acromegaly- post follow up (n=35) | Control (n=41) | p | |
QT max (ms) | 383.20 ± 15.22 | 373.73 ± 26.33 | 0.055 |
QT min (ms) | 317.42 ± 13.55 | 312.46 ± 23.09 | 0.249 |
QT dispersion (ms) | 65.77 ± 10.59 | 61.76 ± 12.18 | 0.133 |
QTc max (ms) | 410.23 ± 15.33 | 408.27 ± 17.08 | 0.603 |
QTc min (ms) | 337.86 ± 13.64 | 339.51 ± 13.34 | 0.595 |
QTc dispersion (ms) | 71.51 ± 9.83 | 68.02 ± 13.13 | 0.200 |
122 - A case of type 1 diabetes represented by diabetic ketoacidosis after isotretinoin therapy: is it a result or coincidence? - 2013
Uluslararası Bildiriler P-327, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Well-known environmental factors,which can lead to type 1 diabetes,are viral infections, vaccines, diet, exposure to cow milk in infancy, vitamin D deficiency, drugs, maternal age, preeclampsia and low birth weight, Isotretinoin is an effective drug for acne treatment. It can cause dyslipidemia, elevated liver enzymes, insulin resistance and type 2 diabetes. Our case is type 1 diabetes developed after the use of isotretinoin and represented with diabetic ketoacidosis.
CASE: 18 years-old-male patient has admitted to hospital with complaints of abdominal pain, increased sense of thirst, frequent urination and dry mouth. In physical examination, he was dehydrated with hypotension and dry oral mucosa. He didn’t have family history of diabetes. With further questioning, we have learnt that he was using isotretinoin for acne treatment for seven months. In laboratory examination, his plasma glucose level was 400 mg/dl,and there was heavy ketonuria and acidosis in arterial blood gas. He was hospitalized in endocrinology ward with diagnosis of diabetic ketoacidosis. Hydration with isotonic saline together with insulin infusion, potassium replacement and dextrose infusion were given to the patient. His anti GAD was positive and C-peptid level was very low leading to diagnosis of type 1 diabetes. After amelioration of ketoacidosis, we have skipped intensive insulin therapy and blood glucose levels were regulated.
CONCLUSION: Isotretinoin is related with metabolic syndrome and type 2 diabetes. However, there are few cases of type 1 diabetes in literature. Anti GAD positivity is suggestive of underlying autoimmune mechanisms triggered by the drug. Patients should be monitoredwith frequent glucose measurements during follow up.
Table 1. Labaratory results at the time of diagnosis
Laboratory Results | Reference Range | |
Glucose | 400 | 74-106mg/dl |
Urine ketone | +++ | Qualitative |
Na | 133 | 135-145mmol/lt |
K | 3.3 | 3,5-5,1mmol/lt |
PO4 | 2,5 | 2,5-4,5mg/dl |
Ca | 8,5 | 8,5-10,2mg/dl |
Cr | 1,3 | 0,5-1,2mg/dl |
ALT | 16 | 0-33 u/l |
Hb | 12,6 | 12-16gr/dl |
Wbc | 20000 | 4000-10000 K/ul |
CRP | 4,8 | 0-0,8 mg/dl |
Arterial PH | PH:6,9 | 7,35-7,45 |
pCO2 | 30 | 35-45mmHg |
HCO3 | 10 | 22-26 mEq/L |
121 - Cyclosporine induced autoimmune thyroid disease: presentation of two cases - 2013
Uluslararası Bildiriler P-317, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Immune supressive patients due to any cause(disease, medication etc.) rarely have autoimmune diseases. In this presentation two patients diagnosed with Graves' disease and subacute thyroiditis while taking cyclosporine therapy will be discussed.
CASE 1: A 47 year-old female patient applied to outpatient clinic with weight loss, sweating and tremor which had been present for the last two months. She had been on cyclosporine therapy for three years because of hypoplastic anemia. Laboratory tests are listed in table 1. Thyroid ultrasound revealed enlarged thyroid gland with diffuse parenchymal heterogeneity. Patient's thyroid scan showedincreased uptake which was diffuse and homogenous in pattern.(Picture 1). On 24-hour radioiodine uptake test 4th hour uptake was 46 % (15-25 %) and 24th hour uptake was 27 % (25-35 %). Based on these clinical and laboratory findings the patient was diagnosed as Graves’ disease. With thyromazol therapy euthyroid state was achieved.
Normal values | Case 1 | Case 2 | |
TSH | 0.27-4.2 uIU/ml | 0,01 | 0,015 |
fT3 | 1.8-4.6 pg/ml | 28,56 | 3,92 |
fT4 | 0.9-1.7 ng/dl | 7,77 | 1,48 |
Anti-Tg | 0 - 115 IU/mL | 387,8 | 143,2 |
Anti-TPO | 0 - 34 IU/mL | 35,2 | 9,7 |
TSH Reseptor Antibody | 0 - 14 u/L | 95,02 | 5 |
RAI Uptake | 4.hour%15-25 | 46 | 1 |
24.hour %25-35 | 27 | 0 |
CASE 2: A 41 year-old female patient admitted to our clinic with pain and tenderness in the thyroid area. She had been using cyclosporine during the last 2 year period for psoriases. Laboratory tests are listed in table 1. Thyroid ultrasonography showed multiple hypoechoic thyroid nodules with ill-defined margins on the basis of chronic thyroiditis. In the thyroid scan there were supressed areas in nodular pattern and a global nonhomogenous uptake. There was low radioiodine uptake in the 24-hour radioiodine uptake test.(Picture 2). The patient was diagnosed as subacute thyroiditis. Nonsteroidal anti inflamatory drug and beta bloker were given. One month later her thyroid function tests were within normal limits..
CONCLUSION: Cyclosporine is an immune-supressive drug which is also used in the treatment of Graves’ ophthalmopathy. Cyclosporine inhibits calcium, IL-3, IL-4 and IL-5 induced T and B lymphocyte proliferation and cytotoxic T cell egzocytosis but rarely it can be a cause of autoimmune disease by an unknown mechanism of abnormal modulation of the immune system. Patients taking cyclosporine especially those having another autoimmune disease or family history of thyroid disease must be carefully monitorized with thyroid function tests.
Picture 1 Picture 2
120 - Mixed medullary-follicular carsinoma of the thyroid: two case reports - 2013
Uluslararası Bildiriler P-316, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Mixed medullary-follicular carcinomas (MMFC) of the thyroid are rare tumors which represents less than 0.15% of all thyroid tumors showing the morphological and immunochemical properties of both parafollicular and follicular cell lineages. Cases were immunoreactive for both calcitonin and thyroglobulin. However, there are discussions in the literature related to histopathological characteristics and originof MMFC. In this paper, we aimed to present our two cases of MMFTK.
CASE 1: A 25-year-old female patient referred us for evaluation of a thyroid mass located on the left lobe. Ultrasonography(US) revealed 38 mm solid isoechoic nodule with well-defined margins on the left lobe. An US-guided fine needle aspiration(FNA) was performed and reported as follicular neoplasm. A total thyroidectomy with central lymph node dissection was performed.Immunostaining revealed that the tumor cells were diffusely positive for calcitonin and chromogranin. Further, there were scattered follicules that stained positively with antibody against thyroglobulin.The histological findings in correlation with the immunoprofile, support a diagnosis of MMFC.Post-operatively calcitonin level was 2.69 pg/ml.Radioactive iodine ablation with 150 mCi and levo-thyroxine supression theraphy had given to the patient.
CASE 2: A 46-year-old female patient admitted with enlargement of a neck mass. US revealed 33 mm solid isoechoic nodule with ill-defined margins and microcalcifications on the left lobe of thyroid.US-guided FNA was reported as thyroid neoplasm with differentiation or anaplastic transformation. Patient’s serum level of calcitonin was 1802 pg/ml (normal <12 pg/ml). Results of blood testing for pheochromocytoma and hyperparathyroidism were within the normal range.Total thyroidectomy with central lymph node dissection was performed. The histological findings were consistent with MMFC with metastatic lymph nodes.The serum calcitonin level dropped to 3,75 pg/ml following the surgery.
FİGURE 1. Histopathologic appearance of case 1
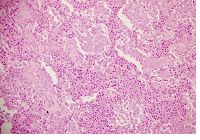
FİGURE 2. Histopathologic appearance of case 2
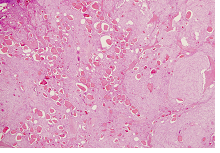
CONCLUSION: The majority of MMFC occurs in a sporadic form, rarely it can be a component of MEN type 2. MMFC,medullary and follicular thyroid cancer behave differently in terms of clinical course and management. Identification of MMFC by FNA may be difficult, the proper immunostaining panel could have showed the different aspects of the mixed tumor.
119 - Primary octreotide therapy in a patient with pituitary adenoma cosecreting GH and TSH - 2013
Uluslararası Bildiriler P-313, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Pituitary adenomas which co-secrete growth hormone(GH) and thyroid stimulating hormone(TSH) accounts for less than 0.2% of all adenomas of the pituitary. Symptoms of hypertyroidism are usually masked by clinical manifestations of acromegaly. Here we have reported the result of the primary one-year-long medical therapy in a case who was diagnosed to have adenoma co-secreting GH and TSH.
CASE: 70-years-old female patient has admittedto hospital with the complaints of excessive sweating, enlargement of hands and feet. In physical examination there were frontal bossing, coarsening of facial structures and acral enlargement. In hormone tests, GH level was : 17 ng/mL and IGF-1 level was : 607 ng/ml (64-188 ng/mL).GH levels were not suppressed during glucose suppression test. Her serum TSH, fT4 and fT3 levels were elevated. Serum alpha subunit was also high (80 IU/l). In thyroid ultrasonography, we have detected goiter. In thyroid scintigraphy, homogenous diffuse hyperplasia of both lobes was reported. In pituitary MRI,there wasa 13x16 mm sized macroadenoma on the left handside of the pitiutary gland. The diagnosis of acromegaly was made with high suspicion of TSH co-secretion from the adenoma. Since the patient had dilated cardiomyopathy and obstructive sleep apnea syndrome, the operation could not be done. Octreotide LAR was started in a dosage of 30 mg/28 days. The patient was evaluated at the first year of the therapy. IGF-1 level decreased (285 ng/ml) and the size of the adenoma was reduced(11x10 mm). Serum fT4, fT3 and TSH levels were normal together with normalization of serum alpha subunit.
CONCLUSION: Coexistence of GH secreting adenoma and TSHoma is rareIn such cases, transsphenoidal surgery must be the first choice for therapy. However when operation is contraindicated as it occurred in our case or when the lesion cannot be excised completely resulting in residual mass, somatostatin anolnalogues should be used. Sandostatin LAR is the one which the clinicans have the most experience in TSHomas.
Picture 1. 13x16 mm sized adenoma on the left handside of the pitiutary gland
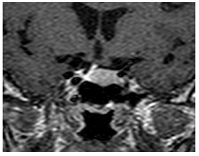
Table 1. Laboratory results of the patient at the time of diagnosis
Laboratory Results | Reference Range | |
Free T3 | 5.1 pg/mL | 2,3-4.2 |
Free T4 | 1.8 pg/mL | 0,74-1,52 |
TSH | 2 uIU/mL | 0,35-5,50 |
GH | 17 ng/mL | 0-8 |
IGF1 | 607 ng/mL | 61-186 |
PRL | 9,5 ng/ml | 2,8-29 |
FSH | 40mIU/ml | 2,5-10,2 |
LH | 15mIU/ml | 1,9-12,5 |
Estradiol | 48 pg/ml | 0-160 |
ACTH | 15 pg/ml | 0-46 |
Cortisol | 12ug/ml | 5-20 |
Alpha subunit | 80 IU/L | 0-1.6 |
118 - Primary hyperparathyroidism associated with atrial septal defect, interatrial septal aneurisym and skeletal anomaly: a case report - 2013
Uluslararası Bildiriler P-297, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
BACKGROUND: The classic clinic manifestation of primary hyperparathyroidism(PHPT) is osteitis fibrosa cystica, a severe skeletal disease characterized by brown tumors, bone cysts and deformities, due to extremely elevated bone resorption elicited by continuously high parathyroid hormone (PTH) levels. In cardiovascular system there may be shortened QT interval, deposition of calcium in heart valves, coronary arteries, and myocardial fibers. Here, we report a case with PHPT, who have anorexia nervosa, sceletal anomaly, atrial septal defect(ASD) and interatrial septal aneurysm.
CASE: An 18-year-old woman, who has anorexia nervosa has applied for constipation.She had bradycardia, low weight(Body mass index:15 kg/m2), and prognathism. The radiographic finding of the extremities showed that, bilaterally 2 and 5 metacarpals ofthe hands , and bilaterally 1, 3, 4, 5 metatarsals ofthe foots were short. Laboratory tests revealed hypercalcemia, hypophosphatemia and hyperparathyroidism. 24-hour urinary calcium was 504 mg/day. The neck ultrasound revealed a 4.9x6.8x10.4 mm hypoechoic lesion in the outsideofthe thyroid right lobe inferior. Sestamibi scintigraphy results were consistent with parathyroid adenoma. Renal ultrasonography determined milimetric crystaloids in the right kidney. Bone mineral densitometry revealed osteopenia. Her electrocardiography showed shortened QT interval and bradycardia. Echocardiography revealed an ASD and interatrial septal aneurysm. Her pituitary hormonal levels were consistent with panhypopituitarism. She had also evaluated for the eye, ear and nose anomaly, but no pathology was found. After the diagnosis and emergency treatment for hypercalcemia she had underwent parathyroidectomy.Histopathology was consistent with parathyroid adenoma.Postoperative her calcium and parathyroid levels were reduced in normal levels.
CONCLUSION: Our case revealed hypercalcemia and hyperparathyroidism and also unusual manifestations like anorexia nervosa, ASD, interatrial septal aneurysm and sceletal anomaly. In the literature to our knowledge, there is only one case with PHPT and ASD associated with mongoloid features. In conclusion, the patients with PHPT may be evaluated for atypical manifestations of cardiac and sceletal system.
Picture 1. MIBI scan of the patient
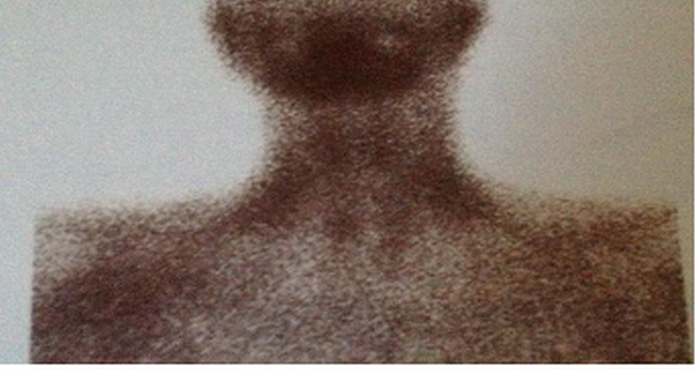
Picture 2. A. Hand X-ray of the petient B. Food X-ray of the patient


A. B.
117 - Giant cell granuloma as initial presentation of primary hyperparathyroidism: a case report - 2013
Uluslararası Bildiriler P-279, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Giant cell granuloma is a skeletal manifestation seen now rarely in hyperparathyroidism due to early recognition of the disease. Lesions usually occur in the areas of intense bone resorption. They can affect mandible, maxilla, clavicle, ribs and pelvic bones. Most of the patients who have primary hyperparathyroidism are asymptomatic and are discovered incidentally during laboratory examinations. Here we represent a female patient who was referred to endocrinology clinics because of maxillary brown tumor detected by her dentist.
CASE: 30-years-old female patient has admitted to dental clinics with the complaint of oral mass and accompanying symptoms as decreased apetite, weight loss and numbness on the jaw. Biopsy of the oral lesion was consistent with giant cell granuloma. Radiographic imaging has revealed multiple bone cysts on the mandible and maxillary bones. In laboratory exam, severe hypercalcemia and hypophosphatemia were detected. Her serum parathormon level and urinary calcium level were elevated. In ultrasonographic examination, we have detected two parathyroid adenomas on left side and MIBI scan was positive. In bone mineral densitometry, osteoporosis was detected at the lumbar vertebrates. She didn’t have any renal stones in abdominal ultrasonography. We have searched for MEN1 syndrome. There was a microadenoma in pituitary MRI that was provento be nonfunctional with hormone tests. Her upper gastro intestinal endoscopy was normal as the serum gastrin levels. She underwent surgery and all parathyroid glands and thymus were excised then ½ of a paratyhroid gland was seeded on forearm. No complications occurred during or after surgery and she was discharged and referred to her dentist for curettage of the bone cysts.
CONCLUSION: Treatment of hyperparathyroidism is surgery. However, treatment for bone lesions is controversial. They can regress after removal of the adenoma. In the persistent cases, surgical removal of the bone lesion after a short course of steroid therapy is advised.
Picture 1. Bone cysts on mandibula

Picture2. MIBI scan of the patient
116 - Malignancy rate of thyroid nodules, which defined as follicular lesion of undetermined significance and atypia of undetermined significance in thyroid cytopathology and relation with ultrasonographic features - 2013
Uluslararası Bildiriler P-271, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
BACKGROUND: Fine needle aspiration cytology (FNAC) has been widely accepted as the most accurate, safe and cost-effective method for the evaluation of thyroid nodules. The most challenging category in the FNAC is atypia of undetermined significance (AUS) and follicular lesion of undetermined significance (FLUS). Bethesda System (BS) recommends repeat FNAC in that category due to their low risk of malignancy.In our study; we aimed to investigate the malignancy rate of thyroid nodules of AUS and FLUS and to evaluate the presence of biochemical, clinical and echographic features possibly predictive of malignancy related to AUS and FLUS.
MATERIALS AND METHODS: Data of 268 patients operated for AUS and FLUS cytology were screened retrospectively. Ultrasonographic features and thyroid function tests, thyroid antibodies, scintigraphy and histopathological results were evaluated.
RESULTS: 276 nodules of 268 patient’s results are evaluated. Malignancy rates were 24.3% in the AUS group, 19.8% in the FLUS group and 22.8% in both group. In the evaluation of all nodules the predictive features of malignancy arehypoechogenicity and peripheral vascularization of the nodule. In the AUS group, the predictive feature of the malignancy isonly hypoechogenicity, and peripheral vascularization in the FLUS group.
CONCLUSION: We determined that the malignancy rates in these nodules are higher than the anticipated literature rate. This high ratio may be due to the fact that we studied only the patients who underwent surgery. The ultrasonographic features alone may be insufficient to predict the malignancy, therefore all the clinical and ultrasonographic features must be considered in the evaluation of the thyroid nodules. In addition, we think that, the recommended management of repeat FNAC in these groups must be reconsidered with the clinical and ultrasonographic features.
Table. Ultrasonograpfic features of benign and malignant thyroid nodules
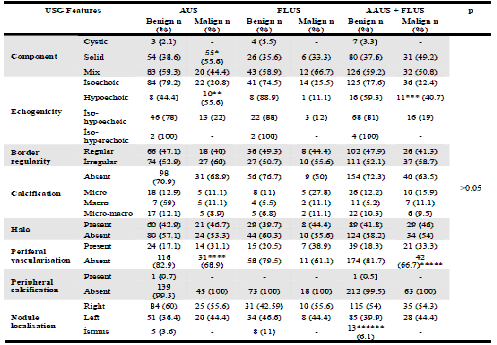
*p: 0.045, **p: 0.003, ***p:0.02, ****p: 0.04, *****p: 0.011, ******p: 0.044
115 - Differential diagnosis of an incidental pituitary lesion detected with PET-CT in a patient with a known history of metastatic maxillary sinus tumor - 2013
Uluslararası Bildiriler P-265, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
BACKGROUND: Metastatic pituitary tumors are seen rarely and it is hard to differentiate them from the benign lesions of the gland. We have reported a case, with a known maxillary tumor, detected to have a pituitary lesion coincidentally on PET-CT.
CASE: 45 years old male patient with a known history of relapsed maxillary sinus tumor has been referred to our clinics because of thehypophyseal lesion detected to have increased FDG involvement on PET-CT examination. It is learned from the medical history that he was operated for the maxillary sinus tumor 35 years ago and had the second operation last year because of the recurrent disease. Histopathological examination of the lesion was reported as well-differentiated squamous cell carcinoma with perineural and lymphovascular invasion. He received 6 cycles of chemotherapy, conventional external radiotherapy and 66 Gys of tomotherapy(maximum of 30 Gys to the pituitary gland). There was a tissue defect on the right maxillary region, nose and the right eye lid in physical examination. Pitiutary lesion was metabolically active on PET-CT and SUV max value was 11.7(Fig.1). There was also left lung involvement (SUV max: 4.3) compatible with metastasis. We have demanded a pitiutary MRIand detected a 5.4x4.3 mm sized nodular pitiutary lesion on the right side of the gland which was isointense on T1A and T2A images and with late contrast concentration on dynamic sequences. In the labaratory examination GH was0,09 ng/ml, IGF1 was 239 ng/ml, prolactin was 57.6 ng/ml, TSH was 1.9 uIU/ml, FSH was 18.4 mIU/ml, LH was 4.6 mIU/ml, ACTH was 52 pg/ml, cortisol was 15.7 μg/dl. There wasn’t any symptom or sign of diabetes insipitus. The PET-CT control, made one month after radiotherapy, has revealed that the pituitary lesion was less metabolically active after RT (SUV max: 7.1).
Fig 1. İncreased metabolic activity in pituitary on PET-CT
CONCLUSION: It is difficultto differentiate metastatic lesions from the benign lesions of the pituitary gland. Most of the metastatic lesions are asymptomatic although presence of diabetes insipitus or ophtalmoplegia are suspiciousfor metastasis in patients with a known history of a malign tumor. Although there isn’t any specific radiologic sign for metastatic lesions, increased thickness of pituitary stalk, diminished signal intensity of posterior pituitary, isointense appearance on T1 and T2 images, cavernous sinus invasion and sclerotic changes in cella turcica should make the clinician consider presence of a metastatic lesion within the gland. In our case because of the lesion being metabolically active on PET-CT with a high SUV max value, isointense appearance on MRI and a history of previous maxillary sinus malignancy made us suspect pituitary metastasis. However absence of pituitary insufficiency, diabetes insipitus or ophthalmoplegia and decreased metabolic activity (SUV max) on control PET-CT might indicate that the lesion might be benign. Tissue biopsy for the definitive diagnosis could not be performed because of the facial defect of the patient.
114 - Ectopic ACTH dependent Cushing syndrome diagnosed with octreotide scan - 2013
Uluslararası Bildiriler P-245, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
INTRODUCTION: Cushing's syndrome may be either corticotropin (ACTH)-dependent or -independent. Ectopic secretion of ACTH by nonpituitary tumors accounts for 10 to 15 percent of ACTH dependent Cushing syndromes. Generally it is difficult to localize the ACTH secreting tumor by conventional imaging methods because these tumors are often small in size. Neuroendocrine tumor cells exhibit somatostatin receptors on their cell surfaces. By using this feature 111-In-octreotide scan is an alternative diagnosing method. Here we present a case of ectopic ACTH syndrome diagnosed with octreotide scan.
CASE PRESENTATION: A 26 year old male patient presented with moon face, purplish striae, supraclavicular fat pads and proximal muscle weakness. Laboratory tests were as follows:
Normal values | Patient results | |
Sodium | 136 - 145 mmol/L | 144 |
Potassium | 3,5 - 5,1 mmol/L | 2,4 |
06:00 cortisol | μg /dL | 33 |
23:00 cortisol | μg /dL | 39 |
24 hour urinary free ccrtisol | 0.0 - 60 µgr/gün | 258 |
Cortisol after 1 mg Dexamethasone supression test | <1,8 μg /dL | 31,2 |
Cortisol after 2 day 8 mg Dexamethasone supression test | <1,8 μg /dL | 30,6 |
ACTH | 0 - 60 pg/mL | 92 |
Pituitary magnetic resonance imaging (MRI) revealed no mass. Inferior petrosal sinus sampling was negative with no increase in ACTH after CRH administration. On thorax computerized tomography (CT) there was a 14 mm nodule in the middle lobe of the right lung. The patient was a heavy smoker. There was no pathology on 18-FDG positron emission tomography scan. But 111-In -Octreotide scan depicted the neuroendocrine tumor located in the right lung.
Following surgey there was no need for antihypertensive treatment or insulin therapy any more and hypokalemia did not recurr.
CONCLUSION: The last step of approaching to a patient with ACTH dependent Cushing Syndrome is to detect the source of ACTH secretion. As most of the ACTH secreting tumors arise from thorax it is important to start evaluation from this anatomic localisation. CT or MRI is the first imaging modality of choise. The sensitivity of CT to detect a small tumor such this is 53 % whereas it is 37 % in MRI. The senstivity of octreotide scan in detecting ACTH secreting tumor is approximately 30-53 %. It is the last but not least choise of non invasive procedure on the way going to surgery as in our case.
113 - Differential diagnosis of aggresive macroprolactinoma, adenoma or atypical adenoma: a case report. - 2013
Uluslararası Bildiriler P-231, 15th European Congress of Endocrinology, 27 April - 1 May 2013, Copenhagen, Denmark, Endocrine Abstracts April 2013 Volume 32, ISSN 1479-6848
ABSTRACT
BACKGROUND: Atypical tumors were identified in 15% of pituitary adenomas, and they tended to be aggressive, invasive macroadenomas. World Health organization (WHO)classification of atypical pituitary adenomas include; Ki-67 proliferative index greater than 3%, excessive p53 immunoreactivity, and ≥ 2 mitotic figures per 10 high-powered fields. Pituitary carcinomas are extremely rare tumors with cerebrospinal or extracranial metastasis.
CASE: A 31 years old man with symptoms of stuffy nose and snore, presented to our policlinic due to the solid lesion on paranasal sinus tomography. Tomography showed a soft tissue lesion with 38 Haunsfield Unit (HU). Pituitary imaging revealed a mass, which lead to destruction of bone structures, suppression of optic chiasm, extending to suprasellar cistern and right nasal cavity. Except increased prolactin (470 ng/ml),hormonal levels were in normal ranges. Also macroprolactin was negative. Nasal punch biopsy showed an atypical pituitary adenoma with atypical and 8 mitotic figures in the 10 high-powered fields. Ki-67 labeling index 2-3%, p53 immunoreactivity was 1%. 18-Fluoro-Deoxy-Glucose Positron Emission Tomography determined increased activity in this lesion with 6.4 SUV-max. No distant metastasis was determined. Cabergolin 0.5 mg/ twice a week was begun and then he underwent to operation. Histopathological result was a pituitary adenoma with diffuse staining PRL. Ki-67 index was 1%, whereas p53 immunoreactivity was 10%. Postoperative prolactinlevel reduced to 65 ng/ml and no solid lesion was seen in postoperative imagining. His medical treatment is now ongoing.
CONCLUSION: Because of the atypical and ≥2 mitotic activity, necrosis in the nasal punch biopsy, also 38 HU solid lesion in tomography and absent of distant metastasis, we thought primarily atypical adenoma in this case. Although histopathological result is consistent with benign prolactinoma, it must be considered that its biological behavior may be progressed to malignancy after several years.
Table 1. Laboratory parameters of the patient before and after operation
Parameter | Referance | Preop | Postop (1.Month) |
GH | 0 - 5 ng/mL | 1 | 0,03 |
IGF- I | 115-307 ng/mL | 150 | 239 |
PRL | 4.6-21.4 ng/mL | 470 | 65.79 |
Macro PRL | Negative | - | |
TSH | 0.27-4.2 uIU/mL | 2.5 | 1.21 |
FSH | 1.5-12.4 mIU/mL | 1.71 | 1.87 |
LH | 1.7-8.6 mIU/mL | 2.4 | 1.46 |
Cortisol | 6.2-19.4 ug/dL | 17.2 | 9.5 |
ACTH | 0-46 pg/mL | - | 5.6 |
Total Testosterone | 2.84-8 ng/mL | 3.6 | 1.94 |
Picture 1. Pituitary imaging of the patient before and after operation
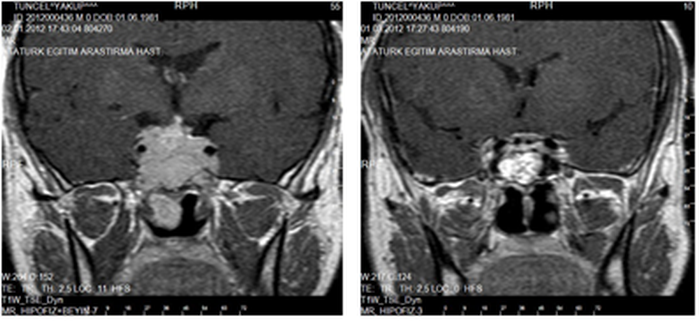
Picture 2. A: Atypical mitotic figure of the lesion on histopathological specimen B: Diffuse staining with PRL
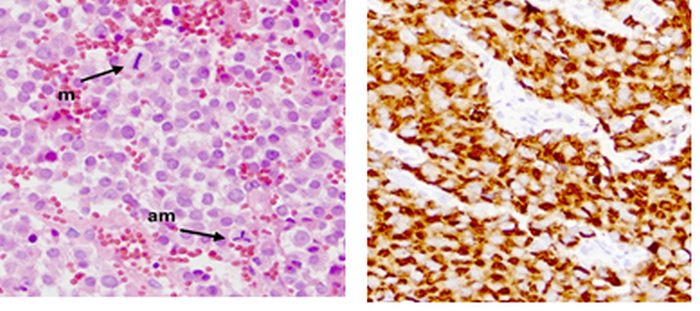
112 - Primary thyroid lymphoma diagnosed during pregnancy: report of a case - 2012
Uluslararası Bildiriler P-1846, 15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
INTRODUCTION: Primary thyroid lymphoma is a rare tumor which represents 1-5% of all thyroid malignancies, and 1-2.5% of all lymphomas. Prompt recognition is important because the management of this potentially curable disease is different from the treatment of other neoplasms of the thyroid gland. Cancer complicates between 0.02 and 0.1% of all pregnancies. Thyroid lymphoma is very rarely encountered during pregnancy and there are only a few case reports in the modern literature. Here we present a case of thyroid lymphoma in a young pregnant woman and review the pertinent literature.
CASE: A 28-year-old female patient presented with a neck swelling, pain and respiratory distress while she was in the 17th week of her first pregnancy. Ultrasonographic and elastosonographic images of left thyroid lobe wasshown in Figure 1. Subtotal thyroidectomy was performed and combined histological and immunohistochemical analyses led to the diagnosis of diffuse large B cell lymphoma with a high proliferation index (Ki-67: 80%) and positive CD20 (Figure2 and3), CD10 and BCL6. Chemotherapy (cyclophosphamide, doxorubicin, vincristine and prednisone (CHOP), 6 cycles every 4 weeks) was planned and the patient underwent the first 4 cycles without vincristine. Twenty weeks after the initiation of chemotherapy she had cesarean delivery of a healthy, full-term male infant. Four additional courses of chemotherapy were administered, after which the patient was reevaluated. She had no complaints and a total body CT did not show relapse of the disease.
Figure 1. Ultrasonographic and elastosonographic images of left thyroid lobe
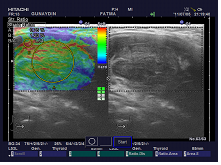
Figure 2.Immunohystochemical examination with Ki67
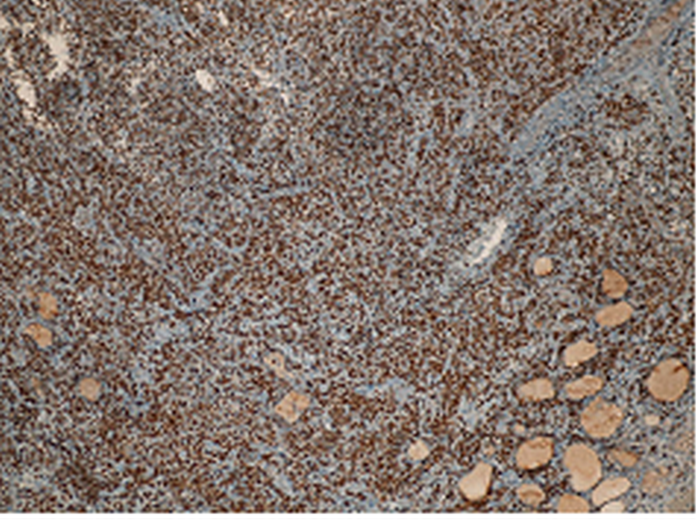
Figure 3.Immunohystochemical examination with CD 20
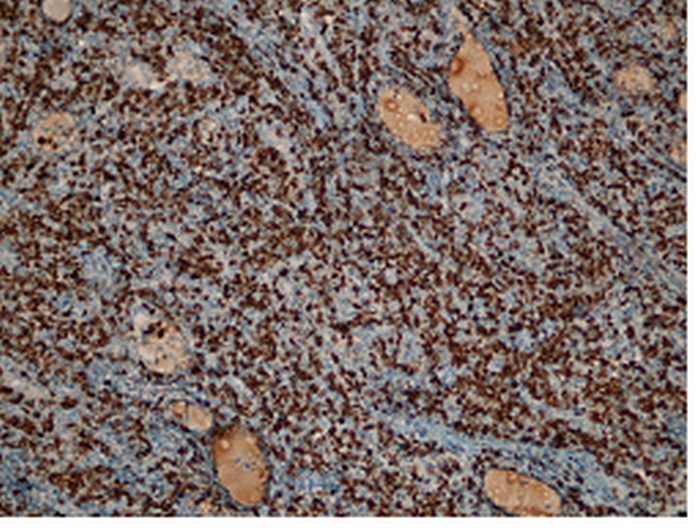
DISCUSSION: Thyroid lymphoma occurs primarily in middle-aged to older aged females. Diffuse large B cell lenfoma is the most frequent histologic subtype of thyroid lymphomas. Patients with primary thyroid lymphoma usually present with compressive symptoms such as dyspnea, dysphagia and hoarseness. The co-existence of thyroid lymphoma and pregnancy is a rare condition. The unusuality of this condition becomes more clear when it is considered that only approximately 100 cases of non-Hodgkin lymphoma in pregnancy have been reported so far. If diagnosed during early pregnancy, the pregnancy should be terminated and chemotherapy started immediately. In advanced pregnancy, chemotherapy should be started as early as possible. In conclusion our case is a one of the few examples of thyroid lymphoma associated with pregnancy and it was successfully managed with a combination of surgery and chemotherapy.
111 - Malıgnancy rate of thyroıd nodules whıch defıned as atypıa of undetermıded sıgnıfıcance ın the thyroıd cytopathology - 2012
Uluslararası Bildiriler P 1841-15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
AIM: According the Bethesda classification for reporting thyroid fine-neddle aspirations (FNAs), atypia of undetermined significance (AUS) is a category with limited reported follow-up and outcome data. True malignancy rate in AUS is not definitely known, because not all of them are histologically checked and also litherature reports have heterogeneous data. Therefore, this classification is grey zone for clinicians who struggle the correct therapeutic approach to thyroid nodules. In this study, our aim was to evaluate the ultrasonographic features and histopathologic results of the thyroid nodules which are defined as AUS and contribute to the therapeutic approach of these nodules.
METHODS: We evaluated 95 nodules of 92 patients, who have nodular or multinodular goiter and had diagnosed AUS at least in one nodule with fine-neddle aspiration (FNA). Patients’ thyroid function tests, ultrasonographic features of the nodules and histopathologic results were evaluated.
RESULTS: 81.1 % of patients were female, 18.9 % were male. Mean age was 47.5 ± 12.1 years. In the ultrasonographic features presence of microcalcification, border irregülarity, peripheral vascularisation and absence of hypoechoic halo was respectively 28.4 %, 47.4 %, 20 % and 60 %. 43.2 % nodules were hypoechoic and 47.4 % were solid. According to the histopathology, 63.2 % of nodules (n=60) were benign, 36.8 % (n=35) were malign. In malign nodules papiller carcinom, well-differentiated thyroid neoplasm, follicular carcinom and hurthle cell carcinom were found respectively 88.6 %, 5.7 %, 2.9 %, 2.9 %. In malign nodules mean tumour size was 1.2 ± 1.1 cm. No lymph node methastasis was found. Vascular invasion, capsular invasion, extracapsular invasion and multicentrity was positive respectively; 11.4 %, 28.6 %, 20 %, 31.4 %. According to the malign or benign histopathologic features of nodules were shown in table 1.
Table 1. Histopathologic Features of Benign and Malign Nodules
BENIGN n=44 | MALIGN n=20 | p | ||
Nodule Component % | Solid | 48,3 | 45,7 | 0,909 |
Cystic | 1,7 | 2,9 | ||
Mix | 50 | 51,4 | ||
Echogenity % | İsoechoic | 85,3 | 51,4 | 0,370 |
Hypoechoic | 41,7 | 45,7 | ||
Hyperechoic | 0 | 2,9 | ||
Hypoechoic Halo % | Positive | 36,7 | 45,7 | 0,385 |
Negative | 63,3 | 54,3 | ||
Microcalcification % | Positive | 28,3 | 28,6 | 0,980 |
Negative | 71,7 | 71,4 | ||
Macrocalcification % | Positive | 16,7 | 20 | 0,683 |
Negative | 83,3 | 80 | ||
Border İrregülarity % | Positive | 51,7 | 40 | 0,272 |
Negative | 48,3 | 60 |
CONCLUSION: In AUS, maligancy rate is reported 25 % of operated patients, but it is thought 5-10 % of the total. In our study we found this ratio 36.8 %. Our high ratio may be due to few and heterogeneous litherature data outcomes. So, this high malignancy ratio in AUS nodules, have to be considered in the decision of operation .
110 - Malignancy rate of thyroid nodules which defined as follicular lesion of undetermined significance ın thyroid cytopathology - 2012
Uluslararası Bildiriler P 1834-15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
AIM: In the Bethesda Classification (BC), which is used in cytopathologic evaluation of thyroid nodules, follicular lesion of undetermined significance (FLUS) does not involve sufficient cellular atypia for follicular neoplasia or malignancy, while it doesn’t comprise the cytologic benign criteria. Therefore, there is no consensus for those nodules to follow-up and therapeutic approaches. In this study, we aimed to determine the ultrasonographic features and histopathologic results of the thyroid nodules which are defined FLUS in BC.
METHODS: We evaluated 64 nodules of 62 patients, who have nodular or multinodular goiter and had diagnosed FLUS at least in one nodule with fine-neddle aspiration (FNA). Operation endication was decided upon to the nodule size, suspected ultrasonographic feature (border irregularity, solid, hypoechoic nodule, presence of microcalcification), high elastosonographic score and strain index and family history of thyroid cancer.
RESULTS: 87.5 % of patients were female, 12.5 % were male. Mean age was 46.5 ±12.6 years. 51.6 % of nodules were located in the right lobe, 45.3 % in the left lobe and 3.1 % were in the istmus. According to the echogenity and component 43.8 % of nodules were hypoechoic, 57.8 % were solid. Microcalcification, peripheral vascularisation and border irregularity positivity were respectively; 25.5 %, 17.2 % and 59.4 % of nodules. After operation, 68.7 of nodules (n = 44) were benign, 31.3 % (n = 20) were malign. In malign nodules mean tumour size was 1.4 ± 1.3 cm. Vascular invasion, capsular invasion, extracapsular invasion, multicentrity and lymph node metastasis was positive respectively; 15 %, 15 %, 5 %, 35 %, 5 %. According to the malign or benign histopathologic features of nodules were shown in table 1.
Table 1 . Histopathologic Features of Benign and Malign Nodules
| BENIGN n=44 | MALIGN n=20 | p | ||
Nodule Componet % | Solid | 68,2 | 35 | 0,026 |
Cystic | 2,3 | 0 | ||
Mix | 29,5 | 65 | ||
Echogenity % | İsoechoic | 52,3 | 65 | 0,341 |
Hypoechoic | 47,7 | 35 | ||
Hyperechoic | 0 | 0 | ||
Hypoechoic Halo % | Positive | 36,4 | 20 | 0,191 |
Negative | 63,6 | 80 | ||
Microcalcification % | Positive | 20,5 | 35 | 0,213 |
Negative | 79,5 | 65 | ||
Macrocalcification % | Positive | 11,4 | 20 | 0,357 |
Negative | 88,6 | 80 | ||
Border İrregülaritty % | Positive | 54,5 | 70 | 0,243 |
Negative | 45,5 | 30 |
CONCLUSION: In our study, we found malignancy rate 31,3 % in FLUS compared to the 5 - 20 % reported by different studies. Therefore, we think that, in the diagnostic and therapeutic approach of the FLUS nodules that challenge the clinician, this high ratio of malignancy must be kept in mind.
109 - Elastosonographical charachteristics, cytological results and histopathological features of nodules in patients with Hurthle cells - 2012
Uluslararası Bildiriler P-1820, 15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
AIM: The Hurthle cell is characterized cytologically as a large poligonal cell with abundant eosinophilic, granular cytoplasm and a large hyperchromatic nucleus with a prominent nucleolus. Hurthle cells are present in a variety of nonneoplastic and nonneoplastic conditions involving the thyroid and are not specific for any disease process. In this study, we aimed to evaluate ultrasonographical and elastosonographical characteristics, cytological results and histopathological features of nodules in patients with Hurthle cells in cytological examination and operated for various reasons.
MATERIAL AND METHOD: Patients admitted to Endocrinology and Metabolism Out-patient Clinic in Ankara Ataturk Education and Research Hospital between June 2009 and June 2010 and detected to have Hurthle cells in thyroid fine needle aspiration biopsy (FNAB) were included in the study. 57 patient /57 nodule recruited for the study. TSH, fT3, fT4, Tg and, Anti-TPO, Anti-TgAb were studied. Thyroid US, elastosonography, ultrasound guided FNAB, is performed. 14 cytomorphologic features examined to distinguish benign Hurthle cell lesions (BHCL) from Hurthle cell neoplasms (HCN). Operation indications in nodules including Hurthle cells cytologically were large nodule diameter, compression symptoms and increase in diameter of nodules with time. Nodules with a FNAB result of Hurthle cell neoplasm were operated because of high suspicion of malignancy. Histopathological evaluation was made by the same pathologist who evaluated cytopathology.
RESULTS: There were 57 patients with a mean age of 46.12±11.69 years. Among 57 nodules with Hurthle cells in cytological examination, 49 (86%) were classified as Bethesda 1 and 8 (14%) were classified as Bethesda 3. Histopathologically, 45 (78.9%) nodules were benign and 12 (21.1%) were malignant. When nodules were grouped according to Bethesda results, nodule volume, ultrasonographic features in gray-scale and vascularization pattern were similar in two groups. There was no signicant difference in terms of elastosonographic scoring and mean strain index (SI) between groups. Elastosonography scores determined in transverse axis were found to be more predictive for malignancy compared to scores determined in longitudinal axis (p=0.023 and p=0.867, respectively). However, calculated mean SI in longitudinal and transverse axis was significantly higher in malignant tumors than benign (p<0.05) ( Table 1). Cytological features were compared in benign and malignant nodules histopathologically . Nuclear groove, transgressing blood vessel (TBV) and absence of colloid were observed with a higher frequency in malignant nodules compared to benign nodules (p<0.05). ( Table 2).
CONCLUSION: Thyroid nodules containing Hurthle cells are composed of a wide range of pathologic entities, including Hashimoto thyroiditis, Hurthle cell adenomas , Hurthle cell carcinomas , oncocytic variant of papillary carcinoma and medullary carcinoma. Nuclear groove, transgressing blood vessel and absence of colloid were observed with a higher frequency in malignant nodules compared to benign nodules. In our study , SI values of malignant nodules were significantly higher than those of benign evaluated by elastosonography . Therefore. Higher SI values obtained during elastosonographical examination in malignant nodules compared to benign nodules suggest that SI might be used as a parameter to predict malignancy. SI determined by elastosonography will reduce unnecessary operations and surgical procedures.Since malignancy rate in our patient group was 21.1%, we think total or near total thyroidectomy should be preferred in nodules with Hurthle cells in cytological examination.
Table 1. Comparision of mean elastosonographic scores and strain index values according to histopathology results
Benign (n=45) | Malign (n=12) | p | ||
Transvers Score % | Score 1 | 2,2 | 0 | 0,023 |
Score 2 | 68,9 | 58,3 | ||
Score 3 | 20 | 0 | ||
Score 4 | 6,7 | 41,7 | ||
Score 5 | 2,2 | 0 | ||
Longitudinal Skor % | Score 1 | 4,4 | 0 | 0,867 |
Score 2 | 35,6 | 50 | ||
Score 3 | 33,3 | 25 | ||
Score 4 | 17,8 | 16,7 | ||
Score 5 | 8,9 | 8,3 | ||
Strain index | Transvers | 14,33± 2,48 | 35,25±9,31 | 0,003 |
Longitudinal | 21,24±3,79 | 40,98±9,03 | 0,027 |
Table 2. Comparative data of cytologic features of nodules according to of histopathologic results
Benign (n=45) | Malign (n=12) | p | ||
Cellularity % | scant | 57,8 | 41,7 | 0,606 |
moderate | 35,16 | 50 | ||
high | 6,7 | 8,3 | ||
Colloid % | absent | 15,6 | 33,3 | 0,035 |
scant | 28,9 | 58,3 | ||
moderate | 44,4 | 8,3 | ||
abundant | 11,1 | 0 | ||
Nuclear groove % | absent | 80 | 50 | 0,036 |
present | 20 | 50 | ||
TBV % | absent | 95,6 | 66,7 | 0,04 |
present | 4,4 | 33,3 |
108 - Urine neopterin levels in differentiated thyroid cancer - 2012
Uluslararası Bildiriler P-1775, 15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
Aim: Neopterin is a mareker of inflammation secreted from monocytes and macrophages. It is found to be increased in malignant diseases. The aim this study was to evaluate the urine neopterin levels in thyroid cancer.
Materials and methods: Sixty nine patients with thyroid cancer, 76 patients with benign thyroid pathology and 33 healthy subjects were evaluated. First morning urine samples were collected from the patients and the normal subjects for neopterin and creatinin measurment and stored at -20°C until analyzed.
Results: Neopterin levels were 149.3 (15.2-1602.2) μmol/mol creatinin in the malignant group, 32.0 (5.2-275.6) μmol/mol creatinin in the benign group and 9.2 (2.7-78.7) μmol/mol creatinin in normal subjects. Urinary neopterin levels were significantly higher in patients with throid cancer than patients with benign thyroid pathologies and normal subjects. There was 22 (%31.9) patients with chronic thyroiditis and 47 (%68.1) patients without chronic thyoiditis in the malignant. Urinary levels of neopterin didn’t differ in both groups (168.6 (21.3-716.8) μmol/mol creatinin and 135.3 (15.2-1602.2) μmol/mol creatinin respectively,P=0.381). Patients who had capsul invasion, vascular invasion and lymph node invasion had a higher urine neopterin level although not statistically significant.
Conclusion: Urinary neopterin levels are high in thyroid cancer and this result is not affected from the presence of chronic thyroiditis.
Declaration of interest: The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research project.
Funding: This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
107 - Histopathological results in patients with thyroidectomy due to repeated nondiagnostic cytologies - 2012
Uluslararası Bildiriler P-1743, 15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
AIM: Thyroid fine needle aspiration biopsy (FNAB) is an important diagnostic methodtoevaluate thyroid nodules. In FNAB cytological examination; it is reported that 70%of nodules is benign, 4% malignant, 10%suspiciousand 17% insufficient material (non-diagnostic). Despite all this, the biopsy of thyroid nodules reported as nondiagnostic at least 2 or 3 times causes indication for the operation. We aimed to assess ultrasonographical and histopathological data of thyroid nodules with repeated non-diagnostic cytology results.
MATERIAL AND METHOD: Seventy-five patients with nodular thyroid disease were enrolled in this study. Thyroid fine needle aspiration biopsy (FNAB) results were reported as non-diagnostic at least for 2-3 times in these patients. Operation indications were large nodule, ultrasonographically suspicious nodule, high elastosonography score or strain index and family history of thyroid cancer. Demographical features of these patients and ultrasonographical features of nodules were evaluated.
RESULTS: 53 (70.7%) patients were female and 22 (29.3%) were male. There were 59 patients with multinodular goiter (MNG), 8 patients with nodular goiter (NG), 7patients with Graves disease and MNG. 45 patients (60%) were euthyroid, 25(33.3%) had hyperthyroidism and 5 (6.7%) had hypothyroidism. In 41 patients (54.7%) nodules were localized in the right lobe, while in 34 (45.3%) patients in the left lobe (Table 1). Ultrasonographically, microcalcification was found in 30 nodules (40.0%) and macrocalcification was found in 20 nodules. Irregular margins were observed in 45 (60%) nodules and hypoechoic halo was observed in 28 (37.3%) nodules. 17(22.7%) nodules had peripheral vascularization and 1 (1.3%) nodule had peripheral macrocalcification. Histopathologically 57 (76%) nodules were benign and 18 (24%) were malignant. Of malignant nodules 17 (94.4%) were papillary carcinoma, whereas 1 was follicular carcinoma. Mean tumor diameter was 0.77±0.63 (range 0.1-2.2) cm. Vascular invasion, capsular invasion, extracapsular extension and multicentricity were detected in 1 (5.6%), 5 (27.8%), 1 (5.6%) and 6 (33.3%) patients, respectively.
CONCLUSION: In our study we found the rate malignancy 24% as high for thyroid nodules which were performed FNA biopsy and reported repeated non-diagnostic cytology results. Therefore, we conclude that when treatment is planned for the patients that have non-diagnostic cytology possibility of high rate of malignancy as we found in this study may be considered.
Table 1. Ultrasonography features and histopathological findings in patients with repeated non-diagnostic cytology results
n | % | |
Nodule localization Right lobe Left lobe | 41 34 | 54.7 45.3 |
Calcifications Macrocalcification Microcalcification | 30 20 | 40.0 26.7 |
Irregular margins Hypoechoic halo Peripheral vascularisation Peripheral macrocalcification Echogenicity Isoechoic Hypoechoic Texture Solid Mixed Cystic | 45 32 17 1 43 32 40 34 1 | 60.0 37.3 22.7 1.4 57.3 42.7 53.3 45.3 1.3 |
Histopathological findings Benign Malignant Papillary tm Follicular tm Vascular invasion Capsular invasion Extracapsular invasion Multisentricity | 57 18 17 1 1 5 1 6 | 76.0 24.0 94.4 5.6 5.6 27.8 5.6 33.3 |
106 - Evaluation of the cytopathologic findings of the thyroid nodules which include macrocalcification - 2012
Uluslararası Bildiriler P-1709, 15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
AIM: Evaluation of thyroid noduleswith ultrasound hasbeenrecently become very important. Ultrasonographically; solid nodule, hypoechogenicity, microcalcifications, macrocalsifications, border irregularity, intranodular vascularity is associated with increased risk of malignancy, In this study, we aimed to evaluate the cytological findings of the thyroid nodules in which macrocalcification is determined with ultrasonography.
MATERIAL AND METHOD: We retrospectively evaluated 907 nodules of 269 patients with nodular or multinodular goiter and macrocalcification at least in one nodule. The nodules without macrocalcifications in the same patients were taken as the control group. Thyroid function tests, ultrasonographical features and cytological results of the nodules were evaluated in all subjects. Cytological findings are classified as benign, non-diagnostic, suspicious and malignant.
RESULTS: There were 215(79.9%) female and 54(20.1%) male patients. Macrocalcification was present in 420 nodules (Group1). No macrocalcification was observed in 487 nodules (Group 2) (Table-1). Group 1 was furtherly divided into two groups. Group 1A: nodules with peripheral macrocalcification (n=53) and group 1B: nodules with intranodular macrocalcification (n=367). Mean nodule size in group 1A, 1B and 2 were 12.94±6.26 milimeter (mm), 25.50±14.27 mm and 15.72±7.53 mm, respectively (p<0.001)(Table-2). In ultrasonography, prevalence of peripheral irregularity and presence of halo were similar in Group 1 and 2. Microcalcification was observed in 61.4% of nodules in group 1 and 17.5% of nodules in group 2 (p<0.001). Rate of solid nodules was significantly lower in group 1 compared to group 2 (11.7% vs 49.9%, p<0.001). We observed that malignant and suspicious cytology results were significantly higher in group 1 compared to group 2 (p=0.004 and p=0.003, respectively) (Table- 1). In group 1A, only rate of suspicious cytology results was higher than group 2 (p=0.010) (Table 2). In group 1B, both suspicious and malignant cytology results were higher compared to group 2 (p=0.007 and p=0.003, respectively) (Table- 3).
CONCLUSION: This study showed that presence of macrocalcification and particularly presence of intranodular macrocalfication was associated with higher malignant and suspicious cytology results. We think presence of macrocalcification in ultrasonography should not be always taken in favour of benignity in contrast to the usual opinion and FNAB should also be performed in these nodules.
Table 1. Comparison of thyroid nodules with and without macrocalcifications
CYTOLOGY | GROUP 1 % | GROUP 2 % | P |
Benign | 75.2 | 80.3 | 0.067 |
Malignant | 3.6 | 0.8 | 0.004 |
Suspicious | 5.5 | 1.8 | 0.003 |
Non-diagnostic | 15.7 | 17 | 0.590 |
Table 2. Comparison of thyroid nodules with peripheral macrocalcifications and without macrocalcification
CYTOLOGY | GROUP 1A % | GROUP 2 % | P |
Benign | 67.9 | 80.3 | 0.036 |
Malignant | 1.9 | 0.8 | 0.442 |
Suspicious | 7.5 | 1.8 | 0.010 |
Non-diagnostic | 22.6 | 17 | 0,309 |
Table 3. Comparison of thyroid nodules with intranodular macrocalcifications and without macrocalcifications
CYTOLOGY | GROUP 1B % | GROUP 2 % | p |
Benign | 76.3 | 80.3 | 0.159 |
Malignant | 3.8 | 0.8 | 0.003 |
Suspicious | 5.2 | 1.8 | 0.007 |
Non-diagnostic | 14.7 | 17 | 0.359 |
105 - The effect of radio-iodine treatment on helicobacter pylori eradication - 2012
Uluslararası Bildiriler P 1687- 15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
INTRODUCTION: Radioactive treatment after surgery forms the basis of treatment of differentiated thyroid cancers (DTC) and also used as permanent theraphy of hyperthyroidism. Iodide is being transported into the thyrocytes by the NIS system that located on the thyrocytes' cell membran.NIS system also has been shown at the gastric mucosa. H. pylori prevalence of 90% in developing countries, as well as the wide variety of drugs are given intensive treatments because of high morbidity. In addition, the development of resistance for antibioticis is now common and frequent recurrence so researchers has led to finding new and more effective treatment. In this study we proposed to analyse the effect of low and high dose radio-iodine treatment on helicobacter pylori eradication.
MATERIAL AND METHOD: Total 87 patients included for study. The patients investigated detailed about medications and gastrointestinal symptoms Patients have neither dyspeptic symptoms nor any usage of H2 receptor bloker,proton pump inhibitor,antiasit or any form of antibiotics. Undergoing gastric surgery were excluded . Urea breath test before and 2 months after radio-iodine treatment have been made for detection of Helicobacter pylori eradication.
FINDINGS: The radio-iodine treatment has been planned to give as permanent threapy to 76 patient (%87,4) with hyperthyroidism and 11 patient(%12,6) with differantial thyroid cancer. The average dose of given radio-active iodine to patients for ablation purposes is 115±3.3 mCi and 22.7±1.4 mCi. Before RAI treatment,in the group of DTC the urine breath test (UBT) result of the 44 patients had positive HP and 32 of them had negative HP, and for hyperthyroid patients 4 of them had positive HP and 7 of them had negative HP. All patientshaving initial positive test results, had also Positive control test results at the 2nd month of the RAI treatment(%100). (Table 1). Both patient group having initial negative test results, had also negative control test results (Table 1).
Table 1. Rodyoaktif iodine-treated patients before and after treatment of urea breath test (UBT) results
| Before treatment UBT | After treatment UBT | Total | |
Negative | Positive | ||
Negative | 39 | 0 | 39 |
Positive | 0 | 48 | 48 |
Total | 39 | 48 | 77 |
RESULT
The frequency of H. pylori in developing countries has been increasing steadily. Development of resistance to the treatments and frequent recurrences due to explored ways to more effective treatment. There are some literature studies show that RAI treatment is effective on HP eradication. Our results indicate that low and high dosage of RAI treatment does not have any effect on HP eradication in early period.
104 - Prevalance of thyroıd dıseases ın patıents wıth colon cancer and benıgn colon polyps - 2012
Uluslararası Bildiriler P 1682-15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
AIM: In this study, we aimed to evaluate thyroid functions, thyroid antibody positivity, thyroid ultrasonography (US) findings and prevalance of thyroid cancer in patients with colon cancer and benign colon polyps. Also, we aimed to compare prevalance of thyroid diseases in two groups.
MATERIAL AND METHOD: This study was designed as a prospective study by Department of Endocrinology and Metabolism Clinic in Ankara Ataturk Research and Education Hospital. 57 patients with colon cancer and 50 patients with colon polyps that were referred from gastroenterology and medical oncology clinics between October 2010-January 2011 were included in the study. Patients with colon cancer were operated previously, followed in remission and were not taking chemotherapy or radiotherapy actively. Colon polyp group included patients diagnosed to have polyps during routine colonoscopy examination. In two groups, TSH, FT3, FT4, anti-TPO and anti-Tg antibodies and Tg were measured. All patients were evaluated with thyroid US and thyroid fine needle aspiration biopsy (FNAB) was performed in indicated nodules. Cytology results were classified as benign, nondiagnostic, suspicious and malignant.
RESULTS: There were 57 (53.27%) patients with colon cancer (22 female, 35 male) and 50 (46.23%) patients with colon polyps ( 17 female, 33 male). There was no difference in terms of age and sex distribution between groups (p=0.622 and p=0.529, respectively). Ultrasonographically, nodular and multinodular goiter was observed in 30 (52.63%) patients with colon cancer and 29 (56%) patients with polyp. Thyroiditis was observed in 14 (24.56%) patients with colon cancer and 16(32%) patients with polyp (Table 1). FNAB is performed to 23 patients with colon cancer and 14 patient with colon. FNAB is performed to cytology was reported as malignant in 1 patient with cancer and in 1 patient with polyp. In these 2 patients and in another colon cancer patient with suspicious FNAB result, thyroid cancer was confirmed histopathologically. Presence of thyroid disease defined as thyroid dysfunction or positive antithyroid antibody or presence of nodule or thyroiditis in US was found in 44 (77.19%) patients with cancer and 44 (88.0%) patients with polyp (p= 0.228 ).
Table 1. Thyroid ultrasonography findings according to colon pathologies
| Ultrasonographic Findings | Colon Carsinom (n=57) | Colon polyp (n=50) | p |
| Normal | 6 (%10.53) | 4 (%8) | 0.478 |
Minimal heterogeneous | 7 (%12.28) | 2 (%4) | |
Nodular Goiter | 7 (%12.28) | 9 (%18) | |
Multinodular Goiter | 23 (%40.35) | 19 (%38) | |
Thyroiditis | 14 (%24.56) | 16 (%32) |
CONCLUSION: This study showed that thyroid dysfunctions, thyroid US findings and prevalance of thyroid cancer are similar in patients with colon cancer and colon polyps. Since thyroid pathologies are observed in more than 2/3 of patients in both groups, we think laboratuary examinations for thyroid functions and thyroid antibodies and thyroid US should be a part of investigation in patients with colon cancer and colon polyps.
103 - Anti neutrophil cytoplasmic antibody levels ın graves patients using propylthıourasıl - 2012
Uluslararası Bildiriler P 1660-15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
AIM: Antineutrophil cytoplasmic antibody (ANCA) positivity is usually determined in medium and large vessel vasculitis. This antibody has two different forms. Cytoplasmic ANCA (PR3-ANCA) occurs against proteinase -3, while perinuclear ANCA (MPO-ANCA) occurs against myeloperoxidase and bactericidal-permeability increasing proteins. The presence of ANCA is mostly seen in systemic vasculitis and also in drug induced vasculitis. There is no sufficient data about prevalance of positivity ANCA and development of antithyroid antibodies after treatment. In this study our aim was to investigate MPO-ANCA and PR3-ANCA levels in Graves patients using propylthiourasil (PTU)..
MATERIAL AND METHOD: 52 Graves patients (9 men,41 women) using PTU and 37 healthy control group were included in the study. TSH , fT3, fT4, anti TPO, anti Tg, tiroglobulin (Tg), MPO-ANCA ve PR3-ANCA levels of patients and control groups were evaluated.
RESULTS: Mean level of PR3-ANCA in Graves group was significantly higher than control group (p=0.025). No significant difference was found between levels of MPO-ANCA (p=0.109) ( Table-1). Positive correlation was observed between Anti-TPO, AntiTG with PR3-ANCA in patient group (respectively, p=0.001, r=0.447; p=0.030, r=0.310). No correlation was observed between Anti-TPO, AntiTG with MPO-ANCA. No correlation was observed between TSH, fT3, fT4, Tg levels with MPO-ANCA and PR3-ANCA. Longer duration of treatment in the patient group showed increased levels of PR3-ANCA (p=0.024, r=0.314). Positive anti-Tg was detected in 33 patients with Graves' disease (anti-Tg> 4.11 IU/ml) and in 10 patients in the control group. PR3-ANCA levels in anti-Tg positive patients were higher than those with negative (p=0,006). Positive anti-TPO was detected in 34 patients with Graves' disease (anti-Tg> 5.61 IU/ml) and in 6 patients in the control group. There was no statistically significant difference forMPO-ANCA and PR3-ANCA levels between Anti-TPO-positive and negativecases. MPO-ANCA and PR3-ANCA were positive in two Graves patients while only MPO-ANCA positive in two patients. ANCA positivity in Graves' patients was detectedto be 7.6%.In the control group of patients there were nopositive MPO-ANCA and PR3-ANCA patients.
Table 1: Comparison of laboratory values of the groups
Graves group (n=52) | Control group (n=37) | p | |
TSH (uIU/ml) | 1.64±1.73 | 2.13±1.45 | 0.167 |
fT3 (pg/ml) | 3.43±1.31 | 3.49±0.34 | 0.820 |
fT4 (ng/dl) | 1.36±0.84 | 1.13±0.12 | 0.115 |
Tg (ng/ml) | 44.22±84.64 | 21.92±28.24 | 0.139 |
Anti TPO (IU/ml) | 325.18±408.16 | 75.90±206.70 | 0.001 |
Anti Tg (IU/ml) | 145.79±263.96 | 18.70±55.97 | 0.005 |
MPO-ANCA (U/ml) | 3.45±2.97 | 2.65±0.21 | 0.109 |
PR3-ANCA (U/ml) | 2.94±0.67 | 2.64±0.52 | 0.025 |
CONCLUSION: PTU may cause ANCA positivity but vasculitis not develop in all cases. ANCA positivity mechanism due to PTU is unknown. PTU related ANCA positivity is reported 4.1-64%. In our study PTU induced ANCA positivity rate in patients with Graves' was 7.6%. There are publications reporting the correlation between ANCA production and duration of treatment with PTU and thyroid autoantibodies. In our study we also detected correlation between ANCA production and duration of treatment with PTU and thyroid autoantibodies. In our study, higher ANCA levels were found in Graves patients recieving long term PTU treatment.
102 - Evaluation of pituitary gland with magnetic resonance imaging in hypogonadic patients - 2012
Uluslararası Bildiriler P 1470-15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
AIM: Hypogonadism occurs as a result of testicular failure and/or insufficient pituitary stimulation. Various hypothalamo-pituitary abnormalities or lesions can contribute to hypogonadism. Benign or malignant tumoral lesions of cellar or paracellar region may be associated with hypogonadism. Therefore, patients with hypogonadism should be evaluated with pituitary magnetic resonance imaging (MRI). In this study, we aimed to investigate hypothalamo-pituitary MRI findings in patients with hypogonadism.
MATERIAL AND METHOD: Forty nine patients with hypogonadism followed in our clinic were included in the study. Pituitary MRI findings in these patients were evaluated retrospectively.
RESULTS: There were fourty two (79.4% ) patients with hypogonadotrophic hypogonadism and seven (20.6%) patients with hypergonadotrophic hypogonadism. 80.9% of patients with hypogonadotrophic hypogonadism were male and 19.1 % were female. Distribution of pituitary MRI findings of these patients were as follows: 59.5% normal, 16.7% pituitary microadenoma, 11.9% partial empty sella, 4.7% pituitary macroadenoma, 2.4% empty sella, 2.4% ectopic neuropituitary, and 2.4% empty sella and ectopic neuropituitary (Table 1). In the hypergonadotrophic group all of the patients were male. In this group pituitary MR findings were normal in 71.4%, ectopic neuropituitary in 14.3% and pituitary microadenoma in 14.3% (Table 1).
CONCLUSION: In half of the patients with hypogonadotrophic hypogonadism, Pituitary MRI findings may be normal. In these patients, if clinic and laboratory results are harmonious, to determine the diagnosis dynamic tests are required and appropriate therapy must be done, even if pituitary MRI is normal. In the hypergonadotrophic hypogonadic patients, although etiology is not associated with hypothalamus and / or pituitary gland, we can find pathologic pituitary MRI results. So, we suggest, to carry out hipothalamo-pituitary imagining with hypergonadotrophic patients.
Table 1. Hypothalamo-pituitary MRI findings in patients with hypogonadism
| PITUITARY MRI FINDINGS | HYPOGONADOTROPHIC HYPOGONADISM N = 42 | HYPERGONADOTROPHIC HYPOGONADISM N = 7 |
Normal | % 59,5 | % 71,4 |
Empty Sella | % 2,4 | - |
Partial Empty Sella | % 11,9 | - |
Ectopic Neuropituitary | % 2,4 | % 14,3 |
Microadenom | % 16,7 | % 14,3 |
Macroadenom | % 4,7 | - |
Ectopic neuropituitary,Empty Sella | % 2,4 | - |
101 - Insulin resistance and the effect of treatment on insülin resistance in patients with prolactinoma - 2012
Uluslararası Bildiriler P-1399, 15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
Aim: The relationship between hyperprolactinoma and insulin resistance has been shown in many studies. It is also known that hyperprolactinoma causes changes in carbohydrate and lipid metabolism. The aim of our study is to evaluate insulin resistance in patients with prolactinoma and see the effect of treatment on insulin resistance and karotis intima media thickness (CIMT).
Material and methods: Twenty-two female patients diagnosed biochemically and radiographically with prolactinoma were included in the study. None of the patients were treated previously. Median age of the patients was 30.0+- LDL-cholesterol, HOMA score, prior to treatment and 6 months after starting treatment. The body mass index (BMI) was measured and CIMT was evaluated for each patient prior to and 6 months after the treatment.
Conclusion: Treatment with cabergolin causes decrease in HOMA score and decrease in CIMT after 6 months of treatment independant from the decrease in BMI.,
Results: The prolactin levels before and after treatment was 145.5+-66.4 and 12.4+-7.2 μg/l respectively (P<0.001). This decrease was not related to the decrease in BMI(r=-0.057, P=0.808). HOMA score before and after treatment was 1.25 (0.22-4.5) and 1.02 (0.24-4.1) respectively (P=0.024). This decrease was not related to the decrease in prolactin levels (r=-0.248 vs P=0.279). Homocystein levels before and after treatment was 13.8 (7.0-28.0) and 8.5 (2.3-26.4) (P<0.001) respectively. CIMT before and after treatment was 0.58+-0.15 and 0.52+-.12 (P<0.05) respectively. The decrease in CIMT was not found to be related with the decrease in prolactin levels, HOMA score and BMI (r=0.250, P=0.274).
Declaration of interest: The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research project.
Funding:This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
100 - Effect of obesity on vitamin D and parathormone levels - 2012
Uluslararası Bildiriler P 1223-15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
AIM: Obesity is quickly growing health problem and associated with many comorbid disease. One of them is abnormalities seen in calcium metabolism. It is reported that vitamin D deficiency can be seen in obese people. It is thought that Vitamin D deficiency can effect insulin sensitivity and can be a risk factor for impaired glucose tolerance (IGT) and diabetes mellitus (DM). Parathormone (PTH) increase seen in obese people can be attributed to vitamin D deficiency but there are some publications report that PTH increase is independently related with obesity. In this study our aim was to investigate the relationship between obesity and vitamin D and hyperparathyroidism.
MATERIAL AND METHOD: 127 healthy persons included in this study and anthropometric measurements were performed. Body fat mass and fat percentage is determined. Study group were divided into four groups according to body mass index. Group 1 (n=35) BMI 18,5-24,9 kg/m², Group 2 (n=35) BMI 25-29,9 kg/m², Group 3 (n=35) BMI 30-34,9 kg/m², Group 4 (n=22) BMI 35-40 kg/m². Serum calcium (Ca), phosphorus (P), parathormone (PTH), 25(OH)D, fasting glucose and fasting insulin levels were evaluated.
RESULTS: Antropometric measurements of the groups are listed in Table-1andlaboratory dataarelisted in Table-2. Serum Ca levels of Group 2 were significantly higher thanGroup 3 and Group 4, respectively (p= 0.049 and p=<0.001). Vitamin D levels of Group 4 were significantly lower than group 2 (p= 0.033). In all groups, fasting glucose and fasting insulin levels showed a statistically significant increase with the increase ofwaist circumference (respectively, p= 0.004, r= 0.254 and p= 0.001, r= 0.290). Statistically significant decrease in waist circumference was observed with increasing vitamin D levels (p = 0.049, r = -0.178),but serum Ca decreasewas not statistically significant. With the increase in BMI,statistically significant increase were determined in fasting glucose and fasting insulin levels (respectively, p= 0.001, r= 0.296 and p= 0.003, r= 0.259)while significant decreasewere determined in serum Ca and vitamin D levels(respectively, p=0,040, r=-0,181 ve p= 0,016, r= -0,214). Negative correlation was determined betweenbody fat massand serum Ca and vitamin D levels(p= 0.021, r= -0.204, p= 0.026, r=-0.199), whereas no significant correlation was determined between body fat massand PTH levels. Fasting glucose levels showed a statistically significant increase with increasing serum Ca levels(p=0.010, r=0.226)while no significant correlation was determined between fasting glucose levels and P, PTH and vitamin D levels.
CONCLUSION: The literature suggests that low vitamin D levels in obesity is negative correlated with BMI, waist circumference and fat mass. In our study, significant decrease was observed in vitamin D and serum Ca levels while body fat mass. Statistically significant decrease in the level of vitamin D was determined with increasing waist circumference although there was no significant reduction in serum Ca levels. Negative correlation was observed between body fat mass and serum Ca and vitamin D levels. The findings of our study support that there is a negative correlation between vitamin D levels and waist circumferance and body fat mass. There are publications indicating that increase in PTH isnt depending on decrease of vitamin D, it is directly associated with obesity. But in our study there was no association between obesity and PTH levels. It is tought that vitamin D deficiency may be a risk factor for IGT and DM and can affect insulin sensitivity. However, in our study no significant relationship was observed between fasting glucose levels and vitamin D levels. In conclusion, our results support the view that vitamin D deficiency in obese individuals isn’t related with insulin resistance.
Table 1:Antropometric measurements of the groups
Group 1 | Group 2 | Group 3 | Group 4 | |
Waist circumference (cm) | 79,17±8,75 | 91,26±7,25 | 97,82±5,25 | 108,95±12,33 |
BMI (kg/m²) | 22,54±1,90 | 27,56±1,55 | 31,96±1,60 | 37,19±1,45 |
Fat mass (kg) | 43,39±3,51 | 46,53±6,67 | 49,45±6,19 | 53,20±6,75 |
Fat percentage (%) | 25,99±6,14 | 33,56±6,43 | 38,57±5,41 | 42,15±5,32 |
Table 2: Laboratory results of the groups
Group 1 | Group 2 | Group 3 | Group 4 | |
Fasting glucose (mg/dl) | 85,45±6,77 | 89,14±8,55 | 91,00±5,81 | 90,95±8,71 |
Serum Ca(mg/dl) | 9,24±0,34 | 9,40±0,31 | 9,21±0,28 | 9,05±0,31 |
Serum P (mg/dl) | 3,58±0,41 | 3,53±0,46 | 3,44±0,33 | 3,63±0,59 |
Vitamin D(µg/l) | 28,20±14,30 | 30,06±18,48 | 22,20±13,38 | 18,96±9,88 |
PTH (pg/ml) | 65,63±36,05 | 71,68±24,90 | 77,47±30,06 | 73,81±27,62 |
Fasting insulin(uIU/ml) | 5,41±3,27 | 8,68±5,41 | 9,53±5,16 | 7,16±3,05 |
99 - Measles and new onset type 1diabetes presented with bilateral facial paralysis: report of a case - 2012
Uluslararası Bildiriler P-582, 15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
INTRODUCTION: Measles virus infections generally occur in childhood, but infections in adolescence and adulthood can lead to complications. Here we present an adult patient with positive measles serology who was diagnosed with new onset type 1 diabetes and bilateral facial paralysis.
CASE: A previously well 28-year-old woman had suffered from fever, nausea, vomiting and generalized fatique for one day before being transferred to our emergency department in a confused state. Physical findings on admission were height 150 cm and body weight 88 kg, with a body mass index of 39 kg/m2. She had a fever of 38 Celsius degrees. Laboratory data on admission are demonstrated in Table 1. She was treated by intravenous infusion of saline and insulin and eventually switched to intensive insulin therapy four times a day. On the second day of hospitalisation she developed weakness on both sides of her face. On physical examination, there was bilateral facial nerve paralysis. An electroneuromyography demonstrated bilateral axonal neuropathy of the facial nerve and confirmed the diagnosis. We performed serological testing for several viral antibodies. The results revealed significant elevation of the measles IgM and IgG titers but no abnormal results were shown in any of the other serological tests (Table 2). One week later, the patient’s facial weakness had improved spontaneously with no residual weakness.
Table 1. Laboratory data on admission.
Complete Blood Count | |
WBC | 11200/µl |
Hb | 13 g/dl |
Plt | 23.4 x 104/µl |
Blood Chemistry | |
BUN | 23 mg/dl |
Cre | 1.2 mg/dl |
Alb | 4.7 g/dl |
Na | 122 mEq/l |
K | 3.8 mEq/l |
SGPT | 17 IU/l |
SGOT | 15 IU/l |
T-Chol | 135 mg/dl |
TG | 324 mg/dl |
Amylase | 92 IU/l |
Glu | 421 mg/dl |
HbA1c | 9.2 % |
Urinalysis | |
Glucose | 3+ |
Protein | 1+ |
Ketone | 4+ |
Arterial Blood Gas Analysis on 2 L/min oxygen by mask | |
pH | 7.143 |
pO2 | 98.0 mmHg |
pCO2 | 23.7 mmHg |
HCO3- | 8.4 mmol/l |
Table 2. The results of serological testing for viral antibodies (IU/ml)
Measles virus* | IgM | 1.44 (0-1.2) |
IgG | 1.86 (0-1.1) | |
Mumps virus | IgM | 0.48 |
IgG | 0.09 | |
Rubella virus | IgM | 0.16 |
IgG | >400 | |
Varicella zoster virus | IgM | 0.67 |
IgG | 2.23 | |
Cytomegalovirus | IgM | negative |
IgG | 420 | |
EBV-anti VCA | IgM | 0.93 |
IgG | 303 | |
Herpes Symplex virus | IgM | negative |
IgG | 52.662 | |
Borrelia Burgdorferi | IgM | 0.42 |
IgG | 0.43 | |
Treponema Pallidum | Hemagg. | (-) |
DISCUSSION
Data on T1DM comes from the Swedish Childhood Diabetes Study which showed a significantly higher rate of children who developed diabetes and were not vaccinated against measles. The authors hypothesized that measles vaccine could have a protective effect or that measles infection could be a diabetogenic agent. The differential diagnosis of the causes for bilateral facial paralysis covers a wide field, including genetic, infectious, traumatic, neoplastic, metabolic, neurological, vascular, iatrogenic and idiopathic etiologies. Measles is not among the well documented infectious etiologies but three adult patients with acute renal failure and bilateral facial paralysis have been reported. Our patient had an atypical presentation of measles, as expected in adults, because of fever and positive measles IgG and IgM antibodies. Our case is interesting due to coexistence of bilateral facial paralysis, new onset T1DM and positive measles serology. And there is not a similar case in the literature. Although there are limitations with respect to the true relation between measles and these two manifestations, this clinical picture should be kept in mind as a possible atypical presentation of measles infection in adults.
98 - Plasmapheresis therapy in a case with recurrent pancreatitis attacks as a consequence of hypertryglyceridemia - 2012
Uluslararası Bildiriler P-416, 15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
INTRODUCTION: Hypertrygliceridemia is responsible from 1-4% of all acute pancreatitis cases. Risk of pancreatitis increases if plasma tryglyceride levels are above 1000-2000 mg/dl. Medical therapy is usually insufficient for cases of hyperlipidemia with serious and recurrent pancreatitis attacks. Here,we have reported a case of recurrent pancreatitis due to hypertriglyceridemia which was resistant to medical treatment and could be effectively controlled with single time plasmapheresis therapy
CASE: 45 years old female patient has been referred to our endocrinology clinics because of hypertrygliceridemia. We have learned from the history of the patient that she had underwent cholecystectomy in an another hospital in 2005 to which she had admitted with the complaints of abdominal pain and diagnosed to have acute billiary pancreatitis. After cholecystectomy she had to be hosptalized in almost every 2-3 months because of recurrent pancreatitis attacks. Hypertyglyceridemia was recognised in the detailed routine laboratory tests. Her plasma triglyceride level was above 2000 mg/dl despite she has received gemfibrosil and fenofibrate alternately since March of 2006 and she had her last pancreatitis attack one month before her referral to us. In our clinics, the patient’s liver enzymes, serum acute phase reactants (crp), serum amylase and lipase levels were found to be normal. The patient’s serum triglyceride level was 9000 mg /dl and she has received single time plasmapheresis therapy in volume of 4 liters and in exchange of albumin. One day after single-time plasmapheresis her trigyceride level has decreased to 600 mg/dl and on the third day it was 400 mg/dl.Patient has been discharged with fenofibrate therapy.
RESULTS: Acute pancreatitis occuring secondary to hypertriglyceridemia is generally treated with agressive hydration and pain control and its prognosis is not different from the others. Serious or recurrent pancreatitis can be indications for plasmapheresis. Plasmapheresis is able to reduce serum triglyceride levels effectively and it also removes serum active enzyme, proteases and proinflammatory molecules from the circulation. Altough there are reports about the effectiveness of plasmapheresis in prevention of recurrent pancreatitis attacks , there is no consensus about the appropriate frequency and number of plasmapheresis which should be applied to a patient with high triglyceride levels. In our case after single time plasmaphersis and fenofibrate therapy, our patient’s triglyceride level has returned to the normal range and she hasn’t had any recurrent attacks for the four months. We have thought that plasmapheresis is cost effective because it reduces the need for hospitalization.
| Table 1.LABORATORY TEST RESULTS | ||
| BEFORE PLASMAPHERESIS | AFTER PLASMAPHERESIS | |
FPG | 82 mg/dl | |
TG | 9000 mg/dl | 439mg/dl |
HDL | 19mg/dl | 20.5mg/dl |
LDL | 295mg/dl | 6.7 mg/dl |
VLDL | 1610mg/dl | |
AST | 18U/L | |
ALT | 19 IU/L | |
GGT | 11U/L | |
AMILASE | 77 U/L | |
LİPASE | 27U/L |
97 - Evaluation of clinical and laboratory findings of our primary hyperparathyroid patients - 2012
Uluslararası Bildiriler P 264-15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
AIM: Primary hyperparathyroidism (PHP) is a disease characterized by hypercalcemia and accompanying with increase in parathyroid hormone (PTH) levels. In this study our aim was to evaluate clinical and laboratory findings of our primary hyperparathyroid patients and detect complications caused by hyperparathroidism.
MATERIAL AND METHOD: 83 primary hyperparathyroid patients (73 women,10 men) were included in this study. Serum calcium (Ca), phosphorus (P), parathormone (PTH), 25(OH)D, 24 hour urine Ca and P levels, bone mineral density and renal ultrasonography were evaluated.
RESULTS: The mean age at diagnosis was 52.4±9.6 years. Laboratory values of patients are summarized in Table-1. Hypercalciuria was detected in 27 patients (%32.5) while nephrolithiasis was determined in 17 patients (%20.5). In 16 patients (%19.3) BMD was normal. In 31 patients (%37.3) osteopenia, in 36 patients (%43.4) osteoporosis was determined. Vit D deficiency was found in 38 patients (%45.8). 9 patient (10.8%) had normal thyroid ultrasonography, 23 patient (27.7%) had chronic thyroiditis, 11 patient (13.3%) had nodulary goitre and 40 patient (48.2%) had multinodulary goitre. With these results operation were recomended to 44 patients (%47). In 3 patients atypical parathyroid adenoma and in 4 patients (16%) incidental papillary thyroid microcarsinoma were detected in histopathological evaluation.
Table 1: Laboratory data of our patients
Serum Ca(mg/dl ) | 10.47±0.67 |
Serum P(mg/dl) | 2.85±0.50 |
PTH (pg/ml) | 254.12±140.72 |
25-OH vitamin D3 (µg/l ) | 22.97±16.15 |
24 hour Ca (mg/day) | 354.52±177.23 |
CONCLUSION: In recent years primary hyperparathyroidism is detected in asymptomatic phase and fewer complications are found. In 70-80% of PHP patients no symptoms and signs are observed. They are detected incidentally only with the hypercalcemia. The most common finding in symptomatic patients is nephrolithiasis. Overt skeletal disease is rare but incidence of osteoporosis-related fracture is increasing. We detected nephrolithiasis in 20.5% patients, osteopenia in 37.3% and osteoporosis in 43.4% of patients. Frequently seen vitamin D deficiency and elderly patients may have contributed to the high prevalence of osteopenia and osteoporosis. The risk of multigland involvement and bigger adenoma is higher in cases accompanied by a lack of Vitamin D. In our study, vitamin D deficiency was observed in 45.8% of PHP patients. Thyroid malignancies accept medullary thyroid carcinoma are reported in 2.1-4.3% of patients who were operated for PHP. In our study, 16% incidental papillary microcarcinoma was detected.
96 - Evaluation of glucose metabolism in Primary hyperparathyroid patients - 2012
Uluslararası Bildiriler P 222-15th International Congress of Endocrinology and 14th European Congress of Endocrinology, 5-9 May 2012, Florence, Italy
ABSTRACT
AIM: In recent years, primary hyperparathyroidism (PHP) is frequently detected in asymptomatic patientsdue to the routine measurement of serum calcium (Ca) levels.As a result of this; metabolic effects cause increased cardiovascular morbidity began to gain importance instead of the classic signs in PHP patients. There are publications showed the increasedincidence of insulin resistance, impaired glucose tolerance (IGT), anddiabetes mellitus (DM)in PHP. In this study our aim was to investigate frequency of impaired glucose tolerance, undiagnosed diabetes mellitus and presence of insulin resistance by HOMA.
MATERIAL AND METHOD: 55 primary hyperparathyroid patients (50 F, 5 M ) without known glucose tolerance were included in this study. The control group (52 F,3 M) was with similar BMI, normocalcemic, without known glucose tolerance. Serum calcium (Ca), serum phosphorus (P), parathyroid hormone (PTH), vitamin D, fasting glucose and fasting insulin levels were measured in PHP patients and the control group. 75 gr oral glucose tolerans test (OGTT) was performed to PHP patients and control group. Second hour glucose and insulin levels were measured in theOGTT.Insulin resistance was calculated by HOMA-IR (fasting glucose (mg/dl) x fasting insülin (mU/l)/ 405).
RESULTS: There was no significant differences between PHP and control group according to the fasting glucose, fasting insulin and HOMA-IR levels. Second hour glucose and insulin OGTT value were significantly higher than control group (respectively, p= 0.001, p= 0.020) (Table-1). While IGT was detected in 6 PHP patients (11.3%), there is no IGT in control group (p= 0.013). Diabetes mellitus (DM) didn’t detected in OGTT in PHP patients. In PHP group there were positive corelation between Ca levels and fasting plasma glucose (p= 0.005, r= 0.376). There was no statistical corelation between serum Ca levels and fasting insulin levels and HOMA-IR. In PHP group there was negative corelation between PTH levels and vitamin D levels (p= 0.023, r= -0.306) while there was no corelation between PTH and fasting glucose and fasting insulin levels and HOMA-IR. In PHP group there was negative corelation between vitamin D levels and fasting glucose (p= 0.040, r= -0.278). There was no statistical corelation between vitamin D levels and fasting insulin levels and HOMA-IR. Mean serum Ca level (11,16±0,76 mg/dl) of BGT group was statistically higher than non BGT group’s serum Ca levels (10,35±0,78 mg/dl) (p= 0.020).
CONCLUSION: PHP is considered to change glucose tolerance by decreasing insulin sensitivity. There are publications reporting increased frequency of BGT and DM in PHP. In our study we verified the increased frequency of BGT in PHP patients and the prevalance of BGT was 11.3%. But we didn’t found DM in OGTT and no increased insulin rezistance. In our study we observed positive corelation between serum Ca levels and fasting glucose. Serum Ca levels were higher in BGT group than non BGT group. This situation support the opinion of risk factor of serum Ca in glucose metabolism. It is reported that vitamin D defiency could be risk factor for BGT and DM and can effect insulin sensitivity. In our study we found negative corelation between vitamin D levels and fasting glucose in PHP group. This suggest that vitamin D defiency can effect glucose metabolism. As a result frequency of BGT is increased in PHP patients. Increase in serum calcium levels effect the glucose metabolism and cause glucose intolerance.
Table 1: Laboratory results of the groups
PHP (n=55) | Control(n=55) | p | |
Age(year) | 52,16± 9,67 | 50,74±8,56 | 0,152 |
BMI(kg/m²) | 29,19±4,92 | 29,54±4,38 | 0,676 |
Serum Ca (mg/dl ) | 10,46±0,81 | 9,26±0,39 | 0,000 |
Serum P (mg/dl ) | 2,86±0,54 | 3,55±0,53 | 0,000 |
PTH (pg/ml) | 267,10±195,32 | 77,95±39,65 | 0,000 |
Vitamin D(µg/l) | 21,76±17,51 | 25,11±15,14 | 0,296 |
Fasting glucose (mg/dl) | 91,58±11,08 | 90,01±10,41 | 0,447 |
OGTT second hourglucose (mg/dl) | 92,28±30,86 | 81,05±24,89 | 0,001 |
Fastinginsülin (uIU/ml) | 6,66±3,82 | 6,02±3,84 | 0,448 |
OGTT second hourinsülin (uIU/ml) | 22,84±17,92 | 14,94±14,10 | 0,020 |
HOMA-IR | 1,50±0,88 | 1,36±0,91 | 0,458 |
95 - Does the presence of hurthle cells alter the distribution of Bethesda classification and outcome? - 2011
Uluslararası Bildiriler P-151, Abstracts of the 36th European Congress of Cytology, Istanbul, Turkey, 22-25 September 2011, Cytopathology, Vol:22 (Suppl 1)
ABSTRACT
OBJECTIVE: We aimed to find out whether the presence of Hurt-hle cells alters the expected Bethesda distribution and neoplasia rate.
METHOD: From 8720 FNAC reports, made between January 2009 and October 2010, cytology reports containing Hurthle or oncocytic cells were evaluated. The Bethesda distributions were noted and compared with thyroidectomies.
RESULTS: Nine hundred and fourteen patients with 953 FNACs (10.93% of total FNACs) were found. Of the 895 diagnostic nod-ules, 764 (85.36%) were benign, 86 (9.6%) AUS/FLUS, 32 (3.5%) SFN, 12 (1.34%) SFM and one (0.11%) malignant. This Bethesda distribution was different to the distribution of our 2-year diagnos- tic FNAC series without Hurthle cells (P < 0.001). This difference was due to a decrease in benign and increase in AUS/FLUS and SFN group ratios (P < 0.001 for all).One hundred and twenty-eight cases had thyroidectomy; 35 (27.3%) were neoplastic and 93 (72.7%) were benign. Among neoplastic nodules, 3 were Hurthle cell carcinoma, 8 Hurthle cell adenoma, 17 papillary thyroid carci-noma, 3 papillary microcarcinoma, 3 follicular carcinoma and 1 well-differentiated thyroid carcinoma. Twenty-two of the benign nodules were Hashimoto thyroiditis and 71 MNG with Hurthle metaplasia. On cytopathological correlation, 9.3% of benign, 46.2% of AUS/FLUS and 70.0% of SFN diagnoses had neoplastic matching nodules on thyroidectomy. On cytopathological correlation of our whole FNAC series of 2 years, neoplastic ratios of benign nodules were 6.3%, of AUS/FLUS 31.5%, and of SFN 45.0%.
CONCLUSION: We found that the distribution of Bethesda classiÞca-tion is changed when Hurthle cells are present. Benign, AUS/FLUS and SFN groups also have increased corresponding neoplastic nod-ules. According to our results, Hurthle cells in FNAC may be a mar-ker of increased incidence of neoplasia.
94 - Nodule-based cytopathological correlation of fnac and thyroidectomy - 2011
Uluslararası Bildiriler P-146, Abstracts of the 36th European Congress of Cytology, Istanbul, Turkey, 22-25 September 2011, Cytopathology, Vol:22 (Suppl 1)
ABSTRACT
OBJECTIVE: Our aim was to correlate the Bethesda classiÞcation of thyroid FNAC with thyroidectomy results.
METHOD: Between Janurary 2009 and October 2010, 582 patients had thyroidectomy. From these patients 2222 nodules had been sampled with US-guided FNAC before operation. We compared Bethesda class with histopathologic diagnosis of each corresponding nodule.
RESULTS: Among 2222 nodules in 582 patients 1136 (51.1%) were benign, 130 (5.9%) AUS/FLUS, 40 (1.8%) suspicious for follicular neoplasia (SFN), 62 (2.8%) suspicious for malignancy (SFM), 26 (1.2%) malignant and 828 (37.3%) non-diagnostic including cyst ßuids and thyoiditis. Thyroidectomy diagnosis were grouped into benign and neoplastic categories which include follicular adenoma, follicular carcinoma, Hu¬rthle cell adenoma, Hu¬rthle cell carcinoma, medullary carcinoma, papillary carcinoma, papillary microcarcino-ma, well differentiated thyroid carcinoma, well differentiated thy-roid neoplasm of uncertain malignant potential.Neoplastic lesions were found in 6.3% with benign FNAC, and 31.5% with AUS/ FLUS, 45.0% with SFN, 80.6% with SFM, 96.2% malignant and 7.9% with non-diagnostic FNAS. Forty-seven neoplastic lesions in 45 thyroidectomies did not have previous FNAC: 43 papillary mi-crocarcinomas, three papillary carcinomas and one well differenti-ated carcinoma giving an incidental malignancy rate of 7.7%.
CONCLUSION: We believe that less than expected amount of malig-nancy in our series is due to higher incidence of US-guided FNACs in our center. Our results show a malignancy risk of AUS/FLUS
93 - Prediction of neoplastic outcome in fnac containing hurthle cell using cytomorphological features - 2011
Uluslararası Bildiriler FP1-003, Abstracts of the 36th European Congress of Cytology, Istanbul, Turkey, 22-25 September 2011, Cytopathology, Vol:22 (Suppl 1)
ABSTRACT
OBJECTIVE: We investigated whether detailed cytomorphological examination differentiates benign and neoplastic nodules in pres-ence of Hu¨rthle cells.
METHOD: Between January 2009 and October 2010, 128 cases with Hu¨rthle cells in thyroid FNAC had thyroidectomy. The thyroid FNACs were reviewed for cytological features and patterns. Results were compared with thyroidectomy.
RESULTS: Presence of binuclear cells (p=0.014), macronucleoli (p=0.023), large cell dysplasia (p=0.038), small cell dysplasia (p<0.001), nuclear budding (p<0.001), increased ratio of nuclear enlargement (p=0.017), cellular discohesion (p=0.001) and Hurthle cells (p=0.004) were more in neplastic nodules. Increased colloid (p=0.015) and lymphocyte (p=0.018) ratios were more in benign nodules. Presence of capillaries, transgressing vessels, ratios of cellularity and macrophages were no different between benign and neoplastic nodules. In multivariate analyses, the likelihood of corresponding neoplastic nodules increased 4.20 times in the presence of nuclear budding (P = 0.016), 7.05 times in the presence of small cell dysplasia (P = 0.005) and 5.83 times in the presence of cellular discohesion in more than 50% of cells (p=0.033). A microfollicular-rich pattern was not observed in Hu¨rthle cell nodules but was in follicular neoplasms; a pleomorphic nuclear pattern was common in papillary thyroid carcinoma; and a macrophage-rich pattern only in multinodular goitre.
Conclusion: We found that detailed cytomorphological examina-tions are likely to predict histomorphological outcome, especially in the presence of nuclear budding, small cell dyplasia and cellular discohesion. We conclude that if clinical and radiological features are also added, histopathologic outcome of FNAC with Hu¨rthle cells can be predicted even more precisely.
92 - Follow up of aus/flus in thyroid fnac - 2011
Uluslararası Bildiriler FP1-002, Abstracts of the 36th European Congress of Cytology, Istanbul, Turkey, 22-25 September 2011, Cytopathology, Vol:22 (Suppl 1)
ABSTRACT
OBJECTIVE: We aimed to determine our atypical/follicular lesion of undetermined significance (AUS/FLUS) rate and outcome.
METHOD: Between January 2009 and October 2010, among 7658 patients with 19 569 nodules, 524 (2.7%) nodules were diagnosed as AUS/FLUS. After exclusion of patients with simultaneous nod-ules that were suspicious for follicular neoplasm or malignancy and that were malignant, 368 (4.8%) patients were diagnosed as AUS/ FLUS. These US-guided FNACs were matched with repeat FNACs and thyroidectomies.
RESULTS: Seventy-two (19.6%) of 368 patients had directly under-gone thyroidectomy for suspicious radiological or clinical features. Among these 27 (37.5%) had neoplastic nodules: five follicular adenomas, two follicular carcinomas, nine papillary microcarcino-mas, 10 papillary carcinomas and one well differentiated thyroid neoplasm of undetermined malignant potential. Seventy-four (20.1%) of 368 patients had repeated FNACs: on the second FNAC, 47 (63.5%) were benign, three suspicious for follicular neoplasm, one malignant and 23 (31.1%) non-diagnostic. None had AUS/ FLUS diagnosis on second FNAC; but two had AUS/FLUS in a third and one in a fourth. Sixteen (21.6%) of patients with repeated FNAC had thyroidectomy. All had benign or non-diagnostic nod-ules in subsequent FNACs: three were neoplastic (one papillary mi-crocarcinoma, one follicular carcinoma and one follicular adenoma) on thyroidectomy. Eight patients with second FNACs are on follow up without thyroidectomy or another FNAC. Overall 88 of 368 patients had undergone thyroidectomy and 30 (34.1%) were found to be neoplastic.
CONCLUSION: Our AUS/FLUS rate was below the expected maxi-mum. However our overall neoplastic rate of AUS/FLUS on follow up (34.1%) was higher than expected.
91 - Prevalance of gestational diabetes mellitus in patıents with gestational transient thyrotoxicosis - 2011
Uluslararası Bildiriler 35th Annual Meeting of the European Thyroid Association Abstracts, Krakow, Poland, P104, 10th-14th September, 2011,
90 - Autoimmune markers in patients with type 1 diabetes mellitus - 2011
Uluslararası Bildiriler P715, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
Introduction: Type 1 diabetes mellitus (DM) is frequently associated with other autoimmune diseases. In this study, we aimed to evaluate thyroid autoantibodies, celiac antibodies and antiparietal antibody in patients with type 1 DM.
Methods: Thyroid antithyroid peroxidase (anti-TPO) and antithyroglobulin (anti-Tg) antibodies, antiinsulin, antiislet cell and anti-glutamic acid decarboxylase (antiGAD) antibodies, antiparietal antibody, antiendomisium, antigliadin IgA and IgG antibodies were obtained from the records in patients diagnosed and followed with type 1 DM in our clinic. Also, thyroid functional status and serum vitamin B12 levels were evaluated. In available patients, thyroid ultrasonography (US) findings were recorded.
Results: One hundred and sixty-one patients with type 1 DM were included in the study. Antibodies related to type 1 DM were obtained in 117 patients and 63 (53.80%) had positive anti-GAD, 4 (3.42%) had positive antiinsulin, 13 (11.11%) had positive antiislet cell antibodies. Thyroid functions were normal in 138 (85.71%) patients, 18 (11.18%) had hypothyroidism and 5 (3.11%) had thyrotoxicosis. Anti-TPO antibody was positive in 55 (34.16%), Anti-Tg was positive in 31 (19.25%) patients, and in 58 (36.02%) patients at least one of these antibodies was positive. Thyroid US was performed in 113 patients, 59 (52.21%) had normal thyroid US findings, 49 (43.37%) had chronic thyroiditis with or without nodules, 18 (15.93%) had solitary or multiple nodules. Celiac antibodies were positive in 15 (14.42%) of 104 patients. Among 77 patients with available antiparietal antibody, it was positive in 9 (11.69%) and negative in 68 (88.31%) patients. Forty-six (28.57%) patients had vitamin B12 levels lower than 250 pg/ml.
Conclusion: Autoantibodies related to various diseases may be observed with high frequency in patients with type 1 DM. It seems reasonable to screen for concomitant thyroid diseases, celiac disease and vitamin B12 deficiency by measuring specific antibodies in a patient newly diagnosed with type 1 DM.
89 - Two cases of allergic reactions which has developed due to usage of insulin analogues - 2011
Uluslararası Bildiriler P620, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
We have presented two cases of allergic reactions developed due to usage of insulin aspart.
CASE 1: 40 years old female patient has admitted to emergency with diabetic ketoacidosis. Parenteral hydration with saline solution and insulin infusion has been given to her in ER. After ketoacidosis picture has improved, mixture of insulin asparte and insulin asparte protamine was started as maintenance therapy. After the application of second insulin dosage, itchy and erythematouspapulopustular lesions have developed all over the patient’s body. Therapy with insulin analogue was terminated immediately and human insulin was started instead. Punch biopsy was performed from the lesions. According to the pathological examination the diagnosis of Ig E mediated allergic reaction has been made. Right after corticosteroid and antihistaminic therapy was started, the lesions regressed and disappeared.
CASE 2: The second patient is 75 years old female patient who has admitted to emergency department of our hospital with hematuria, erythematous papulopustular lesions and distruption of general well being. Ten days before this clinical picture developed, intensive therapy with insulin aspart and insulin detemir had been prescribed to patient for blood sugar regulation. We have stopped analogue insulins and started human insulin. We have performed punch biopsy from the skin lesions. Biopsy result was compatible with leucocytoclastic vasculitis. We have started glucocorticoid and antihistaminic therapy immediately however the patient has died because of the concomitant acute renal failure picture.
CONCLUSION: Allergic reactions occurring due to insulin injection may present with localized or systemic reactions. Systemic allergic reactions might be IgE mediated, anaphylactic or due to IgG mediated insulin resistance or rarely it might show itself with the clinical picture of serum sickness. Although analogue insulins have reduced the incidence of immune mediated allergic reactions, clinicians still can experience few cases one in a while.
88 - A rare cause of nontraumatic rhabdomyolysis: central diabetes insipidus - 2011
Uluslararası Bildiriler P618, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
Nontraumatic rhabdomyolysis is mostly caused by drugs, alcohol consumption or compression of muscles. Severe hyperosmolarity rarely can cause rhabdomyolysis. Our case has santral diabetes insipidus that has admitted with the clinical picture of rhabdomyolysis.
CASE: 26 years old male has admitted to our clinic with the complaint of weakness, nausea, vomitting, polydipsia, polyuria, difficulty in walking and tendency to sleep. Neurologic examination was normal. In laboratory glucose:166 mg/dl, Na:168 mEq/L, Urea:19 mg/dl, Cr:1.6 mg/dl , K:2.8 mEq/L, CK:2916 IU/L, plasma osmalality 348 mosmol/L, and urine density 1005 were. Serum CK level have increased progressively up to 15000 IU/L during the follow up. We have thought that rhabdomyolysis might have been due to hyperosmolality caused by high Na and low K levels. We have administered hypotonic fluids and followed the urine output and fluid intake of the patient. His general condition was not well enough to tolerate fluid restriction test and he had severe polyuria that is why we have directly made the desmopressin administration test. Plasma osmolality was 348mosmol/L before desmopressin administration and it regressed to 330mosmol/L thereafter. Urine osmolality has increased to 330mosmol/L from 77mosmol/L after desmopressin administration. Amount of urine per hour has decreased significantly after desmopressin. Consequently the patient has been diagnosed to have central DI. In pituitary MRI a lesion was detected at the level of hypothalamus in right anterolateral neighborhood of 3rd ventricule and 14x18x11in size. It was interpreted as low grade glial lesion. Desmopressin was started po 0.1 mg three times daily and clinical picture has improved thereafter. Serum Na, K and CK levels have returned to normal values after the treatment.
CONCLUSION: Rhabdomyolysis is a rare but very important complication of hyperosmolality due to DI. CK levels should be monitor strictly in hyperosmolar states.
87 - Evaluation of autoimmune endocrine disturbances in celiac patients - 2011
Uluslararası Bildiriler P615, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
AIM: Celiac disease is closely related with other autoimmune diseases. Our purpose is to examine the existence of endocrine diseases in Celiac patients.
MATERIAL AND METHOD: Celiac patients admitted to gastroenterology clinic were referred to our endocrinology clinic between the dates of September of 2009 and June of 2010.This patient group was evaluated to see as if they had autoimmune thyroiditis, type 1 DM, primary hypoparathyroidism and primary adrenal insufficiency.
RESULTS: 27 patients were registered in our study and 6 of them (22%) were male where as 21 (77.8%) of them were female. Mean age was 35±11 years (20-61). Mean body mass index was 22.61±4.45 kg/m2 (17.9-34.9). We have detected chronic thyroiditis in 6 and type 1 diabetes mellitus in 2 of patients. All patients with endocrinopathy were female. Plasma cortisol levels were normal. We have made low dose ACTH test to all patients and the results were normal. Moreover we have detected vitamin D deficiency in 23 of the patients (85.2%) and there was secondary hyperparathyrodism in 17 of these patients. We haven’t detected primary hypoparathyroidism in any patient. In addition to endocrinopathies we have detected vitamin B12 deficiency in 13(48.1%) patients and in 3(11.1%) of them antiparietal antibody was positive.
DISCUSSION: Endocrinological pathologies especially type 1 DM, autoimmune thyroiditis, rarely Addison’s disease, chronic autoimmune hepatitis, primary billiary cirhosis, cystic fibrosis and lastly SLE have been known to accompany celiac disease. We have detected in our study group that the occurrence rate of Type 1 DM in celiac patients was 7.4% and chronic thyroiditis was 22%. We assume that periodic screening for endocrinopathies should be done in Celiac patients.
86 - A case of small cell lung cancer of which first finding is hyponatremia - 2011
Uluslararası Bildiriler P614, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
Small cell lung cancer (SCLC) is accepted as a neuroendocrine tumor and usually accompanied with paraneoplastic syndromes. Our case has been diagnosed as SCLC and the only finding of disease was hyponatremia.
CASE: 44 years of female patient has admitted because of nausea, vomitting and fatigue. Serum Na level was 116 mEq/L. The patient hospitalized for further investigation. In physical examination BP was 140/80 mmHg, HR was 72 beats/min. Patient didn’t have complaints such as coughing, sputum, weight loss, dispnea or chest pain. Serum glucose level 101 mg/dl, urea 9 mg/dl, Cr: 0.6 mg/dl and K: 4.1mEq/L were. Plasma osmolality was measured as 226 mosm/L, urine osmolality was 306 mosm/L, urine dansity was 1013 and Na in 24 hour collection of urine was 147 mmol/ L. In imaging of brain with MRI there were hyperintense lesions located in white matter which were interpreted as finding of encephalomyelitis or demyelinating disease. It could be related to hyponatremia. In abdominal MRI images adrenal glands were normal. Plasma cortisol and 17-OH Progesterone responses to short ACTH stimulating test, pitiutary hormones, cortisol and growth hormone response to insulin tolerance test were normal. We thought all these results could be due to SIADH. In thorax CT we have detected multiple nodules biggest 6mm in dimension and multiple enlarged hilar and mediastinal lymph nodes biggest in 23 mm in size. Endobronchial biopsy was taken from the enlarged lymph nodes Histopathology results were compatible with SCLC metastasis and patient was referred to an oncology clinics.
SIADH syndrome occurs in oncology patients due to ectopic production of hormone by cancer itself, complications or treatments. Early recognition of it is important in order to reduce morbidity and mortality. It should be kept in mind that hyponatremia might be first sign of cancer as it is in our case.
85 - Suspected parathyroid lesions and incidentally detected parathyroid adenomas during thyroid ultrasonography - 2011
Uluslararası Bildiriler P506, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
Introduction: Although incidentalomas in endocrine glands such as pituitary, adrenal or thyroid are well defined, parathyroid incidentaloma is a rare concept. In this study, we aimed to determine the prevalence of suspicious parathyroid lesions and true parathyroid incidentalomas in patients referred for thyroid ultrasonography (US) and investigate the possible factors that might cause inadvertent suspicion of a parathyroid adenoma.
Methods: Patients suspected to have parathyroid lesions during thyroid US were recorded prospectively between August 2009 and January 2010. Patients referred for parathyroid US and patients with known high serum calcium or parathyroid hormone (PTH) levels were excluded. Suspected parathyroid lesions were defined as hypoechoic homogeneous solid lesions with regular margins located outside the thyroid lobe, most commonly inferior to the thyroid gland.
Results: Thyroid US was performed in 6528 patients during the study period. There were 78 patients (1.19%) (73 female and 5 male) with suspected parathyroid lesion and the mean age was 45.32±12.59. The diagnosis of a true parathyroid adenoma was confirmed six (7.69%) patients. Mean serum calcium, phosphorus and PTH levels were 10.57±0.48 mg/dl, 3.03±0.52 mg/dl and 182.91±46.62 pg/ml respectively in patients with true adenoma. Among 72 patients with false positive parathyroid lesion, antithyroid peroxidase antibody was positive in 50 (69.4%), antithyroglobulin antibody was positive in 46 (63.9%) and one of these antibodies were positive in 59 (81.9%) patients. Also, 46 (63.9%) of 72 patients had thyroid dysfunctions (43 hypothyroidism and 3 hyperthyroidism) and 59 (81.9%) had chronic thyroiditis ultrasonographically.
Conclusions: Parathyroid incidentaloma was detected in 0.09% of patients referred for thyroid US. Presence of clinically or ultrasonographically chronic thyroiditis seems to be the major factors related to inadvertent interpretation of a hypoechoic lesion as a parathyroid pathology during thyroid US. Most of these lesions are probably lymphadenopathies that may occur commonly in patients with chronic thyroiditis.
84 - Serum 25-OH Vitamin D levels in patients with benign and malignant thyroid nodules - 2011
Uluslararası Bildiriler P460, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
Introduction: Increased exposure to sunlight and high serum levels of Vitamin D were reported to relate with decreased risk of various cancer types, such as prostate, breast and colon. Vitamin D receptor and 1α-hydroxylase expression were shown in papillary thyroid carcinoma. In this study, we aimed to evaluate serum 25-OH vitamin D levels in patients with benign and malignant thyroid nodules
Methods: Patients admitted to our thyroid clinic were recruited for the study. Thyroid ultrasonography and serum 25-OH vitamin D measurement were done in all patients and controls. Because serum 25-OH vitamin D levels may change with seasons, blood samples were taken in April-May 2009 and 2010. Results were compared in patients with histopathologically proven thyroid papillary cancer, patients with histopathologically or cytologically proven benign thyroid nodules and patients without thyroid nodules. Patients with diseases related to bone metabolism and thyroid dysfunctions were excluded.
Results: There were 31 patients with histopathologically proven papillary thyroid cancer, 128 patients with cytologically or histopathologically proven benign nodules and 269 patients without any nodule. Of 428 subjects, 360 (84.1%) were female and 68 (15.9%) were male and sex distibution were similar in three groups (P=0.079). Mean serum 25-OH vitamin D levels were 16.91±10.42, 16.35±9.02 and 17.19±10.74 μ/l in malignant, benign and control groups, respectively (P=0.746). Including all subjects, although mean serum vitamin D levels were higher in males compared to females, the difference did not reach statistical significance.
Conclusion: Serum 25-OH vitamin D levels, here in this study, were shown not to differ in patients with benign nodules, malignant nodules and patients without nodules. Possible effect of vitamin D metabolism and receptors on thyroid papillary cancer that was suggested in previous in vitro and in vivo studies seems to be independent from serum 25-OH vitamin D levels.
83 - Classical and follicular variant papillary thyroid carcinoma: comparison of clinical, ultrasonographical, cytological and histopathological features in 402 patients - 2011
Uluslararası Bildiriler P459, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
Introduction: Follicular variant papillary thyroid carcinoma (FVPTC) is the most common variant of papillary thyroid carcinoma (PTC) after classical PTC (CPTC). In this study, we aimed to compare functional status, ultrasonographical features, cytological results and histopathological characteristics of patients with CPTC and FVPTC.
Methods Patients: Diagnosed with CPTC and FVPTC in our clinic were reviewed retrospectively. Data of preoperative thyroid functional status, thyroid autoantibodies and ultrasonographical features were obtained from the records. Sensitivity of fine needle aspiration biopsy (FNAB) was calculated and histopathological features were compared in two variants.
Results: There were 322 (80.1%) CPTC and 80 (19.9%) FVPTC patients and sex distribution, mean age, thyroid functions and autoantibody positivity rates were similar. 228 CPTC and 62 FVPTC patients had preoperative US examination. Echogenicity, texture, presence of microcalcifications and macrocalcifications were similar in two groups. A hypoechoic halo was observed more frequently (15.4 vs 29%, P=0.012) and marginal irregularity was observed less commonly (81.6 vs 67.7%, P=0.018) in FVPTC lesions. Among 261 CPTC and 73 FVPTC patients with preoperative FNAB results, rate of malignant cytology was significantly higher in CPTC (37.2 vs 19.2%, P=0.004) and rate of suspicious cytology was significantly higher in FVPTC (35.6 vs 53.4%, P=0.006). When only malignant cytology was treated as true positive, sensitivity of FNAB in CPTC and FVPTC was 37.2 and 19.2%, respectively (P=0.004). Mean tumor diameter was markedly higher in FVPTC compared to CPTC (16.04±13.44 vs 10.88±9.88 mm, P<0.001). There was no difference in terms of multicentricity, capsule and vascular invasion, extrathyroidal involvement and lymph node invasion.
Conclusion: FVPTC tends to have more benign features in US and less malignant results in cytology. Higher tumor size in FVPTC compared to CPTC might be explained by the recognition of clinical importance of these lesions after reaching particular sizes due to benign US features.
82 - Cytological evaluation of pyramidal lobe and thyroglossal duct cysts - 2011
Uluslararası Bildiriler P406, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
AIM: Thyroid pyramidal lobe and thyroglossal duct cysts were reported to be associated with increased risk of thyroid cancer. In this study, we aimed to evaluate ultrasonography (US) guided fine needle aspiration biopsy (FNAB) cytology results of pyramidal lobe and thyroglossal duct cysts.
MATERIAL AND METHODS: Patients with pyramidal lobe and thyroglossal duct cysts detected in US were included. Thyroid functions, thyroid autoantibodies, Tc 99m thyroid scintigraphy and US guided FNAB cytology results were evaluated
RESULTS: There were 79 (97.5%) female and 2 (2.5%) male patients with a mean age of 52.0±12.3 (20-82). Thyroglossal duct remnant was observed in 26 (32.1%) and pyramidal lobe in 55 (67.9%) patients. There were 74 (91.4%) patients with a previous history of thyroidectomy and all were histopathologically benign. In 7 patients, there was not a history of thyroid operation. FNAB results of all thyroglossal duct and pyramidal lobe were benign
CONCLUSION: Pyramidal lobe is an embryological remnant of thyroglossal duct and its incidence varies between 15-75% in surgical and autopsy series. It was reported that this tissue becomes hypertrophic under the influence of increased thyrotrophin in thyroidectomized patients. Thyroglossal duct cysts develop in front of the neck. Increased risk of occult malignancy risk was reported in solid lesions, particularly when they include ectopic thyroid tissue. In our series, we did not observe any malignant cytology result.
81 - Comparison of GH suppression response after oral and intravenous glucose tolerance tests in healthy subjects - 2011
Uluslararası Bildiriler P230, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
Introduction: In this study, we aimed to compare GH values obtained in oral glucose tolerance test (OGTT) and intravenous glucose tolerance test (IVGTT) in healthy individuals.
Material and methods: Data of 18 healthy volunteers were analysed (10 male and 8 female). Firstly all subjects were evaluated with 75 g oral glucose tolerance test. In another day, intravenous glucose tolerance test was performed. Serum glucose, insulin and GH levels obtained during two tests were measured.
Results: Basal GH levels had a wide distribution ranging from 0.00005 μg/l (0.05 pg/ml) to 0.768 μg/l (768.92 pg/ml) (median 0.0145 μg/l). Mean nadir GH level during OGTT was 0.0376 μg/l (between 0.00011 and 0.387, median 0.0016, S.D.: 0.095, S.E.M.: 0.038) and it was obtained at 60th minute. Nadir GH level during IVGTT was observed at 10th minute and it was 0.112 μg/l (between 0.0005 and 0.770, median 0.0053, S.D.: 0.242, S.E.M.: 0.057). There was statistically significant difference between GH levels at 10th minute in IVGTT and at 60th minute in OGTT (Z=2.201, P=0.028). GH level at 10th minute in IVGTT was higher than GH level at 60th minute in OGTT.
Conclusions: Effect of gastroenteropancreatic pathway which may show individual differences can be eliminated by IVGTT. GH suppression by IVGTT may be used in the diagnosis and follow-up of patients with acromegaly. Higher nadir GH levels in IVGTT indicates that nadir GH levels suggested for remission in acromegalic patients are relatively low. Our results show that there may be need to revise the remission criteria for acromegaly.
80 - Prevalence of thyroid pathologies in patients with polycystic ovary syndrome - 2011
Uluslararası Bildiriler P92, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
Introduction: Polycystic ovary syndrome (PCOS) is a common disorder characterized by chronic anovulatory oligo-amenorrhea and signs of hyperandrogenism. In this study, we aimed to determine prevalence of thyroid nodules and autoimmune thyroid diseases in patients with PCOS.
Methods: Patients diagnosed with PCOS in our endocrinology clinic were included in the study. In patients with irregular menses and/or hirsutism, the diagnosis of PCOS was made by high serum LH/FSH ratio, high serum free testesteron levels and/or polycytic ovaries in pelvic ultrasonography. Serum thyrotropin, free thyroid hormones, antithyroid peroxidase (AntiTPO) and antithyroglobulin (AntiTg) antibody levels were evaluated. Thyroid ultrasonography was performed in all subjects by the same examiner. Thyroid fine needle aspiration biopsy (FNAB) was carried out when indicated.
Results: There were 107 women with PCOS with a mean age of 23.96±5.70. Seventeen (15.9%) patients had hypothyroidism and 2 (1.8%) had hyperthyroidism. 30.5% patients had positive AntiTPO, 30.5% had positive AntiTg and 37.8% had positive AntiTPO or AntiTg antibodies. Thyroid nodules were detected in 29 (27.1%) patients, 10 had solitary and 19 had multiple nodules. FNAB was performed in 11 patients with nodules; 10 were cytologically benign and 1 was malignant (papillary thyroid carcinoma was confirmed histopathologically). Totally, in 54 (50.5%) patients, there was a thyroid related disease such as positive thyroid antibodies, thyroid dysfunctions or nodules. Insulin resistance calculated with HOMA-IR was ≥2 in 47 (43.9%) and <2 in 60 (56.1%) patients. Nodule prevalence, thyroid dysfunctions, thyroid autoantibody positivity and thyroid volume did not differ between PCOS patients with and without insulin resistance.
Conclusion: Thyroid pathologies are observed in half of the patients with PCOS. Measurement of thyroid hormones are usually a part of investigation in PCOS patients, but we think serum thyroid autoantibodies and presence of thyroid nodules should also be searched in these patients.
79 - Intranodular glucose levels ın the dıfferentıal dıagnosıs of thyroıd nodules: a prelımınary study - 2011
Uluslararası Bildiriler P179, 35th Annual Meeting of the European Thyroid Association Abstracts, Krakow, Poland, 10th-14th September 2011
ABSTRACT
INTRODUCTION: Recent studies have shown that GLUT-1 expression in malignant cells increases favoring the increase of glucose in to the cells. Detecting intranodular glucose amount might predict malignancy of the thyroid nodule. The aim of this study was toevaluate the glucose content of thyroid nodules during USG guided fine needle aspiration biopsy (FNAB).
SUBJECTS AND METHODS:
Study population
42 patients with suspicious thyroid nodules were selected from our Thyroidout patient clinic who were to undergo Ultrasound-guided FNAB. All these patients underwent total thyroidectomy and confirmed thyroid papillary carcinoma histopathologically.
US and US guided FNAB
Ultrasonography was performed using Esaote color Doppler US(MAG Tecnology Co,Ltd.Model :796FDII Yung-ho City,Taipei Taiwan) and superficial probe (Model No:LA523 13-4, 5,5-12,5 MHz ) for the evaluation of nodules in the thyroid gland. US guided FNAB was performed using a General Electiric Logiq pro 200(Model number 2270968, GE Healtcare Korea, Seongnam -SI, Gyean GGI-DO ,Korea) and a 5,5-7,5 MHz probe was used. FNAB was performed on an extended neck using a 27 gauge needle. The needle was connected to a 2 ml syringe. After the aspiration, the aspirate was expelled onto glass slides and smeared for cytological examination. The sample needle was not thrown. Instead the remaining in the needle was rinsed three times with 250 µl normal saline and the washout was placed in an epandorph tube for glucose measurement. After FNAB procedure, a blood sample was taken from the brachial vein of the patient via a syringe and needle similar to the one used in FNAB. Than the syringe was changed with another syringe with the same properties and the blood sample was expelled out. The remaining blood in the syringe was diluted with 250 µl normal saline. All these procedures were also applied to the serum of the patient. For each patient there were four different samples in which glucose was to be studied.
The results were compared with the patients’ venous blood glucose level, cytological and/or histopathological diagnosis to see if there was any relationship.
RESULTS: Glucose content of 42 nodules of 42 patients was investigated. On cytological examination 21 of 42 nodules had benign, 8 nodules had malignant (proven histopathologically), and 13 nodules had nondiagnostic cytology. One patient atypical cells on cytological examination and refused operation. The cytological evaluation of 5 of the nodules with indeterminate cytology revealed colloidal material only, 8 nodules revealed colloidal material with a few benign follicular epithelial cells. The ratio of serum glucose level/glucose content of the nodule which had benign, malign and indeterminate cytological results were 64.00±24.00, 52.02±22.00, 67.00±27.70 respectively (p=0,371). Although not statistically significant the ratio of serum glucose level/glucose content of the malign nodules were lower than the other groups suggesting that the intranodular glucose content was higher than serum glucose content in this group. There was no relationship between the ratio of serum glucose level/glucose content of the nodule and anti TPO and anti Tg levels (p=0,199 and p=0,202 respectively). Also there was no difference between the ratio of serum glucose level/glucose content of the nodule and the content (solid, partially cystic) between the 3 groups (p=0151).
CONCLUSION: By measuring intranodular glucose content we have for the first time made an initial effort to evaluate the clinical significance of intranodular glucose content and to see if it there is any difference between malignant, benign and nondiagnostic nodules. Here in this study although our study population is small and the results are not statistically significant malignant nodules have higher glucose levels. It may be possible to predict if a nodule is weather benign, malign or nondiagnostic by looking immediately during FNAB. We think that this may be a new technique in the follow up of thyroid nodules and needs further investigation with a larger patient group with more standardized methods.
78 - Metabolic syndrome parameters and ınsulın resıstance ın dıfferentıated thyroıd cancer - 2011
Uluslararası Bildiriler P167, 35th Annual Meeting of the European Thyroid Association Abstracts, Krakow, Poland, 10th-14th September 2011
ABSTRACT
INTRODUCTION: The incidence of thyroid cancer is increasing parallel with the incidence of metabolic syndrome. One of the reasons for the increased incidence of thyroid cancer all over the world might be insulin resistance. The purpose of this study was to investigate the incidence of metabolic syndrome and insulin resistance in patients with differentiated thyroid cancer (DTC).
SUBJECTS AND METHODS: Fourty-one patients between the ages of 18-65 with DTC were included in the study. Forty one patients operated because of eutyhroid nodular or multinodular goitre and pathology benign were chosen as the control group. Blood samples were taken after an overnight fasting from an antecubital vein between 08.00 h and 10.00 h at resting position. Measurements were done before operation and when patients were euthyroid in patient group. Fasting plasma glucose (FPG), insulin, thyrotropin (TSH), free triiodothyronine (FT3), free thyroxine (FT4), total cholesterol, high density lipoprotein (HDL) and triglyceride (TG) measurements were done in all cases. Weight, height, body mass index (BMI) and body fat ratio was determined. Homeostatic model assessment (HOMA) index was used to evaluate insulin resistance. Patients with HOMA-IR>2.5 were accepted to have insulin resistance.
RESULTS: Mean age, sex distribution, height, weight, waist circumference and BMI were similar in two groups. Fourteen (34.1%) patients in each group met metabolic syndrome criteria. Insulin resistance evaluated with HOMA-IR was similar in two groups (p=0.80). Mean TSH was significantly higher in Group 2 compared to Group 1 (p=0.02), while fT3 and fT4 did not differ between groups. However, high TSH was determined as a risk factor for DTC with an Odds ratio of 0.581 in 95% confidence interval (p=0.029). Presence of metabolic syndrome was determined as a risk factor for DTC with an Odds ratio of 0.227 in 95% confidence interval (p=0.047). There was no statistically significant difference in terms of HOMA-IR between patients with microcarcinoma and macrocarcinoma (p=0.08).
CONCLUSION: In this study, the first time in the literature we evaluated prevalence of insulin resistance and metabolic syndrome preoperatively in euthyroid patients with DTC. HOMA-IR wassignificantly higher in patients with DTC compared to control group. However, HOMA-IR was similar in patients with microcarcinoma and macrocarcinoma. Our results suggest that patients with thyroid nodules should be evaluated for the presence of insulin resistance and metabolic syndrome which may be considered as modifiable risk factors for thyroid cancer.
Table1. Demographic, anthropometric and laboratory data of study group
Patients Group 1 N=41 | Control Group 2 N=41 | p | |
Age (year) | 43,73±10,37 | 47,34±10,91 | 0,12 |
Weight (kg) | 77,80±21,11 | 76,59±13,94 | 0,75 |
Height (cm) | 160,56±8,09 | 160,12±7,88 | 0,80 |
Waist (cm) | 94,24±15,96 | 92,54±13,69 | 0,59 |
BMI | 30,19±7,65 | 30,08±6,35 | 0,94 |
FAT (%) | 39,84±10,63 | 40,53±10,21 | 0,76 |
FPG | 93,56±10,85 | 90,80±15,33 | 0,35 |
Insulin | 9,01±4,88 | 7,73±4,32 | 0,21 |
HOMA-IR | 2,52±2,22 | 1,76±1,07 | 0,053 |
fT3 | 2,98±0,53 | 3,03±0,54 | 0,63 |
fT4 | 1,25±0,46 | 1,17±0,37 | 0,37 |
TSH | 1,51±1,19 | 2,08±1,10 | 0,02 |
Total Kol (mg/dL) | 201,20±46,42 | 188,15±36,23 | 0,16 |
TG | 132,54±65,66 | 123,83±57,49 | 0,52 |
HDL Kol (mg/dL) | 52,44±12,80 | 51,62±17,71 | 0,81 |
77 - Prevalance of gestatıonal dıabetes mellıtus ın patıents wıth gestatıonal transıent thyrotoxıcosıs - 2011
Uluslararası Bildiriler P104, 35th Annual Meeting of the European Thyroid Association Abstracts, Krakow, Poland, 10th-14th September 2011
ABSTRACT
Objective: In this study, we aimed to determine prevalence of gestational diabetes mellitus (GDM) in patients with gestational transient thyrotoxicosis (GTT) and investigate the relation between GTT and anthropometric measurements and biochemical parameters
Methods: Fifty two pregnants with GTT (18-42 years old) and 100 healthy pregnants (19-37 years old) were included in the study. Weight, height and body mass index (BMI) were meaured and fasting plasma glucose (FPG), uric acid, LDL-cholestereol, HDL-choloesterol, triglyceride (TG), hemoglobin Alc (HbA1c), thyroid stimulating hormone (TSH), free thyroxine (FT4), free triiodothyronine (FT3), anti-thyroid peroxidase antibody (Anti-TPO), anti-thyroglobulin antibody (Anti-Tg), TSH receptor antibody (Trab) were studied in all subjects. Conventional thyroid ultrasonography was performed. After basal and first hour glucose were evaluated with 50 gram oral glucose tolerance test (OGTT) at the 24-28th gestational weeks, all subjects were also evaluated with 100 gram OGTT in the following week.
Results: Mean age of 52 GTT pregnants was 28.46±5.45 and BMI was 21.66±2.92 kg/m2. Mean age and BMI of 100 healthy pregnants were 26.17±3.75 and 21.12±1.48kg/m2, respectively. Age, BMI, FPG, TG and uric acid were similar in GTT and healthy pregnants (p>0.05). We found significantly higher HbAlc, LDL-cholesterol and HDL-cholesterol in GTT pregnants (p< 0.001, p< 0.001 and p=0.034, respectively). 50 gram OGTT was positive in 14 (26.9%) GTT pregnants and in 10 (10%) healthy pregnants (p=0.01). TSH was significantly lower in pregnants with positive 50 gram OGTT compared to pregnants without glucose intolerance (p=0.001). Also, pregnants with both positive 50 gram and 100 gram OGTT (n=9) had lower TSH compared to pregnants without glucose intolerance, but the difference was not statistically significant (p>0.05).
Conclusion: GTT is a transient abnormality that can be seen in the early periods of pregnancy. However, like other hyperthyroidism states, it seems to have effect on carbohydrate metabolism later in pregnancy.
76 - Comparıson of early total thyroıdectomy wıth antıthyroıd treatment ın patıents wıth moderate to severely actıve graves’ orbıtopathy, a randomızed prospectıve trıal - 2011
Uluslararası Bildiriler OP45, 35th Annual Meeting of the European Thyroid Association Abstracts, Krakow, Poland, 10th-14th September 2011
ABSTRACT
Objectives: We aimed to compare early total thyroidectomy with the anti-thyroid treatment regimens, in patients with moderate to severely active Graves' orbitopathy (GO) prospectively.
Methods: The inclusion criteria: Hyperthyroidism and GO developed in the last six months, thyroid volume ≥15 mL, no previous treatment except local interventions for GO. GO activity has been defined as clinical activity score (CAS) ≥3 and carrying at least one of the following criteria; Proptosis ≥21 mm in one eye, ≥2 mm difference between two eyes, presence of diplopia, lid aperture ≥9 mm. Initially, all the patients were made euthyroid (TSH 0.4-1 mlU/L). Pulse methylprednisolone of total 4.5 gr were given intravenously to all patients before randomization. In the first group, patients were sent to total thyroidectomy and TSH levels were kept within 0.4-1 mlU/L with levothyroxine. Second group of patients were followed with anti-thyroid drugs and with the addition of levothyroxine, when necessary, to keep TSH within 0.4-1 mlU/L.
Results: 12 patients were randomized to total thyroidectomy (TT) group and 11 patients were randomized to medical antihyroid treatment (AT) group. There were no difference between the two groups with respect to age, gender, smoking habit, duration of hyperthyroidism and GO, thyroid volume, TSH, free T4, anti-TPO, anti-Tg and TRAb levels initially. When the TT group was compared with AT group, thyroid antibodies were significantly decreased in TT group while there was no significant difference with respect to proptosis, lid aperture, CAS and diplopia between groups. However in TT group additional pulse methylprednisolone treatment was given to 3 (25%) patients and urgent orbital decompression was applied to 2 (17%) of those patients.
Conclusion: Although the significant decrease of thyroid autoantibodies were achieved in TT group, this was not reflected as an beneficial effect on the course of GO during the 15 months follow-up period.
75 - Comparison of Early Total Thyroidectomy with Antithyroid Treatment in Patients with Moderate to Severely Active Graves’ orbitopathy, Preliminary Results of a Randomized Prospective Trial - 2010
Uluslararası Bildiriler 14th International Thyroid Congress, Paris, France, 11-16 September, Final Programme, www.itc2010.com, OC-076, 2010
ABSTRACT
Aim: We aimed to compare early total thyroidectomy performed within six months of Graves' orbitopathy (GO) with the anti-thyroid treatment, in patients with moderate to severely active GO prospectively and evaluate the clinical course of eye disease.
Materials and Methods: The patients with moderate to severely active GO were enrolled in the study fulfilling the following criteria: Hyperthyroidism and GO developed in the last six months, thyroid volume ≥15 ml, no previous treatment except local interventions for GO. GO severity has been defined as clinical activity score (CAS) ≥3 with at least one of the following criteria; Proptosis ≥21 mm in one eye, ≥2 mm difference between two eyes, presence of diplopia , lid aperture ≥9 mm. Initially, all patients were made euthyroid with anti-thyroid drugs and TSH levels were kept within the range 0.4-1 mlU/L. Pulse methytprednisolone of total 4.5 gr was given intravenously to all patients before randomization to two groups. In the first group, patients were sent to total thyroidectomy and their TSH levels were kept within the range 0.4-1 mlU/L with levothyroxine (LT4). Second group of patients were followed with fixed dose (20-50 mg) of anti-thyroid drugs and with the addition of LT4, when necessary, to keep TSH within the range 0.4-1 mlU/L. Patients were asked for smoking habits, family history of GO. CAS, proptosis, lid aperture and diplopia were evaluated. TSH, freeT4, TSH receptor antibody (TRAb), anti-TPO and anti-Tg levels were measured. These are the preliminary results of the study ongoing for more than 12 months
Results: 12 patients with a mean age of 44±8.7 years were randomized to the total thyroidectomy (TT) group and 10 patients with a mean age of….
74 - The effect of the menstrual cycle, a sample of infradian rhythm on thyroid volume and blood flow in healhty women - 2010
Uluslararası Bildiriler 14th International Thyroid Congress, Paris, France, 11-16 September, Final Programme, www.itc2010.com, P-0797, 2010
ABSTRACT
INTRODUCTION: Previous studies has shown that thyroid blood flow varies cyclically during the normal menstrual cycle in females of reproductive age and that thyroid physiologic characteristics change during different reproductive phases of a woman’s life. The aim of this study is to evaluate the changes in thyroid stimulating hormone (TSH) levels through four different periods of menstrual cycle which is a sample of infradian rhythm; and to investigate the relationship between thyroid volume and doppler parameters of inferior thyroid artery according to TSH and sex hormone alternations in healthy women.
MATERIALS AND METHODS: Twenty-two healthy women having regular menstrual cycles between 21 and 38 years were included in this study. Each participant was evaluated at the 3rd day (menstrual bleeding period), 7th day (follicular phase), 14th day (periovulatory period) and 21st day (luteal phase) of their menstrual cycle. All examinations were performed after a 12 hours fasting time, between am 06:00- 08:00. Blood samples were collected for plasma estradiol (E2), progesterone (PG), luteinizing hormone (LH), follicle stimulating hormone (FSH), thyroid-stimulating hormone (TSH), free triiodothyronine (fT3), free thyroxine (fT4), thyroglobuline (Tg).Conventional ultrasonography and power doppler ultrasonography were carried out(Figure 1).
RESULTS: Mean age of these 22 women was 28,72±5,72 years. The statistical alternations of the mean values of TSH, Tg, peak systolic velocity (PSV), resistance index (RI), pulsatility index (PI) and thyroid volumes at the 3rd day, 7th day, 14th day and 21st days of menstrual cycle were examined. It was detected that there was a statistically significant in TSH, thyroid volume and PSV at the 14th day compared to the 3rd and 7th days(Table 1). With a minimal increase at the 21st day; any statistically significant change could not be found in PI values during menstrual cycle. Compared with the 3rd day; there was a statistically significant decrease in RI value at the 14th and 21st days. Also compared to the 3rd day; there was a statistically significant increase in Tg levels at the 7th and 14th days. During menstrual cycle, there was no significant change in fT3 and fT4 levels. In addition; during this period, no statistically significant correlation was detected between TSH levels and LH, FSH, PG, E2, Tg levels; and yet between TSH levels and PSV, RI, PI, thyroid volume..
CONCLUSION: Through menstrual cycle; with thyroid volume, TSH, and Tg, also some changes occur in blood flow parameters of inferior thyroid artery. Power doppler measurements are used for differential diagnosis of certain thyroid diseases. In this case; we believe that it is appropriate to evaluate the female patients during the follicular phase while performing doppler or population studies.
Figure 1. The velocity waveform is displayed above the baseline to indicate the arterial blood flow. The figure shows the measurement of the blood flow velocity in the inferior thyroid artery (left).
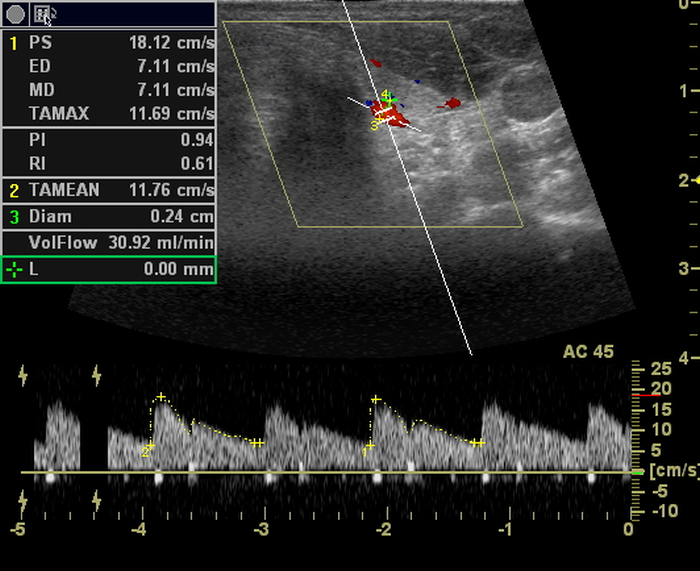
Figure 2.Changes of mean values of RI, PI and TSH at the 3rd, 7th, 14th and 21st days of menstrual cycle
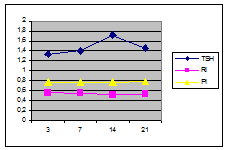
Figure 3. Changes of mean values of thyroid volume and PSV at the 3rd, 7th, 14th and 21st days of menstrual cycle
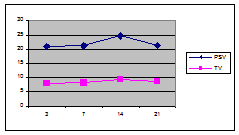
Table 1. Statisticallyalternations of the mean values of TSH, Tg, PSV, RI, PI and thyroid volumes at the 3rd, 7th, 14th and 21st days of menstrual cycle
Days of MS | 3rd vs 7th p | 3rd vs 14th p | 3rd vs 21st P | 7th vs 14th P | 7th vs 21st P | 14th vs 21st p |
TSH Tg PSV RI PI Volume fT4 fT3 | 0,01 0,001 NS NS NS NS NS NS | 0,005 0,021 0,014 0,002 NS 0,000 NS NS | NS NS NS 0,015 NS 0,062 NS NS | 0,021 NS 0,021 NS NS 0,002 NS NS | NS NS NS NS NS NS NS NS | NS 0,001 0,005 NS NS 0,011 NS NS |
73 - Thyroid abscess in a patient with diabetes mellitus - 2010
Uluslararası Bildiriler 14th International Thyroid Congress, Paris, France, 11-16 September, Final Programme, www.itc2010.com, P-0585, 2010
ABSTRACT
INTRODUCTION: Thyroid gland abscess is an uncommon condition, with fewer than 300 cases reported in the literature. Its rarity is attributed to the remarkable resistance of the thyroid gland to infections because of its protective mechanisms, which include a rich blood supply, goodlymphatic drainage, high iodine content, and the protective capsule surrounding the gland. The most common mechanism of thyroid infection is transmission of an infection via a pyriform sinus fistula. We report the case of thyroid abscess in a patient with Type 2 Diabetes Mellitus (DM).
CASE: A 65 years old male patient with Type 2 DM admitted our out-patient clinic with the complaint of tiredness, high blood sugar and swelling in right side of the neck. He was on oral antidiabetic treatment and his glucose levels couldn’t be regulated since two months. His blood pressure was 110/70 mm Hg, heart rate was 81 beats /min and his temperature was 36.80°C. On physical examination, a 1x2 cm nodule was found on the right thyroid lobe. Thyroid ultrasonography revealed a nodule cystic in appearance with a solid component at the right lobe. In laboratory examination, serum TSH, fT3 and fT4 were in normal ranges. The thyroglobulin antibody and thyroid proxidase antibody tests were negative. In cytologic evaluation, needle aspiration of the drained 2 ml pus showed a large number of polymorphonuclear leukocytes. There were no microorganisms on microscopic examination and no growth on culture. Tuberculosis DNA PCR was negative. High sensitive CRP, ESR and leukocyte count was in normal limits. Baryum esophagogram was normal, no fistula could be determined. Two months after the diagnosis total thyroidectomy was performed and histopathological examination revealed chronic inflammatory reaction surrounding the right thyroid nodule with fibrosis. No microorganism could be identified. The patient was diagnosed as a sterile and restrained thyroid abscess with unknown origin.
DISCUSSION: In our case the patient was diabetic and his blood sugar was not regular. This may have made the patient prone to infection. There are several routes of spread of infection to the thyroid gland. Many sources have been reported including hematogenouse and lymphatic spread, direct penetration from adjacent structures, neck injuries. The most frequent reason of thyroid abscess is congenital pyriform sinus fistula. If thyroid abscess is not diagnosed and treated quickly, septicemia, retropharengeal abscess, tracheal or esophageal rupture, suppurative mediastinitis can be occur. In the peresent case the pus obtained by FNAB from the nodule showed no microorganisms on microscopic examination and no growth on culture. Tuberculosis DNA PCR was also negative. A prime cause of infection could’nt be found. Our case was followed for 2 months. An antibiotic therapt was initiated but there was no change in size of the nodule. None of the inflammatory markers were elevated during this period. Although some of the authors donot recommend thyroidectomy, it was the only treatment choice.This case is reported because of the rarity of the condition.
Figure 1. Cytologic evaluation: Abscess formation with colloid material, hystiocytes and polymorphonuclear leucocytes. X400 Giemsa
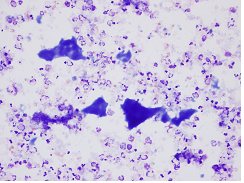
Figure 2. Histopathologic evaluation: Chronic inflammation and fibrosis surrounding on ruptured colloid nodule. X40 HE
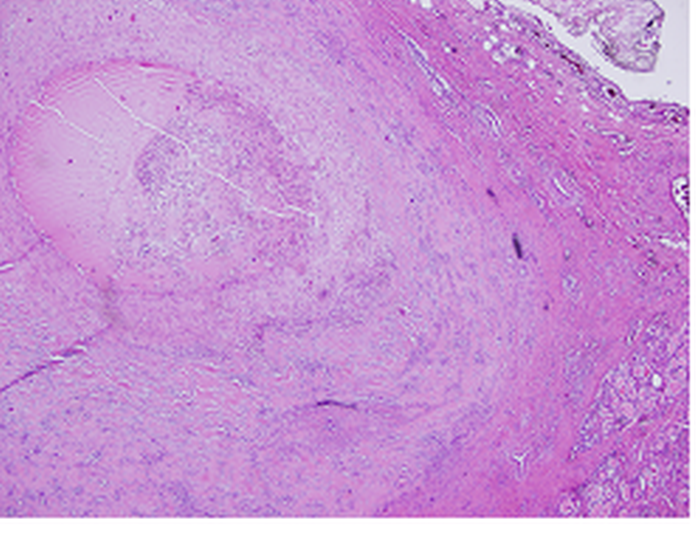
72 - Esophageal squamous cell carcinoma metastasis to the thyroid gland: Case report - 2010
Uluslararası Bildiriler 14th International Thyroid Congress, Paris, France, 11-16 September, Final Programme, www.itc2010.com, P-0584, 2010
ABSTRACT
INTRODUCTION: The thyroid gland is not an uncommon organ for metastatic spread from distant neoplasms at autopsies, but it is rare to be found in clinical situations. It has been reported that <2% of clinically detectable thyroid cancers are of metastatic origin. The most common malignancies that metastasis to the thyroid are melanoma, renal cell carcinoma, breast carcinoma, lung carcinoma and head and neck carcinomas. Although metastases from gastrointestinal tract malignancies are unusual, the majority of them are from esophageal or colonic primary. To our knowledge, there are only 5 cases of esophageal carcinoma with thyroid gland metastases in the literature. We present a new case of esophageal squamous cell carcinoma metastases to the thyroid gland.
CASE: A 57-year-old male patient was admitted for evaluation of an enlarged mass on the right neck, which was just noticed by the patient. There was no history of previous irradiation to the neck or chest. No associated symptoms of neck pain, dysphagia, or hypo or hyperthyroidism were identified. On physical examination, a nontender, well-circumscribed, 2.0 cm nodule was found on the right thyroid. The patient was clinically euthyroid. The thyroglobulin antibody and microsomal antibody tests were negative. Serum thyroglobulin and calcitonin levels were within normal limits. Ultrasonography revealed hypoechoic nodules on the right and left thyroid and lymph nodes with microcalsifications in the right cervical region of the neck (level III). Ultrasound guided fine needle aspiration cytology from the nodules and lymph nodes revealed the presence of a metastatic squamous cell carcinoma. On neck computed tomography (CT) there was 30 mm lesion in the subcarinal localization which deplased the esophagus to the right(Figure1).On thorax CT, there were multiple metastatic noduler lesions. An esophagogastroduadenoscopy revealed a lobulated lesion in the cervical esophagus distal to the vocal cords. Cytological assessment from multiple biopsies confirmed an esophageal squamous cell carsinoma. The extent of the disease didn’t allow surgery. The patient is currently undergoing chemoradiation. In this report, we present an unusual case of metastatic squamous cell carcinoma from the esophagus to the thyroid. We think that thyroid nodules in a patient with a history of malignancy should be considered to be secondary thyroid cancer.
Figure 1. 30 mm lesion in the subcarinal localization which deplased the esophagus to the right

Figure 2. Images of nodule with elastosonography and real time B mode ultrasonography
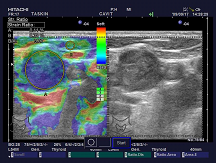
Figure 3. Squamous cell carcinoma diagnosed at proximal eusophagus (H&E, 100x), composed of neoplastic cells with pleomophism, hypechromasia, prominent nucleoli and increased mitotic figures (inlet, H&E 630x).
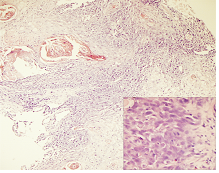
Figure 4. Discohesive areas with high mitotic activity (also inlet, 1000x). Note the presence of cytoplasmic vacuolization and tad pole figures (MGG, 400x). thyroid and LAP
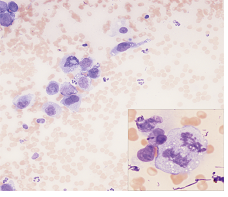
71 - Malignancy rate of thyroid nodules found to have hurtle cells in cytologic examination - 2010
Uluslararası Bildiriler 14th International Thyroid Congress, Paris, France, 11-16 September, Final Programme, www.itc2010.com, P-0144, 2010
ABSTRACT
INTRODUCTION: Oncocytic (presence of Hurthle Cell) changes in thyroid follicular epithelial cells might be seen both in benign and malign thyroid lesions. Our aim in this study is to investigate malignancy rate in nodules that are found to have Hurthle cell after fine needle aspiration biopsy (FNAB) and were operated for various reasons.
MATERIALS AND METHODS: Forty-four patients who has been evaluated in our thyroid diseases clinics between January 2009 and January 2010 and decided to undergo operation were assessed. These patients were asked to have operation for big nodule size, development in nodule sizes during follow up, compression symptoms or for permanent treatment of hyperthyroidism. Presence of Hurthle cell was demonstrated in cytological examination of all patients, preoperatively. Thyroid ultrasonography and ultrasound guided FNAB results were recorded. Patients reported to have these FNAB results were excluded. All patients undertake total thyroidectomy.
RESULTS: Thirty-eight of the patients were female and 6 were male. Mean age was 48±12 (19-70) years. Of the patients; 33 had euthyroid multinodulary goiter, 6 had euthyroid nodulary goiter, 1 had toxic diffuse multinodulary goiter, 1 had toxic diffuse nodulary goiter and 3 had toxic multinodulary goiter. Thyroid malignancy was detected in 6 (18.2%) patients, postoperatively. Of these, papillary microcarcinoma was determined in 4 and follicular carcinoma in 2. At least one of the thyroid antibodies was positive in 38% of cases who were found to have benign histopathology and 87.5% of malign cases (p=0.019). Both in malign and benign group, 25% cases were found to have lymphocytic thyroiditis in histopathological examination.
Table 1. Demographic characteristics of the patients | |
F/M | 38 / 6 |
Mean Age (year) | 48 ± 12 |
Soliter Nodul/ Multiple Nodul | 7 / 37 |
Euthyroid/ Hyperthyroid | 39 / 5 |
Benign/ Malign (B / M) | 38 / 6 (18.2%) |
Positive Thyroid antibodies % (B / M) | 38.0 / 87.5 (p=0.019) |
Figure 1.Hurtle cells in papillary carcinoma
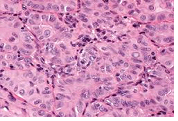
CONCLUSION: Hurthle cell changes which can both be seen in benign and malign thyroid diseases might cause some difficulties during histopathological examination. While Hashimato thyroiditis stands at one side of this spectrum; Hurthle cell adenoma, Hurthle cell carcinoma, oncocytic variant of papillary carcinoma and medullar carcinoma stands at the other side. Therefore, we believe that in case of presence of hurthle cell; possibility of malignancy should be kept in mind even if thyroid antibodies are positive.
70 - The advantage of total thyroidectomy for incidentally found thyroid cancer in an endemic region - 2010
Uluslararası Bildiriler 14th International Thyroid Congress, Paris, France, 11-16 September, Final Programme, www.itc2010.com, P-0143, 2010
ABSTRACT
INTRODUCTION: Total thyroidectomy is the procedure of choice in patients with thyroid cancer, toxic diffuse goiter, and toxic multinodular goiter. In recent years, total thyroidectomy has emerged as a surgical option to treat patients with multinodular goitre, especially in endemic iodine-deficient regions. The aim of this study was to investigate the impact of total thyroidectomy for incidental thyroid cancers in thyroid diseases that are preoperatively accepted as benign in an endemic iodine-deficiency region.
MATERIALS AND METHODS: 580patients who had consulted in our thyroid diseases policlinics between January 2006 and December 2009 were evaluated retrospectively. All the patients who were asked to undertake surgery for permanent treatment of hyperthyroidism, had euthyroid nodulary and multinodulary goiter been included in this study. Bigger nodule size, development in nodule size during follow up, or compression symptoms were the operation indications for patients with nodulary and multinodulary goitre. The results of thyroid ultrasonography (USG) and ultrasound guided fine needle biopsies (FNAB) were recorded. The patients with these FNAB results were excluded: malignancy, suspicion of malignancy, follicular adenoma, follicular lesion, hurtle cell adenoma, hurtle cell lesion and non-diagnostic cytology. All patients undertake total thyroidectomy.
RESULTS: Of the patients, 423 were female and 157 were male. Mean age was 44 ±13 (17-79) years.
429 patients undertake thyroidectomy forthe permanent treatment of hyperthyroidism and 151patient undertake it for euthyroid nodulary or multinodulary goitre. After the evaluation of all these patient groups; malignancy was detected in 64 (11%) patient, postoperatively. There was micropapillary ca(MPTC)in 21 patients, papillary ca(PTC)in 7patients, follicular variant of papillary ca(PCFV)in 6 patients and follicular ca(FTC)in 4 patients. Tumor was determined at a single focus among all patients(Table 2).
Table 1. Reasons of thyroidectomy and final pathology
Reason of thyroidectomy | Benign | Malign | Total |
Progression of nodulesize or big nodule | 6 | 2 | 8 |
Compressionsymptoms | 122 | 21 | 143 |
Hyperthyroidism | 388 | 41 | 429 |
Total | 516 | 64 | 580 |
Table 2. Number of cases of thyroid cancer types
Reason of thyroidectomy | MPTC | PTC | PCFV | FTC | Total |
Progression of nodule size or big nodule size | 1 | - | - | 1 | 2 |
Compressionsymptoms | 7 | 7 | 6 | 1 | 21 |
Hyperthyroidism | 13 | 26 | - | 2 | 41 |
Total | 21 | 33 | 6 | 4 | 64 |
CONCLUSION: In the present study, the incidence of incidental thyroid cancer was found to be 11% in patients undergoing operation for hyperthyroidism or nodular- multinodulary euthyroid goiter without any preoperative or perioperative suspicion of malignancy. We recommend that performance of total or near-total thyroidectomy as the primary procedure significantly reduced the rate of completion thyroidectomy for incidentally found thyroid cancer.
69 - Thyroid disorders in patients with celiac disease - 2010
Uluslararası Bildiriler 14th International Thyroid Congress, Paris, France, 11-16 September, Final Programme, www.itc2010.com, P-0014, 2010
ABSTRACT
INTRODUCTION: Celiac disease (CD) is an immune-mediated disease characterized by chronic inflammation and destruction of the villous structure of the small intestine. CD has increasingly become considered as a multi-organ disorder and has been linked to a number of diseases including autoimmune disorders. Different forms of thyroiditis are often referred to as autoimmune thyroid disease and have previously been suggested to be associated with celiac disease. In this study, we aim to characterize thyroid disorders in patients with CD.
MATERIALS AND METHODS: Twenty-tree patients with the newly diagnosis of CD (19 female, 4 male) based on clinical, laboratory, endoscopic and histopathologic findings were included. Mean age and mean body mass index were 35±11 (20-61) years and 23±4 (18-35) kg/m2, respectively. Thyroid function tests (fT3, fT4, TSH, AntiTPO, AntiTg) and thyroid ultrasonography (US) was carried out for all patients. Thyroid parenchyma was evaluated as homogenious or heterogenious with various degrees (mild, moderate, and severe). The number and size of nodules detected with US were recorded. US guided fine needle biopsy (FNAB) was performed on nodules, if necessary. Clinical diagnoses were made in the light of data obtained from thyroid function tests and ultrasonography.
RESULTS: Chronic autoimmune thyroiditis was detected in 6 (26.1%), multinodulary goitre in 2 (8.7%), solitary nodule in 2 CD patients. Cytological examination of FNAB results of patients with multinodulary goitre were reported as benign. It was reported as benign in one of two patients with solitary nodule, and cellular follicular lesion for the other one. Mean TSH value was found to be 2,47±1,8 (0,58-6,24) in patients with CD. There was a subclinical hypothyroidism in 6 patients who were determined to have chronic autoimmune thyroiditis; and mean TSH value was 5.32±0.59.Primarily, gluten free diet was given to these patients for CD.
Table 1 . Demographic characteristics of the patients
Patients with CD | |
N | 23 |
Female / Male | 19 / 4 |
Mean Age (year) | 35 ± 11 |
BMI (kg/m2) | 23 ± 4 |
Mean TSH ( uIU/mL) | 2.47 ± 1.8 |
Thyroid diseases (N / %) | |
Autoimmune Thyroiditis | 6 (26.1) |
Multinodulary Goitre | 2 (8.7) |
Soliter Nodule | 2 (8.7) |
CONCLUSION: Despite our patient group was small, we determined the incidence of chronic thyroiditis as 26.1%. We detected multinodulary goiter in 8.7% and solitary nodule in 8.7% of the patients. We suggest that CD patients should be evaluated with thyroid function tests, thyroid autoantibodies and thyroid US, when diagnosed.
68 - The predictive value of ultrasonography in detection of autoimmune thyroiditis - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 844, Endocrine Absracts, Volum 22, 2010
ABSTRACT
INTRODUCTION: Diagnosis of autoimmune thyroiditis is made by determination of elevated antibodies against thyroid peroxidase and thyroglobulin, and a hypoechoic pattern in ultrasound. In the present study we have performed a grey-scale quantitative analysis of thyroid echogenicity in the patients affected by autoimmune thyroiditis, obtaining the degree of hypoechogenicity associated with the appearance of thyroid dysfunction.
MATERIAL and METHODS: 632 patients who had autoimmune thyroiditis proven clinically, by laboratory and ultrasonographically were included in our study. Serum thyrotropin (TSH), thyroid hormones (fT3, fT4) and thyroid autoantibodies (Anti TPO Ab, Anti Tg Ab) were evaluated. Thyroid ultrasonography was performed in all subjects. An experienced endocrinologist who was uninformed about the laboratory results performed thyroid ultrasonography.
RESULTS: 551 (%87.2) of 632 patients were female and 81 (%12.8) were male. Mean age of the female and male patients were 46.2 ± 0.5 and 48.6 ± 1.71 years respectively. The thyroid parenchyma was classified as minimal heterogeneous, heterogeneous, and severe heterogeneous. TSH, Anti TPO Ab, and Anti Tg Ab levels were compared between these groups. TSH levels in the minimal heterogeneous and heterogeneous groups were significantly lower than the severe heterogeneous group (p<0.01 and p<0.001 respectively). When Anti TPO levels were compared significant difference was detected between groups (p<0.001). Anti TPO levels were lowest in the minimal heterogeneous, and highest in the severe heterogeneous group. In addition, Anti Tg levels were lower in the minimal heterogeneous and heterogeneous groups when compared with the severe heterogeneous group (p<0.001 and p<0.001 respectively). As with Anti TPO, Anti Tg levels were lowest in the minimal heterogeneous, and highest in the severe heterogeneous group.
CONCLUSION: Our study has shown that the paranchymal destruction has strongly associated with thyroid antibodies and TSH levels when it is classified by grey-scale ultrasonography.
67 - Thyrotoxic normokalemic periodic paralysis: a case report - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 776, Endocrine Absracts, Volum 22, 2010
ABSTRACT
INTRODUCTION: Hypokalemic periodic paralysis associated with hyperthyroidism is a well-known acute electrolyte and acute muscle disorder. Lesser known is normokalemic periodic paralysis associated with hyperthyroidism (TNPP). Because plasma potassium is normal, and it can be misdiagnosed as some other disorder if thyroid function is not evaluated. We report a case of TNPP due to non-autoimmune thyroiditis.
CASE REPORT: A 23-year-old woman was admitted to emergency department with muscular weakness of the lower extremities. She also presented to weight loss, increased appetite, and heat intolerance for the last two months. She denied any previous disease history or medication. In physical examination, her thyroid gland was minimal enlarged diffusely and non tender. In neurologic examination, there was symmetric flaccid paralysis with areflexia and impaired sensation in the lower extremities. Fasciculations, myoclonus and muscular atrophy were not observed. Cranial nerves were intact. ENMG and cranial MR were normal. Lumbar puncture was applied. Cerebrospinal fluids pressure and other related studies were normal. Laboratory studies revealed normal renal and hepatic function. Serum potassium 4,6 mmol/L (3,6-5 mmol/L) was. The thyroid function tests revealed a decreased level of TSH, an elevated level of fT4, and fT3. The thyroglobuline antibody and microsomal antibody test were negative. Thyroid ultrasonography revealed chronic thyroiditis. I-131 uptake was 2% in 4 hours (Normal: 15-25%), and 1% in 24 hours (Normal: 25-35%). The diagnosis was non-autoimmune thyroiditis accompanied by TNPP. Propranolol at a dose 20 mg four times per day was given to control of symptoms of hyperthyroidism. The paralysis completely improved without potassium supplementation.
CONCLUSION: Periodic paralysis can present with initial symptoms of thyrotoxicosis associated withnormokalemia. Thyroid function should be evaluated in patients presenting with muscle weakness, normal potassium concentrations and thyrotoxic symptoms to avoid inappropriate management and missing a curable form of paralysis.
66 - The relationship between aortic stiffness and left ventricular function in patients with Cushing’s Disease - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 731, Endocrine Absracts, Volum 22, 2010
ABSTRACT
INTRODUCTION: Aortic elastic properties and aortic stiffness are important determinants of increased cardiovascular morbidity and mortality in different diseases. We aimed to investigate the aortic function and to evaluate the relationship between aortic stiffness and systolic and diastolic functions of the left ventricle in patients with Cushing’s disease (CD).
MATERIAL and METHOD: Fourteen women and one man with newly diagnosed CD, and 17 control cases were enrolled in this study. All subjects underwent echocardiography and systolic and diastolic aortic measurements were noted from M-mode aortic root. Aortic elastic parameters, aortic strain, and distensibility were calculated. Left ventricle functions were measured using echocardiography including, two dimensional, M-mode, conventional Doppler, and tissue Doppler imaging.
RESULTS: Aortic strain (7.4±1.9% vs 12.3±2.4%; p<0.001), and aortic distensibility (3.2±1.1 10-6cm2dyn-1 vs 5.6±1.4 10-6cm2dyn-1; p<0.001) were significantly decreased in patient group compared with control group. Mitral E velocity and the ratio of E/A were significantly lower and deceleration time of E was significantly prolonged in patients with CD. We also observed that patients with CD had markedly lower early diastolic myocardial peak velocity (Em) and Em/Am ratio and higher Tei index than in control group. Aortic elastic parameters are deranged in patients with CD and there is a significant correlation between left ventricular parameters determined by tissue Doppler echocarciography and aortic elastic parameters in these patients.
CONCLUSION: Patients with CD should be screened with routine physical examination (including anthropometric measures and blood pressure measurement) and laboratory tests (including blood chemistry and electrocardiogram) as well as oral glucose tolerance test, 24 hour ambulatory blood pressure monitoring, echocardiography and carotid artery ultrasonography. In addition to these investigations, we suggest evaluation of aortic stiffness which is an early marker for atherosclerosis in patients with CS.
65 - Complementary and alternative treatment approaches in obese patients: a cross-sectional study - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 678, Endocrine Absracts, Volum 22, 2010
ABSTRACT
INTRODUCTION: Effective conventional medical treatments for obesity are limited and patients with obesity seeking alternative forms of health care for weight loss. While several previous studies have examined patterns of complementary and alternative treatment (CAT) use in different populations, limited data are available on the relationship between obesity and use of CAT. In this cross-sectional study, we aimed to overview the alternative therapy methods in obese patients.
MATERIAL and METHODS: Total 105, 22(21%) male and 83(79%) female patients were included this study. The body mass index (BMI) of female patients was 37.4±7.0 kg/m2 and BMI of male patient’s 35.5±3.8 kg/m2 were. Sixty-six (%62.9) of the patients used or still using alternative therapy methods. While evaluating the study group there were no significant difference found according to their economic status, sex and educational level (p>0.05). The BMI of the patients who use alternative therapy methods were 38.02±7.2 kg/m2, and BMI of the patients who does not lean to those alternative supplements is 35.4±4.5 kg/m2 (p=0.02). Comparing the duration of illness, it is most likely to use complimentary and alternative therapy methods who suffer from obesity for over 15 years (p=0.03). Most frequently used products were natural herbs (83.4%). Following this comes; acupuncture and massage. 30.1% of the cases claims that they temporary benefited from these products and methods, 30.5% said that they didn’t benefit and 39.4% don’t have a clear idea about whether they have benefited or not.
CONCLUSION: It is known that not only in our country but also allover the world the alternative therapy methods are widely used. We think that in our country, because of lacking education for obesity, patients are most likely to search alternative therapy methods.
64 - An association between autoimmune thyroiditis and premature ovarian failure: a cross-sectional study - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 477, Endocrine Absracts, Volum 22, 2010
ABSTRACT
INTRODUCTION: Premature ovarian failure is cessation of ovarian function before the expected age, which is usually accepted to be 40. Autoimmune diseases are a frequently seen group of disorders causing premature ovarian failure. In this study, we aimed to evaluate the frequency of autoimmune thyroiditis in patients with premature ovarian failure.
MATERIAL AND METHOD: Patients who admitted to our thyroid out patient clinic were included to our study. The patients were divided in to two groups according to their menopause age. Group 1 were patients whose menopause age was before 40, and group 2 were patients whose menapause age was after 40. The patients were evaluated according to their thyroid function tests (fT3, fT4, TSH), thyroid autoantibodies (AntiTPO Ab, AntiTg Ab) and thyroid ultrasonography. The patients were diagnosed as autoimmune thyroiditis when thyroid markers supported chronic thyroiditis on ultrasonography.
RESULTS: Forty-six of 80 patients were included in to Group 1, and 34 were included into Group 2. In Group 1 mean age was 42.4±7.6 years, mean menopause age was 34.5±5.1 years. In Group 2 mean age was 48.5±5.4 years, mean menopause age was 46.3±5.5 years. There was a statistically significant difference in age and menopause age between two groups (p<0.001). %72.7 of the patients in Group 1 and %35.3 of the patients in Group 2 had autoimmune thyroiditis. Our study has shown that autoimmune thyroiditis is statistically more common in patients who enter menopause before the age of 40 then patients who enter menopause after the age of 40 (p=0.002). The limitation of our study is that the patients were selected from our thyroid out patient clinic.
CONCLUSION: Autoimmunity is one of the most common causes of premature ovarian failure. We suggest that patients who enter menopause before the age of 40 should be investigated for autoimmune thyroiditis.
63 - Glycemic control and treatments in adults with type 1 diabetes mellitus - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 362, Endocrine Absracts, Volum 22, 2010
ABSTRACT
INTRODUCTION: Survival is increased in childhood- onset type 1 diabetes mellitus (DM) and approximately half of patients are diagnosed after the age of 15. Thus, a considerable number of patients with type 1 DM are adults. In this study, we aimed to investigate glycemic control and modalities of treatments in adult type 1 DM patients.
MATERIAL and METHODS: Data of type 1 DM patients hospitalized between January 2004 and December 2009 were evaluated retrospectively. Age at diagnosis, duration of diabetes, HbA1c levels and type of insulin treatment were recorded. Data at the time of initial hospitalization were analyzed in patients with multiple hospitalizations.
RESULTS: Two hundred and fifty patients were included in the study. There were 123 (49.2%) female and 127 (50.8%) male patients. The mean age of patients at the time of hospitalization was 31.9±9.7, mean age at diagnosis was 24.7±10.1, and duration of diabetes was 7.2±8.4 years. Type 1 DM was diagnosed at the age of 0-14 in 15.2%, 15-30 in 54.8% and >30 in 30% of patients. HbA1c was >9.5% in 49.6%, 7.5-9.5% in 27.6% and <7.5% in 22.8% of patients. 60% of patients was using four daily injections of insulin treatment and 27% was using one, two or three daily injections. 13% of patients was on insulin pump therapy. When we compared HbA1c in patients using different insulin regimens, we found that patients using insulin pump had significantly lower HbA1c levels (p<0.01).
CONCLUSION: In the adult population, type 1 DM is diagnosed with increasing frequency. In adult type 1 DM patient’s metabolic control is not well and the goal of near normoglycemia is achieved in few patients. Additionally, patients on insulin pump therapy have the best glycemic control.
62 - Thyroid disease in patients with type 1 diabetes mellitus - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 317, Endocrine Absracts, Volum 22, 2010
ABSTRACT
INTRODUCTION: Coexistence of Type 1 diabetes mellitus (DM) and autoimmune thyroid diseases was shown in previous studies. Thyroid dysfunctions and thyroid autoantibody positiveness were reported in 23-25% and 27-44% of patients with Type 1 DM, respectively. In recent years, thyroid ultrasonography (US) is widely used to diagnose autoimmune thyroid diseases with regard to its ability to define thyroid morphology and echogenity. In this study, we aimed to evaluate thyroid functions, autoantibodies and US features in Type 1 DM patients.
MATERIAL and METHOD: We retrospectively analysed 104 Type 1 DM patients (53 female, 51 male) followed in our clinic. Patients were matched with 58 healthy controls (27 female, 31 male) according to age and sex. Serum thyrotropin (TSH), thyroid hormones and thyroid autoantibodies were evaluated. Thyroid US was performed in all subjects.
RESULTS: Mean ages of Type 1 DM patients and control group were 31.08±9.38 and 27.59±7.17, respectively. Median TSH and fT3 were similar in Type 1 DM patients and control subjects, however median fT4 was significantly higher in patient group (p=<0.001). 26.3% of diabetic patients and 3.7% of control subjects had at least one of the thyroid autoantibodies (p=<0.001.). Prevalence of thyroid dysfunctions was significantly higher in Type 1 DM patients compared to control subjects (28.8% vs 3.4%, p=<0.001). In thyroid US, thyroid parenchyma was homogenous in 22.1% and heterogenous in 78.9% of patients, while it was homogenous in 91.4% of healthy controls. Similar rates of thyroid nodules was observed in the two groups.
CONCLUSION: Patients with Type 1 DM have higher rates of thyroid dysfunctions, autoantibody positivity and ultrasonographical abnormalities. Morphological abnormalities of thyroid gland are closely associated with thyroid autoantibody positivity and thyroid dysfunctions in Type 1 DM patients indicating the need for close follow-up in patients with abnormal US features.
61 - Causes and patterns of death in an endocrinogy clinic: data of six years - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 239, Endocrine Absracts, Volum 22, 2010
ABSTRACT
INTRODUCTION: Periodic review of hospital deaths is important to know the changing pattern of mortality in our environment. Ankara Ataturk Education and Research Hospital is a tertiary center with 18 in-patient beds in Endocrinology and Metabolism Clinic. Critical patients with endocrine-related diseases are also followed in intensive care unit. In this study, we aimed to evaluate demographic characteristics, hospitalization indications and causes of death in patients who died since the foundation of our endocrine clinic 6 years ago.
PATIENTS and METHODS: Data of patients hospitalized and died between January 2004 and December 2009 in our in-patient clinic were analyzed retrospectively. Age, sex, hospitalization indications and durations and mortality causes were evaluated. Among 5664 patients hospitalized during this period, 34 patients (0.6%) died.
RESULTS: There were 20 female (58.8%) and 14 male (41.2%) patients with a mean age of 70±18.7 (18-96). Hospitalization indications were diabetes mellitus (DM) related hyperglycemic emergencies in 22 (64.6%), oral hypoglycemic or insulin related hypoglycemia in 4 (11.8%), metabolic disturbances secondary to nutritional problems in 3 (8.9%), diabetic foot infection in 1 (2.9%), leukocytoclastic vasculitis and renal failure secondary to insulin therapy in 1 (2.9%), acute adrenocortical failure in 1 (2.9%), pituitary macroadenoma in 1 (2.9%), and hypocalcemia due to hypoparathyroidism in 1 (2.9%) patient. 28 (82.4%) of patients had type 1 or type 2 DM. Duration of hospitalization until death was 6.2±6.6 days(1-25 days). Descriptive data showed that patients were generally in geriatric age group and had chronic diseases (hypertension, coronary heart disease, cerebrovascular disease, cancer) in addition to endocrine-related diseases.
CONCLUSION: At the present day, more than 80% of diseases and deaths are associated with chronic diseases diagnosed in middle and old ages. Diabetes mellitus and DM related emergent states, particularly in geriatric age group, are the leading causes of death in our endocrine clinic.
60 - A rare cause of elevated liver enzymes: Addison’s disease - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 196, Endocrine Absracts, Volum 22, 2010
ABSTRACT
Common reasons of chronically elevated liver enzymes are; fatty liver associated with alcohol abuse or obesity, chronic viral hepatitis, autoimmune hepatitis, chronic bilier disease and hereditary metabolic disorders. Adrenocortical insufficiency can also cause elevated liver enzymes. Until now, there are few cases in the literature with abnormal liver function associated with Addison’s disease. We reported this case to kept mind while investigating the hypertransaminasaemia.
CASE REPORT: A 49-years-old woman admitted to our hospital with a two months history of weakness, fatigue and increased skin pigmentation. Her laboratory tests raveled low serum cortisol (2.9 ug/dL), increased adrenocorticotrophing hormone (ACTH) (>1250 pg/mL), aspartate transaminase (AST) and alanine transaminase (ALT) levels (120 U/mL and 87 U/mL respectively). Nevertheless, hyponatremia and hyperkalemia were not noted. Increased skin pigmentation, low serum cortisol, and high ACTH levels suggested Addison’s disease. Diagnosis was confirmed by ACTH stimulation test. No cortisol response was taken. 21-hydoxylase antibody was found positive. She had also evaluated for hypertransaminasaemia. Liver and spleen were not palpable. No lymphadenopathy was found. Other liver function tests were all normal. All viral hepatitis markers and tests for autoimmune hepatitis (antibodies against smooth muscle, mitochondria and nuclei) were negative. Abdominal tomography showed no pathology for liver and adrenal glands. When the Addison’s disease was confirmed by ACTH stimulation test, glucocorticoid therapy was given. Nearly two weeks after replacement therapy aminotransferase activity returned in normal range.
For patients with constantly elevated liver enzymes extra-hepatic diseases have to be considered. Although rare, Addison’s disease should be kept in mind.
59 - Our clinical experience in percutenous ethanol injection into cystic tyroid nodules - 2010
Uluslararası Bildiriler P619, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
AIM: Percutenous ethanol injection (PEI) is a minimally invasive method which can be preferred in treatment of cystic thyroid nodules. We have presented our cases of PEI below.
MATERIAL AND METHOD: We have performed PEI to 8 patients in our clinic. We have made ultrasound guided fluid aspiration from the cysts which were confirmed to be benign. We have injected ethanol (98%) into the pouche of the cyst in an amount that is 20-40% of the cystic fluid volume with ultrasound guidance.
RESULTS: The mean volume of cystic nodules was 13.6 ml (3.8-36.7 mL) and mean ethanol volume injected was 6.5 ml (1.5-15 mL). After the first performance of PEI we have recorded 50% reduction in nodule sizes at the first control visit of 2 patients. We had to perform PEI for the second time because we couldn’t record any significant reduction in nodule size in 6 patients. During the second PEI performance, mean nodule volume was 10.7 ml(6.5-32.4 mL) where as mean ethanol volume used was 4.5 ml(3-15 mL). After the second PEI, we observed almost 50% reduction in thyroid nodule sizes of extra 4 patients. In two patients we could not record any effective size reduction even after the 2nd PEI. They were referred to a surgeon for thyroidectomy. At the control visit, made 6 months after PEI, in 4 of 6 patients the cystic component of the nodules completely disappeared. Mean nodule size of these 6 patients was calculated as 0.36 ml (0.25- 0.54 mL). One year after PEI, we made fine needle aspiration to the nodules previously received ethanol injection and the cytology results were all benign.
DISCUSSION:PEI may be an alternative to surgery in complex nodules which are dominantly cystic in nature after eliminating the malignancy probability with fine needle aspiration.
58 - Diagnostic value of elastosonographically determined strain indexes in differentiated thyroid carcinomas - 2010
Uluslararası Bildiriler P469, 13th European Congress of Endocrinology, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
ABSTRACT
AIM:We aimed to determine strain index (SI) values using Elastosonography (ES) in histopathologically confirmed differentiated thyroid carcinomas (DTC) and investigate the role of these values for the differential diagnosis of nodular thyroid diseases.
MATERIAL AND METHOD:ES in longitudinal axis (LA) was performed in 391 thyroid nodules of 292 patients. ES scores of thyroid nodules were determined and SI in LA for each nodule was calculated. The findings were compared with histopathological results.
RESULTS: Histopathologically, of 391 nodules, 125 (31.97%) were malignant and 266 (68.03%) were benign. Among 125 malignant nodules, 100 were papillary thyroid carcinoma (PTC) (70 classical, 24 follicular variant, 3 solid trabecular variant, 2 columnar variant, 1 oncocytic variant), 15 were follicular carcinoma, 9 were hurthle cell carcinoma and 1 was medullary carcinoma. When we compared SI of 100 nodules with PTC/PTC variants and 266 benign nodules, we found that SI cut-off value for 90% sensitivity (Sn) was 5.885 (AUC 77.6+-0.03%; p=0.014). In hypoechogenic nodules with ES score of 4-5, irregular margins and type 1 vascularization pattern, SI cut-off value for 90% Sn was 17.020 (Sp: 50%, AUC 72.4+-0.08%; p=0.011). Data of 70 nodules with classical PTC was compared with data of benign nodules and SI cut-off value for 90% Sn was calculated as 7.885 (AUC 79.2+-0.03%; p<0.001). The optimal SI cut-off value in 30 nodules with variant PTC was 14.785 (Sn:73.3%, sp:66.2%, PPV:19.6%, NPV:95.7%). In these nodules, SI cut-off value for 90% Sn in LA was 4.480 (Sp:35.7). Since sample sizes of follicular and hurthle cell carcinomas were small, we did not make any analysis for these nodules.
CONCLUSION: SImeasurement using ES may be a valuable method with high sensitivity in PTC and PTC variants, however further studies with larger sample sizes are required to conclude about follicular and hurthle cell carcinomas.
57 - A diagnostic value of elastosonographically determined strain index in the differential diagnosis of benign and malignant thyroid nodules - 2010
Uluslararası Bildiriler 13th European Congress of Endocrinology, P468, 30 April - 4 May 2011, Rotterdam, The Netherlands, Endocrine Abstracts April 2011 Volume 26, ISSN 1470-3947 (print) ISSN 1479-6848 (online)
56 - Role of elastosonography scoring in follicular cancers - 2010
Uluslararası Bildiriler 14th International Thyroid Congress, Paris, France, 11-16 September, Final Programme, www.itc2010.com, P-426, 2010
ABSTRACT
PURPOSE: Elastosonography (ES) procedure of thyroid nodules is a new technique in differentiated thyroid cancers with yet uncertain results. There is no data in the literature about the ES scores in different forms of thyroid carcinomas. We aimed in this study to evaluate ES scores of 13 nodules which were prospectively undergone ES procedure, and histopathologically diagnosed as follicular thyroid cancer.
MATERIALS AND METHODS: Two hundred forty two patients who applied to our thyroid outpatient clinic with final decision of thyroidectomy due to malignancy, suspectful malignancy, large nodule size, or compression findings were included in the study. Real time ES in both transverse and longitudinal axes was applied to 334 thyroid nodules in these patients by the same person (BC). According to ES scores, 1 and 2 were accepted as benign (group A), and scores 3, 4, and 5 were accepted as malignant (group B). Fine needle aspiration biopsy was performed to all nodules. Nodules were evaluated cytopathologically and histopathologically. Scores in transverse and longitudinal axes were compared with histopathologic findings.
RESULTS: Of the 334 nodules, 104 (31.14%) were shown to be malignant, and 230 (68.86%) to be benign by histopathology. 13 of the 104 malignant nodules were diagnosed as follicular cancer. According to transverse axis scores, 12 (92.31%) of 13 follicular cancers were in Group1, and 1 (7.69%) were in Group 2. According to longitudinal axis scores, 7 (53.85%) of the 13 nodules were in Group 1, and 6 (46.15%) were in Group 2. The difference between ES scores determined according to transverse and longitudinal axes was statistically significant (p<0.001).
CONCLUSION: ES procedure of follicular cancers yielded 92.31% false negative results in transverse axis, and 53.85% false negative results in longitudinal axis. These findings show that scoring according to ES procedure is not a suitable technique in diagnosis of follicular cancers.
55 - Which axis should be performed for elastosonography scoring in thyroid nodules? - 2010
Uluslararası Bildiriler 14th International Thyroid Congress, Paris, France, 11-16 September, Final Programme, www.itc2010.com, P-0327, 2010
ABSTRACT
INTRODUCTION: Elastosonography (ES) is a more recently developed dynamic technique that evaluates the tissue elasticity with the aid of ultrasonography by measuring the degree of morphological changes due to an external force. Up to the present, all the studies on thyroid are generally the ones which investigate the role of ES in estimating malignancy. There is no available data in literature regarding on which axis ES should be performed in thyroid nodules. In this study, we aimed to research whether the scoring differences between transverse and longitudinal axis on which ES is carried out is beneficial in differentiation of benign and malignant thyroid nodules.
MATERIALS AND METHODS: Two hundred and forty two patients who applied to our thyroid policlinics and have been decided to undergo thyroidectomy for bigger nodules, compression symptoms, malignancy or suspicion of malignancy were included in this study.By the same expert (BC), real-time ES was performed on 334 nodules of these patients both in transverse and longitudinal axis. Detected scores 1-2 were accepted as benign (Group 1) and score 3-4-5 as malignant (Group 2). Fine needle aspiration biopsy (FNAB) carried out on all nodules. They were also examined histopathologically and cytopathologically. Both transverse and longitudinal axis scores were compared with histopathologic findings.
RESULTS: Of these 242 patients, 198 were female (81.82%) and 44 were male (18.18%). The mean age was 46.66±12.12 years (19-77). As the mean age was 45.25±12.05 years for women and 47.65±12.48 years for men; the difference between groups in terms of gender was not significant (p=0.234). It was histopathologically demonstrated that 104 of 334 nodules, which were evaluated by ES preoperatively, were malignant (31.14%) and 230 were benign (68. 86%). On transverse axis, the number of histpathologically benign nodules was 140 (specificity: 60.87%) and the number of malignant nodules was 42 (false negativity: 40.78%) in Group 1; in Group 2, the number of benign nodules was 90 (false negativity: 39.13%) and the number of malignant nodules was 62(sensitivity: 59.62%). On longitudinal axis, the number of benign nodules was 86 (specificity: 37.39%) and the number of malignant nodules was 27 (false negativity: 25.96%) in Group 1; in Group 2, the number of benign nodules was 144(false negativity: 62.61%) and the number of malignant nodules was 77 (sensitivity: 74.04%).
Figure1. Nodule image on ES in longitudinal axis
.png)
Figure2.Nodule image on ES in transverse axis
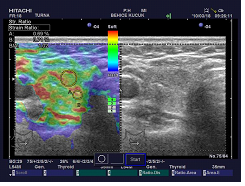
Table1.ES scores and histopathologic findings in transverse axis
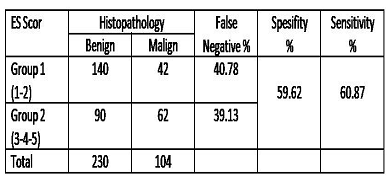
Table2. ES scores and histopathologic findings in longitudinalaxis
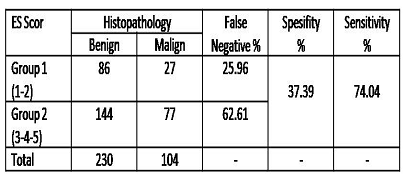
CONCLUSION: In terms of sensitivity, the difference between longitudinal and transvers axis was statistically significant (p=0.036). Longitudinal axis is sensitive for determination of malignant nodules. In terms of specificity, the difference between transverse and longitudinal axis was statistically significant (p=0.002). Transverse axis is specific for determination of benign nodules.
54 - Importance of nodule localisation in elastosonographic evaluation of thyroid nodules - 2010
Uluslararası Bildiriler 14th International Thyroid Congress, Paris, France, 11-16 September, Final Programme, www.itc2010.com, P-0326, 2010
ABSTRACT
PURPOSE: The aim of this study is to investigate whether localization of nodules alters ES scores, and to determine role of nodule localization in predicting malignancy.
MATERIALS AND METHODS: 242 patients with final decision of thyroidectomy due to malignancy, suspicious for malignancy, large nodule size, or compression findings were included in the study. ES was applied to 334 thyroid nodules by the same person (BC). Nodule localizations were defined as right lobe, left lobe, isthmus, inferior, medial, superior, anterior, posterior, and combinations of these regions in grey scale. According to ES scores, 1 and 2 were accepted as benign (Group 1), and scores 3, 4, and 5 were accepted as malignant (Group 2). Nodules were evaluated cyto-histopathologically. ES scores according to transverse (T) and longitudinal (L) axes were compared with nodule localizations.
RESULTS: Of the 334 nodules, 104(31.1%) were shown to be malignant, and 230(68.8%) to be benign by histopathology. According to T axis in Group 1, number of histopathologically benign nodules were 140(specificity: 60.8%), malignant nodules were 42(false negative:40.7%). 10(23.8%) of these nodules were completely filling the lobe. 4(9.5%) of them were superior anterior, and 4(9.5%) had invaded inferior. 24(57.1%) of the nodules were in right lobe, 15(35.7%) were in left lobe, and 3(7.1%) were at the isthmus. 25 of the nodules(64.1%) with false negative results in this axis were at the inferior region. In T axis in Group 2, number of benign nodules was 90(false positive: 39.1%). 15(17.0%) of these nodules were localized at inferior anterior, 14(15.9%) at inferior posterior, 9(10.2%) invading inferior, and 8(9.0%) were at middle posterior. 44.7% of the nodules were in right lobe, 50% were in left lobe, and 2(2.2%) were at the isthmus. 58(65.9%)of total 90 nodules were localized at the inferior region. Number of malignant nodules in transverse axis was 61(sensitivity: 59.6%).In L axis, number of benign nodules was 86(specificity: 37.3%), malignant nodules was 27(false negative: 25.9%) in Group 1. 6(23.0%) of the nodules were invading the whole lobe. 5(19.2%) nodules were at inferior anterior. 19(70.3%) of nodules were in right lobe, 7(25.9%) were in left lobe, and 1(3.7%) was at the isthmus. 20(76.9%) of the false negative nodules in longitudinal axis were at inferior region. Of the 144 nodules which caused false positive results in the L axis, 24(17.0%) were at inferior posterior, 23(16.3%) were at inferior anterior, 17(12.0%) were invading inferior, and 14(9.9%) were at middle posterior localization. 71(49.3%) of the nodules were in right lobe, 70(48.6%) were in left lobe, and 3(2.0%) were at the isthmus.
Figure 1.A score 5 nodule at right lobe - superior anterior
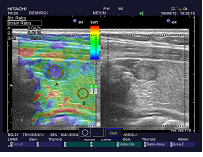
Figure 2. A score 4 nodule at left lobe - inferior anterior
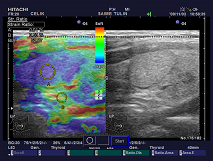
Figure 3. A score 5 nodule at right lobe - medial
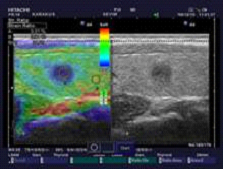
CONCLUSION: 20(76.93%) of the false negative nodules in L axis, and 58(65.92%) of the false negative nodules in T axis were localized at the inferior region. It is remarkable that most of the false positive nodules according to ES scoring in L axis were localized at the inferior region.
53 - Dıagnostic value of elastosonography in evaluation of cellular adenomatous nodules - 2010
Uluslararası Bildiriler 14th International Thyroid Congress, Paris, France, 11-16 September, Final Programme, www.itc2010.com, P-0325, 2010
ABSTRACT
INTRODUCTION: Cellular adenomatous nodules(CAN)are in benign group according to Bethesda classification. Nevertheless, there is no consensus among thyroidologists on the approach to these nodules. We aimed to determine the diagnostic value of elastosonography (ES) in cases which were cytopathologically diagnosed as CAN.
MATERIALS AND METHODS: Two hundred forty two patients who applied to our thyroid out-patient clinic with final decision of thyroidectomy due to malignancy, suspicious for malignancy, large nodule size, or compression findings were included in the study. Real- time ES in both transverse and longitudinal axes was applied to 334 thyroid nodules in these patients by the same person (BC). Nodules were scored between 1 and 5 according to ES. Fine needle aspiration biopsy was performed to all nodules. Nodules were evaluated cytopathologically and histopathologically. Scores in transverse and longitudinal axes of the nodules which were cytopathologically diagnosed as CAN were compared with histopathological findings.
RESULTS: Cytopathological diagnosis of CAN was present in 51 of 334 nodules from a total 242 patients. Final pathological reports of these nodules were benign in 38 (74.54%), and malignant in 13 (25.46%) nodules. Pathological examination of malignant nodules showed that 3 were papillary carcinoma, 4 were follicular carcinoma, 5 were variant of papillary carcinoma, and 1 was hurtle cell carcinoma. From 51 patients with the diagnosis of CAN, ES scores in transverse axis were 1 in 8 (15.69%), score 2 in 28 (54.90%), score 3 in 12 (23.53%), score 4 in 2 (3.92%), and score 5 in 1(1.96%). ES scores in longitudinal axis were 1 in 4 (%7.84), score 2 in 22 (%43.14), score 3 in 13(%25.49), score 4 in 10 (19.61%), and score 5 in 2 (3.92%). There was no meaningful correlation between ES scores and histopathology results. According to transverse scoring, 75% of score 1 nodules, 64% of score 2 nodules, 100% of score 3 nodules, 100% of score 4 nodules, and 50% of score 5 nodules were benign. According to longitudinal scoring, 75% of score 1 nodules, 72% of score 2 nodules, 69% of score 3 nodules, 90% of score 4 nodules, and 50% of score 5 nodules were benign.
Figure1. A cellular adenomatous nodule image on ES in longitudinal axis (Score 2)
.png)
Table1.Demographic datasof the patients
All patients | Patients with CAN (+) | |
N | 242 | 39 |
Mean Age | 46.66±12.12 | 44.93±13.17 |
F / M | 198 / 44 | 31 / 8 |
Nodule (N) | 334 | 51 |
Benign / Malign | 230 / 104 | 38 / 13 |
Table2. ES scores and distribution of patients in each axis
ES Score | 1 | 2 | 3 | 4 | 5 |
Transvers Axis (N) % | 8 15.69 | 28 54.90 | 12 23.53 | 2 3.92 | 1 1.96 |
Longitudinale Axis (N) % | 4 7.84 | 22 43.14 | 13 25.49 | 10 19.61 | 2 3.92 |
CONCLUSION: Nodules with scores 3, 4, and 5 according to ES scoring system were expected to be malignant. High rate of benign pathology results within these groups arouses serious question marks about diagnostic values of ES scoring system.
52 - Is nodule size important in elastosonography scoring of thyroid nodules? - 2010
Uluslararası Bildiriler 14th International Thyroid Congress, Paris, France, 11-16 September, Final Programme, www.itc2010.com, P-0324, 2010
ABSTRACT
INTRODUCTION: Elastosonography (ES) is a technique gaining acceptance in differential diagnosis of benign and malignant thyroid nodules. However, there is no data in the literature about the effect of nodule size on ES scores. Purpose of this study is to categorize evaluated nodules according to the longest axis by ES, and investigate whether it is useful in differentiating benign and malignant nodules.
MATERIALS AND METHODS: Two hundred and forty two patients who applied to our thyroid outpatient clinic with final decision of thyroidectomy due to malignancy, suspicious malignancy, large nodule size, or compression findings were included in the study. Real- time ES was applied to 334 thyroid nodules in these patients by the same person(BC). According to ES scores, 1 and 2 were accepted as benign(Group A), and scores 3, 4, 5 were accepted as malignant(Group B). 4 groups were composed according to longest axis of evaluated nodules. Group 1: <5 mm, Group 2: 5-10 mm, Group 3: 11-40 mm and Group 4: >40 mm. Fine needle aspiration biopsy(FNAB) was performed to all nodules. Nodules were evaluated cytopathologically and histopathologically. Relationship between score, histopathology, and nodule size in transverse and longitudinal axis was examined.
RESULTS: Of the 242 patients, 198 were female(81.82%), 44 were male(18.18%). Mean age was 46.66±12.12 years (19-77). Of the 334 nodules, 104 (31.14%) were shown to be malignant by histopathology, and 230 (68.86%) to be benign. 8 of the nodules (2.40%) were in Group 1; 84 (25.15%) were in Group 2; 216 (64.67%) were in Group 3; and 26 (7.78%) were in Group 4. In T axis of Group 1: 5 nodules (2.75%) were Group A, and 3 nodules (1.97%) were Group B. In L axis of Group1: 5 nodules (4.42%) were group A, and 3 nodules (4.42%) were Group B. In Group 2 T axis, there were 41 nodules (22.53%) in Group A, and 43 nodules (28.29%) in Group B. In Group 2 L axis: 24 nodules (21.24%) were in Group A, and 60 nodules (27.15%) were in Group B. In Group 3 T axis: 112 nodules (61.54%) were in Group A, and 104 nodules (68.42%) were in Group B. In Group 3 L axis, 69 nodules (61.06%) were in Group A, and 147 nodules (66.52%) were in Group B. In Group 4 T axis, 24 nodules (13.19%) were in Group A, 2 nodules (%1.32) were in Group B. In Group 4 L axis, 15 nodules (13.27%) were in Group A, and 11 nodules (4.98%) were in Group B. In L axis, 4.42% of Group A nodules were in Group 1, whereas 13.27% were in Group 4. In L axis, 1.36% of Group B nodules were in Group 1, and 4.98% were in Group 4 (p=0.012). In T axis 2.75% of nodules in Group A were in Group 1, and 13.19% were in Group 4. In T axis, 1.97% of Group B nodules were in Group 1, and 1.32% were in Group 4 (p=0.001)
CONCLUSION: Histopathological distribution according to nodule size was not meaningful (p=0.236), whereas scoring according to nodule size was found to be meaningful (p<0.05).
Group 1: < 5mm Group 2: 5- 10mm Group 3: 11-40mm Group 4: > 40 mm




51 - A rare cutaneous manifestation in Cushing’s Syndrome: generalized pustular psoriasis - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 195, Endocrine Absracts, Volum 22, 2010
ABSTRACT
INTRODUCTION: Generalized pustular psoriasis is a rare and the most severe form of psoriasis. It is usually seen in adults. Generalized pustular psoriasis is characterized with sudden eruption of yellowish pustule groups on the shiny erythematous skin, measuring 2 to 3 millimeter, and cover the all body in a short time. In this report, we presented a patient with Cushing’s syndrome (CS) who had determined pustular psoriasis.
CASE REPORT: A 35 years old woman was admitted because of a widespread erythematous and millimetric brown maculopapular lesions and sterile pustular eruption associated with postinflammatory hyperpigmentation on the head, face, trunk, and extremities. In addition, in her physical examination, she had a facial plethora, hair loss, purple striaes, and hirsutismus. Her biochemical and hormonal tests indicated glucocorticoid excess. Cushing’s syndrome was confirmed by the dynamic tests. Magnetic resonance imaging (MRI) revealed a pituitary lesion of 3.2 millimeter in diameter. Inferior petrosal sinus sampling (IPSS) was performed. After the results of laboratory tests and imaging procedures, Cushing’s disease was determined. Biopsy from the skin lesions revealed early period of pustular psoriasis.
CONCLUSION: The classic cutaneous manifestations of CS are; facial plethora, acne, purpura, cutaneous atrophy, hirsutism, vellous hypertrichosis, and wide purplish striae over the abdomen, flanks and upper arms. Acanthosis nigricans can occur but it is usually mild. In the literature, in our knowledges, there is no case together with Cushing’s syndrome and pustular psoriasis. This case is reported since these two conditions are rarely seen together.
50 - Thyroid storm accompanied by H1N1 influenza infection - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 194, Endocrine Absracts, Volum 22, 2010
ABSTRACT
CASE REPORT: A 56-year-old woman admitted to emergency department with fever, dyspnea, productive cough, palpitations, diffuse myalgia, and malasia. Physical examination revealed an anxious-appearing woman with fine tremor in the hands. Her pulse was 140 beats/minute and irregular; blood pressure, 140/90 mmHg; temperature 38.6 ºC, respiratory rate 40 breaths per min, and oxygen saturation 91% without supplemental oxygen. In auscultation, bilaterally rales and bronchial breath sounds were heard. Chest radiography at admission showed bilaterally patchy pneumonia. The leukocyte count was 3.400 per μl with 45% polymorphonuclear cells, 50% lymphocytes and 5% monocytes. In physical examination, her thyroid gland was enlarged diffusely and non tender. Electrocardiogram showed atrial fibrillation with a rapid ventricular response. Because of her symptoms and the findings on the physical examination, laboratory tests for thyroid function were done. The test revealed a decreased level of thyroid- stimulating hormone, an elevated level of free thyroxine, and free triiodothyronine. The patient’s condition continued to worsen, and she was admitted to the intensive care unit for further evaluation and management. Propylthiouracil, propranolol, and supportive therapy were started. Nasopharyngeal- swab samples were taken for influenza H1N1 virus. On day 4 of admission, samples were positive for influenza H1N1 virus by PCR. No other organisms were detected from blood, urine or respiratory tract. A 5 day course of oseltamivir was added to the therapy. The diagnosis was thyroid storm accompanied by H1N1 influenza infection. After 12 days, patient’s levels of thyroid hormones had decreased, vital signs returned to completely normal.
CONCLUSION: Thyroid storm is a rare and life- threatening endocrinologic emergency that may be precipitated by trauma, surgery, systemic illness, particularly infection and sepsis. We think that, our patient highlights the potential impact of H1N1 influenza infection for thyrotoxic patients.
49 - Are the thyroid function associated with widespread of acute coronary syndromes? - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 133, Endocrine Absracts, Volum 22, 2010
ABSTRACT
INTRODUCTION: Serum thyroid hormone levels have been described in several systemic non-thyroideal illnesses, among them acute heart diseases. The aim of this study was to investigate the relationship between thyroid functions and widespread of ACS, and to evaluate the potential changes in thyroid hormone profile in acute coronary syndromes (ACS) at the time of diagnosis and compare them between two groups, based on therapeutic implications and distinct prognoses: unstable angina/ non-ST-segment elevation acute myocardial infarction (UA/NSTEMI) and ST-segment elevation acute myocardial infarction (STEMI).
MATERIAL and METHOD: 94 patients admitted to the coronary care unit of our center were evaluated. Patients were excluded if they were known to have thyroid function test abnormalities. Coronary artery angiogram was performed in all patients. Significant stenosis was defined as the internal diameter decreased by more than 50%. Groups were re-grouped according to the number of significantly stenotic vessels into normal, 1-vessel, 2-vessel, and 3-vessel diseased groups. Thyroid functions were evaluated in groups.
RESULTS: There were 67 patients with UA/NSTEMI (46 men, 21 women, and the mean age 60.3±11.3 years), and 27 patients with STEMI (13 men, 14 women, and the mean age 64.0±13.0 years) included. Thyroid hormone levels [thyroid-stimulating hormone (TSH), free triiodothyronine (fT3), free thyroxine (fT4)] were compared in UA/NSTEMI and STEMI groups on admission. There were no significant differences between two groups for fT3, fT4 and TSH levels (p>0.05). Also, thyroid functions were not associated with the widespread of coronary artery disease according to coronary angiography (p>0.05).
CONCLUSION: Thyroid function tests are altered in patients with ACS. The changes are characterized by euthyroid sick syndrome. However, our results show that the thyroid functions are not different between UA/NSTEMI and STEMI groups. Also thyroid functions in acute stage are not seems to be associated with the widespread of coronary artery disease.
48 - QTc and P wave dispersion in patients with Cushing’s Syndrome - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 59, Endocrine Absracts, Volum 22, 2010
ABSTRACT
INTRODUCTION: The clinical implications of QTc and P wave dispersion in patients with Cushing’s syndrome have not been studied previously. In this study, we aimed to compare QTc dispersion and P wave dispersion in patients with Cushing’s syndrome and healthy subjects.
MATERIAL and METHOD: Sixteen patients with Cushing’s syndrome diagnosed on clinical, laboratory and imaging findings and 16 age and sex matched control subjects were included. All subjects underwent a routine standart 12- lead suface electrocardiograpy recorded at a paper speed of 25 mm/s and gain of 100 mm/mV. Maximum, minimum and mean QT intervals were calculated. Measured maximum and minimum QT intervals were corrected by Bazett’s formula (QTc=QT/ÖRR), and were defined as corrected QT interval (QTc). The difference between the maximum and minimum QTc interval was defined as QTc dispersion and the difference between maximum P wave duration (Pmax) and minimum P wave duration (Pmin) was calculated as P-wave dispersion (PWD).
RESULTS: Maximum QTc interval (429.9 ±24.8 vs 408.4 ±24.7; p=0.02), QTc interval (389.0 ±22.0 vs 375.5 ±11.6; p=0.04) and QTc dispersion (84.9 ±17.6 vs 70.9 ±13.2; p=0.02) were significantly longer in patients with Cushing’s syndrome compared to healthy subjects. There was no significant difference in Pmax, Pmin and P-wave dispersion between groups (p>0.05).
CONCLUSION: We showed that QTc interval and QTc dispersion were increased in patients with Cushing’s syndrome compared to healthy subjects; however p-wave dispersion did not change. Accordingly, significant electrical heart function disturbances which might be life-threatening may occur in patients with Cushing’s syndrome indicating need for early monitorization by a cardiologist in these patients.
47 - Pheochromocytoma in an incidentally discovered cystic adrenal mass: a case report - 2010
Uluslararası Bildiriler 12th European Congress of Endocrinology, Praque, Czech Republic, 24-28 April, P 15, Endocrine Absracts, Volum 22, 2010
ABSTRACT
INTRODUCTION: Adrenal cysts are rare usually benign and asymptomatic. Histologically, they are classified as epithelial, endothelial, parasitic and pseudocysts. Although extremely rare and clinically more dramatic cystic adrenal carcinoma and cystic pheochromocytoma must be considered in the differential diagnosis of adrenal cysts. In this report, we presented a patient with a large cystic pheochromocytoma.
CASE REPORT: A 30-year-old female patient admitted our clinic with a left sided adrenal mass detected incidentally on a routine control. Her passed medical history was unremarkable. She had no episodic hypertensive attack, no complaint of sweating or headache. Vital signs were normal, with a heart rate of 72 beats/minute and a blood pressure of 110/70 mmHg. Physical examination was completely normal. Adrenal MRI revealed a 72x59x75 mm lesion at the left adrenal lodge with septations. The mass did not show any contrast enhancement and was reported as Type III hydatid cyst. In contrast, the hemmaglutination test was negative. The eosinophil count was normal. Serum potassium levels were normal. Urine normetanephrine and VMA were markedly increased. Left adrenalectomy was performed. The patient’s intra-operative and postoperative courses were uncomplicated. The surgical specimen revealed pure cystic pheochromocytoma. Postoperatively the urine normetanephrine and VMA levels returned in to the normal range.
CONCLUSION: Cystic pheochromocytomas may not present with the classic prodromal symptoms, which are commonly associated with solid pheochromocytomas. This case represents an unsuspected presentation of an extremely rare functional cystic neoplasm. Pheochromocytoma should be considered in patients presenting with an incidental cystic adrenal mass, even in the absence of hypertension.
46 - Ca 19-9 levels in type 2 diabetes mellitus patients4 - 2009
Uluslararası Bildiriler 11 th European Congress of Endocrinology, Istanbul, Turkey, 25-29 April 2009, P 380. Endocrine Absracts, Volum 20, 2009
ABSTRACT
BACKGROUND
Ca19-9 is a tumor -associated antigen. In this study, we aimed to compare Ca 19-9 levels in type 2 diabetes mellitus (DM) patients and healthy control group.
METHOD
215 type 2 DM patients (82 male and 133 female) and 209 healthy control group (79 male, 130 female) age, sex and body mass index (BMI) matched were included in the study. Duration of diabetes, HbA1c and presence of complications were analyzed. Cases with high serum levels of Ca 19-9(0-35 U/mL) were evaluated with abdominal MRI. A female patient with high serum Ca 19-9 was diagnosed as pancreas carcinoma and excluded from the study.
RESULTS
Median Ca 19-9 in DM patients was 13.8 (0-302.8) and 7.53 (0.4-46.97) in control group and difference was statistically significant (p<0.001). Number of cases with high serum Ca 19-9 levels in patients and control group were 45 and 2, respectively. The difference was again statistically significant (p<0.001). Considering all cases, Ca 19-9 levels were similar in both females and males (p=0.794). In DM patients, Ca 19-9 did not correlate with BMI, duration of diabetes or number of complications, however, it was found to be positively correlated with HbA1c levels (rho=0.17, p=0.015). Ca 19-9 did not change with presence of nephropathy, retinopathy, neuropathy and number of complications (p=0.778, p=0.258, p=0.241 and p=0.457, respectively).
CONCLUSIONS
Chronic pancreatitis is a risk factor for pancreatic cancer, and the same is also true for diabetes. Ca19-9 is used in the diagnosis of pancreatic cancer but also a marker of pancreatic tissue damage that might be caused by diabetes. Therefore it is necessary to define the normal range of Ca19-9 in type 2 diabetic patients in order to eliminate additional approaches. Therefore diabetic patients have to be followed up for pancreatic cancer.
45 - Case Report: papillary thyroid carcinoma in a patient with Penred syndrome - 2009
Uluslararası Bildiriler 11 th European Congress of Endocrinology, Istanbul, Turkey, 25-29 April 2009, P 312. Endocrine Absracts, Volum 20, 2009
ABSTRACT
OBJECTIVE
Pendred syndrome is an autosomal recessive disorder characterized by sensorineural hearing loss, goiter, and a partial defect in iodide organification. Pendred syndrome is caused by mutations in the SLC26A4 gene. Here, we report a patient with pendred syndrome and papillary thyroid carcinoma.
CASE REPORT
A 19-year-old man admitted to our clinic with swelling in his neck. Congenital hypothyroidism was diagnosed at the age of one. His twin brother and his sister had been diagnosed as congenital hypothyroidism when they were one year old. In physical examination, a visible goiter was present and the thyroid was enlarged with multiple palpable nodules. In laboratory examination serum TSH was 2.1 µIU/mL (0.4 to 4.0), free T4 was 0,87 ng/dl (0.85-1.78), free T3 was 4,21 pg/ml (1.57-4.71) and Thyroglobulin was >300 ng/ml(0-55). Ultrasonographically, there were multiple nodules in thyroid. Thyroid scintigraphy showed hypoactive nodular goitre. Perchlorate discharge test revealed increased uptake and washout. Increased discharge pointed to an organification defect as in Pendred syndrome. Fine needle aspiration biopsies were benign. Sensorineural hearing loss was not detected. Bilateral total thyroidectomy was performed because of cosmetic complaints and enlarged multinodular goitre. Postoperative histopatology was reported as papillary thyroid carcinoma of 13 milimeter. There was no capsular or vascular invasion. After surgery 100mCI radioactive iodine was given to the patient and also L-thyroxin was started.
CONCLUSION
Goiter is the most frequent symptom of Pendred syndrome and associated with an insufficient thyroid hormone synthesis caused by a defect in iodide organification. Pendrin expression has been studied in various human benign and malign thyroid neoplasms. Thyroid carcinoma can be seen in patients with Pendred syndrome. Recurrence of benign thyroid nodules after thyroidectomy in these patients is common. Therefore; if surgical management is considered for any reason in these patients, total/near total thyroidectomy should be preferred.
44 - Concurrent thyroid medullary, papillary carcinoma and Hashimoto thyroiditis: case report - 2009
Uluslararası Bildiriler 11 th European Congress of Endocrinology, Istanbul, Turkey, 25-29 April 2009, P 271. Endocrine Absracts, Volum 20, 2009
ABSTRACT
INTRODUCTION
The incidence, cell origin, histopathologic features and prognosis of papillary and medullary carcinoma are considered to be completely different. Simultaneous occurrence of medullary and papillary thyroid carcinoma in the same patient is rare. Here, we present a patient with synchronous medullary thyroid carcinoma and papillary microcarcinoma occurring in a thyroid with chronic lymphocytic thyroiditis.
CASE
A 47 years old woman with no history of chronic illness and no pathologic sign except palpable nodules in thyroid applied with swelling and intermittant pain in the neck. She was euthyroid both clinically and laboratuary. In thyroid ultrasonography, multiple hypoechoic nodules with microcalcifications in left lobe of thyroid were detected. Because, fine needle aspiration biopsy of the 13x10 mm nodule in superior posterior left lobe was reported as suspicious for medullary carcinoma, she underwent bilateral total thyroidectomy and left radical neck dissection. In pathologic examination, in superior part of left lobe a medullary thyroid carcinoma of 15 mm with thyroid capsule infiltration and lymphovascular invasion was found (figure 1). Tumor cells were strongly positive for calcitonin, chromogranin and carcinoembryonic antigen, immunohistochemically (figure 2). Additionaly, there was a papillary microcarcinoma foci of 1 mm in lateral part of the same lobe (figure 3). 3 lymph nodes were positive for medullary carcinoma metastases also, and chronic lymphocytic thyroiditis was detected in remaining thyroid tissue. MEN was excluded with laboratory and imaging studies. Postoperative serum calcitonin was <2 pg/ml. She was treated with radioactive iodine.
CONCLUSION
It is still not obvious whether coexistence of medullary carcinoma and papillary carcinoma in thyroid is just incidental or due to a common stem cell or genetic alteration. Also, role of lymphocytic infiltration in this coexistence remains unidentified. Further investigations and genetic analyses are needed to explain the pathogenesis of simultaneous lymphocytic thyroiditis and papillary and medullary carcinoma in the same thyroid.
Figure1. Medullary thyroid carcinoma
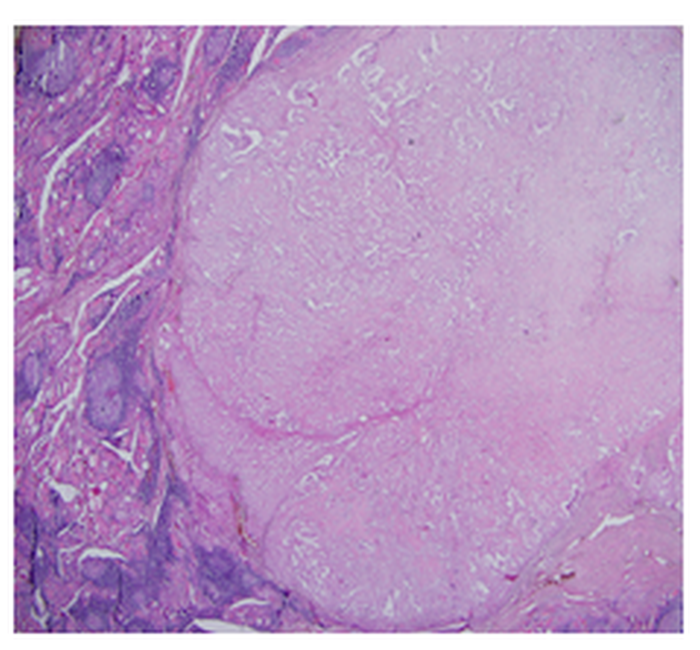
Figure 2: A,B,C:Tumor cells with vesicular chromatin, forming strings and grooves. (Hematoxylene-eosin, magnification, X200, X400, X600) D: Diffuse cytoplasmic chromagranin staining in tumor cells (Chromogranin, magnification X200)
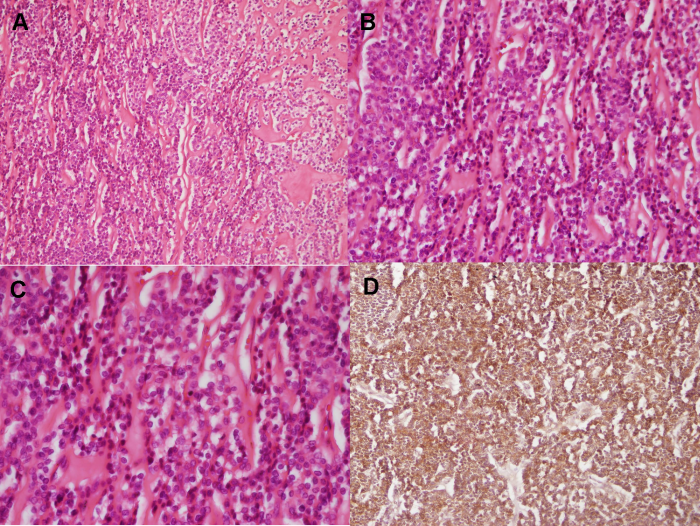
Figure3.Hashimoto thyroiditis and papillary carcinoma in a a small area

43 - Concurrency of primary hyperparathyroidism and thyroid disases - 2009
Uluslararası Bildiriler 11 th European Congress of Endocrinology, Istanbul, Turkey, 25-29 April 2009, P 147. Endocrine Absracts, Volum 20, 2009
ABSTRACT
OBJECTIVE
Thyroid diseases are reported to be in 22-70% of primary hyperparathyroidism (PHPT) patients in different studies. Thyroid pathology is detected during neck exploration in some of these patients. In this study we aimed to investigate thyroid pathology in patients operated for PHPT in our clinic.
METHOD
32 PHPT patients were included in the study. Patients were evaluated with thyroid function tests, antithyroglobulin antibody, antithyroid peroxidase antibody, TSH receptor antibody, thyroid Ultrasonography (US), and fine needle aspiration biopsy (FNAB). All patients were operated including neck exploration.
RESULTS
Thyroid US before operation yielded thyroid nodule in 21 patients. 17 patients were euthyroid before operation of which 12 had multinodular goiter (MNG), 3 had nodular goiter (NG) and 2 had postoperative recurrent MNG. One of two hyperthyroid patients had toxic MNG whereas the other had toxic diffuse goiter. Chronic thyroiditis and MNG with thyroiditis were responsible from hypothyroidism in 4 and 3 patients, respectively. Thyroid autoantibodies were high in 7 patients. Summing these, preoperative thyroid pathology was found to be in 27 (84%) patients. Preoperatively 33 of 54 nodules were aspirated and all were reported as benign. 24 patients had parathyroidectomy with thyroid operation. Among these patients, it was reported that 3 had papillary microcarcinoma (9%), 7 had chronic lymphocytic thyroiditis (21%) and 15 had nodular hyperplasia (47%) histopathologically. PHPT was due to parathyroid adenoma in 31 patients and carcinoma in 1 patient.
CONCLUSION
In our study, there was concurrent thyroid pathology in 84% of patients operated for PHPT. We like to draw attention to 3 patients (9%) who had incidental thyroid malignancy postoperatively. With minimal invasive surgical approach used much more common in recent years, during parathyroid operations, thyroid pathologies are not evaluated particularly Therefore, patients should have detailed neck US and FNAB when needed before operation and surgical approach should be determined considering thyroid pathologies.
42 - Nondiagnostic fine needle aspiration biopsy results - 2009
Uluslararası Bildiriler 11 th European Congress of Endocrinology, Istanbul, Turkey, 25-29 April 2009, P 146. Endocrine Absracts, Volum 20, 2009
ABSTRACT
OBJECTIVE
Fine needle aspiration biopsy (FNAB) is a reliable and safe method to distinguish benign and malignant thyroid nodules. FNAB has two major limitations: nondiagnostic and suspicious cytology results. There is uncertainty about clinical approach to the nondiagnostic FNAB in thyroid nodules. Our aim was to evaluate the ratio and reasons of nondiagnostic results, and the ratio of malignancy in these nodules.
METHOD
2082 patients and 3404 nodules in these patients who referred to the thyroid disease outpatient clinic between 2005-2008 were analyzed, retrospectively. Nodules with suspicious ultrasonographic images and two nondiagnostic cytology were given to surgery. Nodules reported as nondiagnostic in two cytologies, but without suspicious ultrasonographic images were taken to clinical and ultrasonographic follow-up.
RESULTS
FNAB was performed in 3404 nodules. After the first ultrasonography guided FNAB, the rate of nondiagnostic cytology was 9.3% and a second FNAB was repeated in this group. Cytology was reported as nondiagnostic again in 10.8% of these. According to nodule size, 14.6% of infracentimetric nodules and 7.9% of supracentimetric nodules were nondiagnostic (p<0.001). The ratio of nondiagnostic results was 8.9% in solid nodules, 12.3% in mixed nodules and 13.8% in cystic nodules (p=0.08). 14 patients with nondiagnostic cytology underwent operation and histopathologically malignancy ratio was found to be 64.3% (n=9).
CONCLUSION
According to our results,the ratio of nondiagnostic cytologyresults was 9.3%. Nondiagnostic cytology was found to be related to the size of the nodule. In the literature malignancy ratio in nondiagnostic cytology is reported between 9-37% in different studies, but ours was 64.3%. The reason for higher malignancy rates in our study may be preference of surgical management not in all patients with nondiagnostic cytology but in patients with clinically and ultrasonographically suspicious nodules. Considering this result, nondiagnostic cytologies might not be of benign cytology and should be evaluated carefully.
41 - Association of thyroid function tests with thyroid malignancy - 2009
Uluslararası Bildiriler 11 th European Congress of Endocrinology, Istanbul, Turkey, 25-29 April 2009, P 111. Endocrine Absracts, Volum 20, 2009
ABSTRACT
OBJECTIVE
Role of thyroid stimulating hormone (TSH) in thyroid oncogenesis is not clear. There are few trials about relationship of TSH, thyroid hormones and autoantibodies with malignancy. We aimed to investigate thyroid function tests and malignancy in patients evaluated in thyroid disease council and decided to be managed with thyroidectomy.
METHOD
272 patients were included in the study. Hyperthyroid and hypothyroid patients, patients on L-thyroxine and antithyroid treatment and those with previous thyroidectomy were excluded. Thyroid function tests (TSH, free T3, free T4, anti-TPO, anti-TG) were recorded before thyroidectomy. Patients were grouped in 2 according to histopathologic results, benign and malignant; and grouped in 3 according to TSH levels, group 1: TSH<0,9 µIU/mL, group 2: TSH: 0,9-1,49 µIU/mL, group 3: TSH≥1,5 µIU/mL.
RESULTS
There were 224 female and 48 male patients and mean age was 44.4±11.7 (18-75). Histopathologically, there were 174 benign and 98 malign reports.
TSH levels and malignancy was found to be correlated significiantly (p<0.001). Although there was no difference between group 1 and 2, difference between 2 and 3 was significant (p<0.001, OR: 2.87). Malignancy was higher in patients with TSH≥1.5 µIU/mL. Median free T3 was 3.55 pg/ml (1.4-5.24) in patients with benign pathology whereas it was 3.35 pg/ml (1.8-4.79) in patients with malign pathology. There was statistically significant difference (p=0.006, OR: 0.61). Anti-TPO was positive in 17.7% of benign group and 31.1 in malign group. Again, these results were statistically significant (p=0.014, OR: 2.10). Antithyroglobulin was positive in 19.9% and 32.2% of benign and malign patients, respectively (p=0.028, OR: 1.92). Multiple regression analysis also showed TSH and free T3 effect on malignancy.
CONCLUSION
Our results showed that, in euthyroid patients, presence of autoantibody, low free T3 even in normal ranges and TSH levels above 1.5 µIU/ml are all related to malignancy
40 - Concomitant thyroid carcinoma and Hashimoto thyroiditis: effects of thyroiditis on ultrasonographic and histopathologic features of nodules - 2009
Uluslararası Bildiriler 11 th European Congress of Endocrinology, Istanbul, Turkey, 25-29 April 2009, P 107. Endocrine Absracts, Volum 20, 2009
ABSTRACT
OBJECTIVE
Incidence of concomitant thyroid cancer and Hashimoto thyroiditis (HT) is found to be 0.3-58% in different series. In this study, we aimed to find out HT incidence in thyroid cancer patients in our clinic and we tried to determine ultrasonographic and histopathologic features of tumor in these patients.
METHOD
165 patients diagnosed with thyroid carcinoma between 2005-2008 were included in the study. Patients with Graves’s disease were excluded. Preoperative and postoperative datas were evaluated retrospectively.
RESULTS
Patients were grouped into 2 according to the presence of HT histopathologically. In Group I HT was not detected and 129 patients were in this group. Of these, 112 were female and 17 were female with mean age of 46.28±10.86. In this group, mean antithyroidperoxidase antibody (anti-TPO) was 34.59±69.16 IU/mL (0-35 IU/mL) and mean antithyroglobulin antibody (anti-TG) was 82.67±207.42 IU/mL (0-40 IU/mL). In Group II HT was present with thyroid carcinoma and there were 36 (21.8%) patients in this group. 34 of these patients were female and 2 were male, mean age was 42.86±12.67. Mean anti-TPO and anti-TG antibody were 272.83±329.59 IU/mL and 442.32±826.5 IU/mL, respectively. Nodule features in ultrasonography were compared in two groups. There was no statistically significant difference between two groups in regard of echogenity, microcalcification, macrocalcification, halo sign and margin irregularity (p>0.05). Additionaly, histopathologically, tumor diameter, presence of capsule invasion and vascular invasion, multifocality were similar in two groups (p>0.05). Nonetheless, extrathyroidal invasion was found to be more in HT patients (p=0.023). Also, thyroid autoantibodies were significiantly higher in this group (p<0.001).
CONCLUSION
In this study we found HT in 21% of thyroid carcinoma patients. Besides, we concluded that presence of HT has no effect on ultrasonographic appearence of nodules. However, histopathologically in patients with HT, extrathyroidal invasion was more common. This result suggests that tumors may behave more aggressive in the presence of HT.
39 - The ratio of malignancy in patients who underwent thyroidectomy due to follicular lesion/neoplasia - 2008
Uluslararası Bildiriler 11 th European Congress of Endocrinology, Istanbul, Turkey, 25-29 April 2009, P 106. Endocrine Absracts, Volum 20, 2009
ABSTRACT
OBJECTIVE
We aimed to evaluate the frequency of malignancy in patients with follicular lesion or follicular neoplasia in cytological examination.
METHOD
29 patients who had follicular neoplasia or follicular lesion in cytological examination after ultrasound guided thyroid fine needle aspiration biopsy (FNAB) were included in the study. Histopathologic results were evaluated after thyroidectomy in all patients.
RESULTS
There were 28 female and one male patient. Ten of the patients had nodular, 18 had multinodular and one had recurrent multinodular goiter preoperatively. One of the nodules was infracentrimetric, 28 were supracentrimetric. Mean age was 42.27±11.06 (21-65). Postoperatively, thyroid malignancy was determined in 12 patients in histopathologic examination. Therefore, the frequency of thyroid malignancy in patients with follicular lesion/neoplasia was found to be 41.4%. All of malign nodules, except one, were supracentrimetric. Six of the patients had nodular and 6 had multinodular goiter. The distribution of thyroid cancer was as follows; 3 follicular thyroid carcinoma, 7 papillary thyroid carcinoma and 2 follicular variant of papillary carcinoma. Three of the histopathologically benign cases had hashimoto’s thyroiditis, 2 had hurthle cell adenoma, 2 had follicular adenoma and 10 had nodular hyperplasia.
CONCLUSION
It is difficult to differentiate follicular and hurthle cell carcinoma from follicular and hurthle cell adenoma cytologically. These nodules are diagnosed as carcinoma if vascular and capsular invasion is seen histopathologically. Studies showed no benefit of frozen sections on differential diagnosis. In the literature the rate of malignancy in follicular neoplasia/lesion is 6-47%. In our study, we found 41.4% malignancy rate in patients who underwent surgery due to follicular lesion or neoplasia. 75% of the malignant cases were papillary carcinoma. We accept this group of patients as malignant and suggest that total /near total thyroidectomy should be performed.
38 - Gastric adenocarcinoma in an acromegalic patient: a rare association - 2008
Uluslararası Bildiriler 13th Meeting of the European Neuroendocrine Association, Antalya, Turkey, 17-20 October, Abstract Book: PS.96, 2008
ABSTRACT
Gastrointestinal neoplasms, particularly colorectal cancer in acromegalic patients seems to be found in higher incidence than expected. An increased incidence of gastric cancer in acromegaly cases has been suggested in a few published retrospective studies, but neither the prevalence rate of gastric cancer nor the mechanisms of carcinogenesis have been clarified in these reports. We reported a rare case of gastric adenocarcinoma in an acromegalic patient.
CASE: A 44-year-old male patient presented to our department with a gradual increase in the sizes of nose, lips, nasolabial skin folds and forehead as well as increased extremity size over a period of ten years. On admission, typical physical features of acromegaly were noted and he had moderate hypochromic anemia with a hemoglobin level of 9.7 g/dl, red blood cell count of 368x104/mm3 and hematocrit of 28.3%. Growth hormone (GH) and insulin-like growth factor I (IGF-I) levels were high (12 ng/ml and 845 ng/ml respectively). The serum GH levels increased after oral administration of 75gr glucose. Magnetic resonance imaging (MRI) identified a microadenoma 7x4 mm in diameter in pituitary gland (Figure 1).
Figure 1. Pituitary microadenoma 7x4 mm in diameter
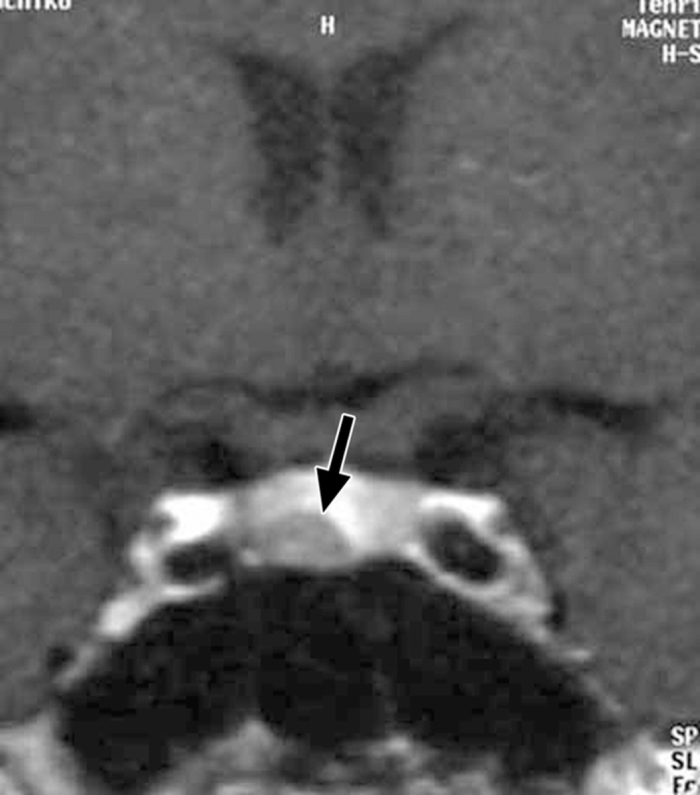
In upper gastrointestinal system endoscopy, a giant ulcer (5x5x1.5 cm) was found localized in small curvature (Figure 2). Endoscopic biopsies were performed. Histopathologic examination of biopsies demonstrated adenocarcinoma. Pre-operative examinations including; colonoscopy, cranial- abdominal and thorax computerized tomography (CT) revealed no evidence of metastasis or any other neoplasms. In the illumination of all these findings, he was diagnosed as acromegaly accompanied by gastric adenocarcinoma.
Figure 2. Malign gastric ulcer in small curvature

Distal gastrectomy with D2 lympadenectomy was performed. Microscopic examination revealed that the lesion was poorly differentiated adenocarcinoma invading subserosal area of the stomach; and metastasis was determined in perigastric lymph nodes. In the postoperative process, 6 cures of chemotherapy and radiotherapy were applied. After the completion of these therapies all the examinations were repeated in terms of pituitary adenoma. Thereafter, an Octreotide LAR 20 mg per month therapy was initiated as primary medication.
CONCLUSION: Although malignancy is among the important factors contributing to the increased mortality rate of acromegalic patients, there is no convincing epidemiological evidence of an association between acromegaly and gastric cancer because of the rare incidence of acromegaly accompanied by gastric cancer. However we recommend that patients with acromegaly should be evaluated not only with colonoscopy but also upper gastrointestinal endoscopy.
37 - The role of inferior petrosal sinus sampling for ACTH-dependent Cushing’s syndrome - 2008
Uluslararası Bildiriler 13th Meeting of the European Neuroendocrine Association, Antalya, Turkey, 17-20 October, Abstract Book: PS.95, 2008
ABSTRACT
BACKGROUND: The differential diagnosis of adrenocorticotropin (ACTH) dependent Cushing's syndrome remains a challenging issue for clinical endocrinologists. In this respect, bilateral inferior petrosal sinus sampling (IPSS) appears to be the most sensitive and specific test. Here, we report our 13 patients experience of analyzing the performance of IPSS, both in the correct diagnosis and in the precise lateralization of tumors in patients with Cushing's disease (CD).
METHODS: Thirteen women with newly diagnosed CD between March 2005 and March 2008 in our center were evaluated in this study. The mean age was 41.5 years (23-57). In all patients, imaging of the pituitary and adrenal was obtained by magnetic resonance, and a pituitary microadenoma was observed in twelve patients. Besides, adrenal adenoma was observed in five patients. Four patients had previously undergone transsphenoidal hypophysectomy and had a recurrence thereafter. With CRH stimulation, IPSS was performed in all patients by inserting a catheter in the right and left inferior petrosal sinus for ACTH assay via a femoral vein puncture. An inferior petrosal sinus/ peripheral ACTH ratio ?2 at base line or ?3 after CRH injection indicated a pituitary origin of ACTH secretion and an interpetrosal ACTH gradient ?1.4 at baseline or after CRH injection indicated evidence of lateralization.
RESULTS: Central to peripheral ACTH gradient of ?2 was found in 10/13 patients at base line and gradient of ?3 in all patients after CRH stimulation, confirming pituitary source of ACTH excess. Interpetrosal sinus gradient of ?1.4 was observed in 10/13 patients at base line and in all patients after CRH stimulation. One of the patients didn't accept surgery. Two of 12 patients who were operated had active disease in their follow-ups. IPSS was repeated in one of the patients, and was given to surgery the second time. The patients was accepted clinically cure in follow up. The second patients, who had previously undergone transsphenoidal hypophysectomy and had a recurrence was not operated and treated medically.
CONCLUSIONS: For patients with CD, surgical removal of the pituitary adenoma is the treatment of choice. Thus, localization of the source of ACTH secretion is critical in guiding timely treatment decisions. Inferior petrosal sinus sampling is considered to be the gold standard for confirming the origin of ACTH secretion in patients with Cushing\'s syndrome.
36 - Cushing’s disease with Unilateral functional surrenal adenoma - 2008
Uluslararası Bildiriler 13th Meeting of the European Neuroendocrine Association, Antalya, Turkey, 17-20 October, Abstract Book: PS.94, 2008
ABSTRACT
CASE: A 46 year-old female patient with a history of type 2 diabetes mellitus since 10 years admitted to our outpatient clinic for blood sugar regulation. She was hospitalized for signs and symptoms of Cushing\’s syndrome. She also had hypertension and hyperlipidemia. In laboratory examination, basal cortisol 27,3 μg/dl (8-25μg/dl), midnight cortisol 10.3 μg/dl (4-12,5μg/dl) and plasma ACTH level was 15 pmol/L. Cortisol was not suppressed by 1 mg and 2 mg dexamethasone (8,25μg/dl and 6,6μg/l, respec tively), and was suppressed by high-dose dexamethasone (3,22μg/dl). Magnetic resonance imaging (MRI) revealed a pituitary lesion of 4 mm in diameter. Inferior petrosal sinus sampling (IPSS) was performed. The ratio of basal inferior petrosal sinus/peripheral ACTH and interpetrosal ACTH gradient before CRH stimulation were 7.46 and 3.29 respectively. The ratio of inferior petrosal sinus/peripheral ACTH and interpetrosal ACTH gradient after CRH stimulation were 11.72 and 6.82 respectively. These results showed pathology at the right side of the pituitary gland. Transsphenoidal resection was performed. After the surgery clinical regression of Cushing\'s syndrome and normalization of fasting cortisol was obtained (11.6μg/dl). Cortisol was suppressed by 2 mg dexamethasone (1.7μg/dl). The patient was accepted to be cured. Six months after the operation the patient was hospitalized because of blood sugar irregulation and symptoms of Cushing\'s syndrome. Basal cortisol level was 20.4μg/dl. Cortisol levels after 2 and 8 mg dexamethasone suppression tests were 6.6 μg/dl and 8.21 μg/dl, respectively. Pituitary MRI was normal. Adrenal MRI showed a 3,5x2 cm adenoma on the left adrenal gland. Adrenal cortex scintigraphy with 19-iodocholesterol (I-131) was performed. There was a focal activity increase in the area where the lesion was seen by MRI. Left adrenalectomy was performed by the urologists. Histopathologic study supported the diagnoses of adenoma. Three months after the operation the dynamic test were repeated. Fasting plasma cortisol was 7.61μg/dl and 1.7μg/dl after 2 mg dexamethasone suppression. Symptoms and signs of hypercortisolism gradually disappeared. The patient was clinically accepted cured and was added to the follow up list. In this case we think that to be exposed to ACTH for a long period due to Cushing's disease, the adrenal gland developed unilateral macronodular hyperplasia and it gained autonomy to produce cortisol.
35 - Primary thyroid disorders in patients with Cushing’s disease - 2008
Uluslararası Bildiriler 13th Meeting of the European Neuroendocrine Association, Antalya, Turkey, 17-20 October, Abstract Book: PS.93, 2008
ABSTRACT
BACKGROUND: It has been reported that, thyroid nodule prevalence is increased in patients with endogenous hypercortisolism. Furthermore, in a small number of studies it has been shown that after resolution of hypercortisolism, there is a worsening of autoimmune thyroid disease.
PATIENTS: Thirteen patients, who were diagnosed as Cushing's disease in our clinic between 2005-2008 participated in the study. Four patients had undergone transsfenoidal hypophysectomy and had relapse. Nine patients had been newly diagnosed. The patients were evaluated with; sT3, sT4, TSH, anti-thyroperoxidase antibodies (AntiTPO Ab), anti-thyroglobulin antibodies (AntiTg Ab), thyroid ultrasonography, thyroid scintigraphy and ultrasonography guided thyroid fine needle aspiration biopsy (US-FNA), if necessary.
RESULTS: All of the patients were female. The median age was 41.5 years (23-57). Six patients had multinodular goiter (46%). With scintigraphic evaluation the nodules were hypoactive. US-FNA biopsy was performed to ultrasonographically suspicious nodules. All the biopsy results were cytologically benign. One patient who had multinodular goiter with symptoms of compression was operated. Three (23%) of the patients had high levels of Anti TPO Ab and Anti Tg Ab. Thyroid ultrasonography was consistent with thyroiditis. One of these patients had subclinical hypothyroidism and the other had subclinical hyperthyroidism. When all of the patients were evaluated, the frequency of primary thyroid disease among patients with pituitary Cushing's disease was 69%.
CONCLUSION: In patients with pituitary Cushing's disease, the risk of developing primary thyroid disease, particularly nodular thyroid disease, is increased. This may be due to the effect of corticotroph cells, which may be stimulating thyrosit proliferation at the same time. We concluded that, patients who are suspected to have Cushing syndrome must also be evaluated for thyroid pathologies.
34 - Xanthoma disseminatum, hypothalamical mass, diabetes insipidus and hypopituitarism: a case of non-langerhans cell histiocytosis - 2008
Uluslararası Bildiriler 13th Meeting of the European Neuroendocrine Association, Antalya, Turkey, 17-20 October, Abstract Book: PS.92, 2008
ABSTRACT
Xantoma disseminatum (XD); a rarely seen normolipemic bening granulomatous disease characterized with mucocutaneus xantoma, is a subgroup of non-Langerhans cell histiocytosis (NLCH). In this report, a case with diabetes insipidus (DI) and hypopituitarism is presented.
CASE: A 16 years old female patient referred to our hospital by following complaints; no menstruation within the last year, gaining weight, polidipsia, poliuria, many yellow-brownish papular lesions manifested at cervical, periorbital, axillary and genital regions (Figure 1). It was learned that initially lesions arose 1.5 year ago, and by the time she referred they have increased in amount and size. During examinations, she was found to have a body mass index as 34.7 kg/m2. In laboratory test, parameters of complete blood counting and biochemical examinations were in normal ranges. After basal hormone levels were studied and dynamical tests were performed, results showed up that she had secondary hypothyroidism, hypogonodothropic hypogonadism, growth hormone deficiency and central DI (Table 1). In MRI screening of hypophyseal region, a mass in 15x8 mm sizes localized at hypothalamohypophysial tract was detected (Figure 2). She had a normal visual examination. In order to diagnose the mass pathologically a biopsy was carried out by transsphenoidal way. But the material taken was not found to be adequate for diagnostic evaluation. At the same time, a biopsy was performed on skin lesions and the result of pathologic analysis was coherent with NLCH. Then, a discriminative process was executed by evaluating lesions in amount, localization, and morphologic and histopathologic patterns. In conclusion, she was diagnosed with XD. Thereafter, replacement therapies intended for hypothyroidism, hypogonadism and DI were initiated. For hypothalamic mass and skin lesions 60 mg/d methyl prednisolone was started and its doses had been gradually reduced to maintenance dose of 4 mg/d. MRI screening performed at 6th month of therapy didn’t show any differences in mass sizes. Hence, medical therapy was converted to cyclophosphamide 50 mg/d. Clinical follow up of this patient is still going on.
Hypopituitarism is a rare condition seen along 1% of granulomatous diseases. This case with XD accompanied by hypothalamic mass, DI, hypopituitarism was presented for its remarkable skin findings and clinical view.
Figure 1.Axillary yellow-brownish papular lesions

Figure 2.The mass in 15x8 mm sizes localized at hypothalamohypophysial tract
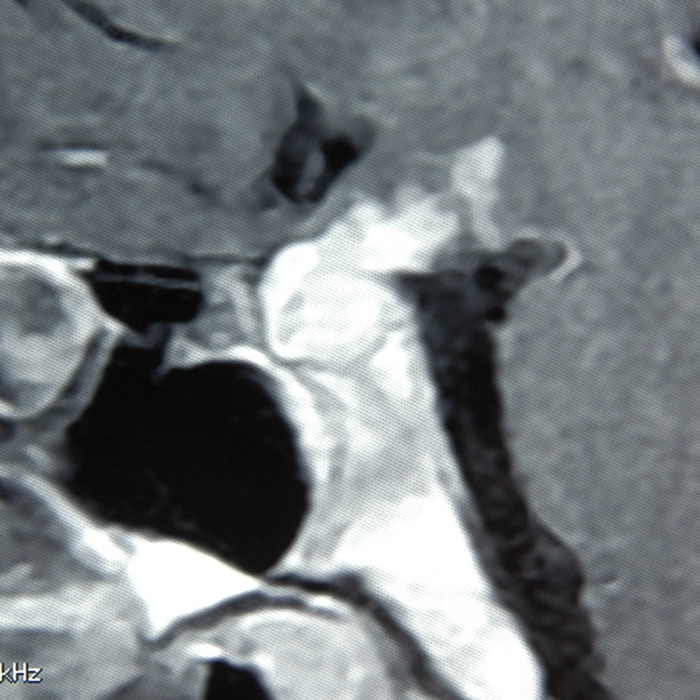
Table 1. Endocrinological evaluation of the patient
A.U. | |||
Age | 16 | ||
Height/ Weight | 167 cm/ 97kg | ||
BMI | 34.7 kg/m2 | ||
Pubic hair develpoment (Tanner) | Stage II | ||
Breast development (Tanner) | Stage II | ||
IGF-1 (131- 278 ng/mL) | 67 ng/ml | ||
Basal Hormonal Status | |||
Pituitary | GH (0-10 ng/mL) | <0.05 | |
TSH (0.4-4.0 uIU/mL ) | 0.216 | ||
LH (1.1-14.7 mIU/mL ) | <0.10 | ||
FSH (2.8-11.3 mIU/mL) | <0.10 | ||
PRL (19.5-25 ng/mL) | 18.2 | ||
ACTH (0-46 pg/mL) | 3.0 | ||
Thyroid | fT3 (1.57-4.71 pg/mL) | 2.85 | |
fT4 (0.85-1.78 ng/dL) | 0.70 | ||
Adrenal | Cortisol (8-25 μg/dL) | <1.0 | |
Gonad | Progesteron (0-1.13 ng/mL) | <0.20 | |
Estradiol (27-246 pg/mL) | 31.8 | ||
Endocrine Tests | |||
İnsulin Hypoglycemia Test 0.1 U/kg ıv | GH response | (-) | |
Cortisol response | (-) | ||
TRH Test | (-) | ||
GnRH Test | (-) | ||
Water deprivation test | Santral DI | ||
Other Tests | |||
Visual field examination | Normal | ||
Neurologic examination | Normal | ||
Echocardiography | Normal | ||
33 - An acromegalic woman first diagnosed in pregnancy - 2008
Uluslararası Bildiriler 13th Meeting of the European Neuroendocrine Association, Antalya, Turkey, 17-20 October, Abstract Book: PS.91, 2008
ABSTRACT
Reports of pregnancy in acromegalic women are uncommon. Less than 100 pregnancies have been reported, in which a case of acromegaly first diagnosed in pregnancy is fairly rare. We report a case of an acromegalic woman who had gestational diabetes as an initial symptom.
CASE: A 30-year-old women in 25-week gestation who previously gave birth to two healthy girls was referred from gynecology department with gestational diabetes mellitus. She complained about polyuria. In laboratory examination; fasting blood glucose: 143 mg/dl and postprandial (1st hour) blood glucose: 195 mg/dl were. On physical examination, she had a coarse face, hands, feet and heel-pad thickness. Random growth hormone (GH), insulin-like growth factor-I (IGF-I) and prolactin (PRL) levels were very high (25.3 ng/ml, 1859 ng/ml and 126 mg/ml respectively). Oral administration of glucose paradoxically increased the serum GH level. Also, oral glucose tolerance test confirmed the diagnosis of gestational diabetes mellitus. An ophthalmological examination did not confirm impairment in visual acuity, and visual field examination was normal. Magnetic resonance imaging (MRI) identified a macroadenoma 18x13x11 mm in pituitary fossa, and the mass was not compressed optic chiasm. Her thyroid and adrenal functions were normal (Figure 1).
This endocrine data suggested that her tumor was a GH-secreting adenoma or GH and PRL co-secreting adenoma. We proposed dopamine agonist treatment, bromocriptine at 27-week gestation but the patient refused. Because of a considerable risk of pituitary apoplexy, she was periodically hospitalized and her visual field examination was done. Gestational diabetes was controlled with diet and insulin therapy. She reached full term, and had a caesarian section and delivered a 4200-gr-baby boy with Apgar score of 9. Her baby had no serious problem. After delivery, she also refused operation and/or medical therapy for six months. She is still breast-feeding her baby.
CONCLUSION: Although pregnancy in acromegaly is a rare event, it may be achieved in acromegalic women with or without treatment. Besides, gestational diabetes mellitus may be initial symptom of disease such as our patient.
32 - Recovery of growth hormone secretion and beginning of the puberty following cabergoline treatment of macroprolactinoma - 2008
Uluslararası Bildiriler 13th Meeting of the European Neuroendocrine Association, Antalya, Turkey, 17-20 October, Abstract Book: PS.89, 2008
ABSTRACT
Pituitary adenomas constitute between 1.1 and 6% of all intracranial tumors in pediatric and adolescent age. Prolactin (PRL) secreting pituitary adenomas rarely occurs in this age group, with various incidences reported to range from 0.6 to 6.2% of pituitary adenomas in all age groups, and from 19.7 to 72.2% of pituitary adenomas in pediatric/ adolescent patients. PRL secreting pituitary adenomas frequently are macroadenomas in the prepubertal and postpubertal ages. Their mass effect frequently cause delayed puberty and growth hormone deficiency (GHD). In this report we represent recovery of growth hormone secretion and beginning of the puberty following the treatment of macroprolactinoma with cabergoline in an adolescent.
CASE: A macroprolactinoma accompanied by symptomatic chiasmal compression, short stature and delayed puberty was diagnosed in a 15 year- old male patient. Height, bone age, height SDS and pubertal stage were as fallows respectively: 141.5 cm, 12 years 6 months, -5.079 and PI. Magnetic resonance imaging demonstrated a mass 25x25x18 mm in diameter occupying suprasellar region and also compressing optic chiasm (Figure 1).
Figure 1.Before cabergoline treatment

Bromocriptine 10 mg per day was applied for 3 months without any response in terms of prolactin (PRL) level (>150 ng/mL) or tumor shrinkage, so cabergoline was initiated in an incremental regimen up to a maintenance dose of 2 mg per week. After 9 months of cabergoline treatment PRL levels decreased in normal range and maximum tumor shrinkage was observed. After 20 months of cabergoline treatment only a tumor remnant 3x2 mm in diameter in the sellar floor was observed (Figure 2).
Figure 2.After 20th of cabergoline treatment
.png)
The patient was asymptomatic, and visual field examination was normal. Insulin tolerance test was repeated. There was no response, and recombinant growth hormone treatment (0.2 mg/ kg/ week) was added to the therapy. GH therapy improved the growth rate (21 cm in 18 months), and no expansion of the macroadenoma was observed during one year of combined treatment (Figure 3).
Figure 3.After combined cabergoline and GH treatment
GH therapy was interrupted at 18th month. The hypophyseal and target hormones were reevaluated after two months of an un-medicated term. FSH, LH, free testosterone, GH and IGF-1 levels were in normal ranges as against with the age group of our patient. ITT was performed again. Peak growth hormone response was 16 ng/dL. His puberty stage was determined as PIII.
CONCLUSION: Prolactinomas are rare in children and adolescent. Delayed puberty and GHD are common findings in young patients with macroprolactinoma. However, normalization of GH and gonadotrophic hormone secretion after therapy has also been reported. Treatment with dopamine agonists (bromocriptine and cabergoline) is effective in normalizing PRL levels and in shrinking tumor mass in the majority of adult patients with prolactinoma. In children and adolescents, dopamine agonists, especially cabergoline, have been used successfully be several investigators, such as our patient. In addition, the combined treatment with cabergoline and rhGH seems to be safe and highly effective in patients with GHD. Nevertheless, careful monitoring and on-going evaluation are necessary. In conclusion, GH and gonadotrophin secretion may recover following a successful reduction of prolactin levels and shrinkage of adenoma after cabergoline therapy in macroprolactinoma.
31 - Reversibl diabetes mellitus during growth hormone therapy in an adolescent patient - 2008
Uluslararası Bildiriler 13th Meeting of the European Neuroendocrine Association, Antalya, Turkey, 17-20 October, Abstract Book: PS.89, 2008
ABSTRACT
Recombinant growth hormone (rhGH) is established treatment of growth hormone deficiency in children and adults. Growth hormone (GH) contributes to insulin resistance. There are several sites in the insulin-signaling pathway at which GH can induce anti-insulin effects. Thus type 2 diabetes mellitus (DM) may be induced by rhGH treatment. Here we describe an adolescent patient with short stature due to GH neurosecretory dysfunction with elevated fasting and daily profile glucose concentrations after rhGH treatment.
CASE: A 15-year-old girl had delayed puberty and short stature due to GH neurosecretory dysfunction. The family history was negative for diabetes mellitus. Height, weight, body mass index, bone age, and height SDS was as fallows respectively: 138 cm, 41 kg, 22 kg/m2, 10 years, and -3.412. The patient was still prepubertal. Growth velocity was only 1.5 cm/year before treatment. Target height was estimated to be at the 25th percentile, and when the patient’s height dropped below the 3rd percentile, recombinant GH (rhGH) treatment was administrated standard dose (0.2 mg/kg/wk), subcutaneously for six days. Before the rhGH treatment, fasting and postprandial serum glucose levels, and hemoglobin A1c (HBA1c) were in normal ranges.
Table1. Basal status of patient before rhGH treatment
A.S | |
Age | 15 |
Height/ Weight | 138 cm/ 41kg |
BMI | 22 kg/m2 |
Bone age | 10 |
HSDS | -3.412 |
Growth velocity | 1.5 cm/year |
IGF-1 (131- 278 ng/mL) | 85 |
GH (0-10 ng/mL) | 0.10 |
TSH (0.4-4.0 uIU/mL) | 1.46 |
Kortizol (8-25 μg/dL) | 15 |
Fasting Blood Glucose (mg/dL) | 84 |
Postprandial Blood Glucose (mg/dL) | 125 |
HbA1C (%) | 5.8 |
On routine outpatient follow up 3 months later, the patient showed increased fasting whole-blood glucose level (158 mg/dL). Postprandial glucose level and HBA1c were also elevated (226 mg/dL and 7.1%, respectively). Weight loss was not noted, but she complained about polyuria. Glutamic acid decarboxylase, islet cell and insulin antibodies were not detected. Because of these findings, the patient was hospitalized and rhGH was discontinued. Fasting and postprandial glucose levels decreased in two weeks after discontinuation of rhGH. We applied oral glucose tolerance test two months after withdrawal of rhGH. Glucose tolerance test results were evaluated as normal.
CONCLUSION: GH contributes to insulin resistance but few studies have examined whether there is a relation in children between GH therapy and DM. In a retrospective study of nearly 2000 Japanese children who had received GH treatment for at least 6 months, only three were found to have glucose intolerance. Based on the limited information available in 1993, the European Society of Pediatric Endocrinology issued a statement that DM is rare among GH-treated children, with a prevalence that did not seem to differ from that of the population. In the KIGS study, authors reported that an increased incidence of diabetes mellitus and impaired glucose tolerance in young people treated with rhGH; and type 2 diabetes was six times more frequent in children on rhGH treatment than normal children. In our series, including 21 patients, we observed diabetes mellitus in only one patient (%4.76), and glucose intolerance was reversible following discontinuation of rhGH. We suggest that fasting and postprandial glucose, and also HBA1c levels should be measured before and after initiation of rhGH therapy.
30 - Evaluation of final height in adolescent patients with growth hormone defiency who were treated with growth hormone replacement therapy - 2008
Uluslararası Bildiriler 13th Meeting of the European Neuroendocrine Association, Antalya, Turkey, 17-20 October, Abstract Book: PS.87, 2008
ABSTRACT
OBJECTIVE: Growth Hormone Deficiency (GHD) is an important cause of growth retardation and short stature. The rate of occurrence has been reported in the literature between 1/3480 and 1/30.000. GHD may be idiopathic or associated with organic causes, such as tumor, surgery, trauma or irradiation of the sellar area, and it may be with or without multiple pituitary hormone deficiency. The first goal of GH treatment in GHD is to obtain an optimum final height. Early diagnosis and initiation of GH treatment, final height can be normalized in most patients with GHD. The aim of this study was to evaluate the growth response to GH treatment in adolescent patients with GH deficiency that treated in our center.
MATERIAL and METHOD: We evaluated 21 patients who were subsequently diagnosed to have GHD in the endocrinology department of our hospital between October 2002 and March 2008 retrospectively. The diagnosis of GHD was based on auxological and biological criteria; exclusion of other diseases, and a GH peak level of <10 μg/dl in at least two stimulation tests, usually the insulin tolerance test and L-DOPA test done by standard methods. Sex steroid priming was applied for boys and girls if they had pubertal development < genital stage 2 or breast stage < 2, independently of bone age. Hypothyroidism was defined as low or low- normal serum TSH concentration and free T3 concentrations. Plasma ACTH and serum cortisol values were measured in the morning. ACTH deficiency was defined as either a morning serum cortisol concentration of less than 3.6 μg/dl or an impaired cortisol serum concentration rise inferior to 20 μg/dl during insulin- induced hypoglycemia. Hypogonadism was confirmed in both sexes by lack of puberty and no increase in FSH and LH in response to gonadotropin releasing hormone. Cranial imaging studies, with special emphasis on the hypothalamo- pituitary region, were performed in all patients using MRI. From a total of 21 patients (18 boys, 3 girls) treated for GH deficiency, to date, 16 boys have reached their final height. At the beginning of the treatment, mean chronological age 16.6±1.07 years (15-18), mean height 140.5±12.7 cm (120-155), growth velocity 1.64±1.59 cm/year (0-3.5), and mean height standard deviation score (SDS) for chronological age -4.60±2.06 were. Four patients had isolated GH deficiency (IGHD) and 12 had multiple pituitary hormone deficiency (MPHD). Peak serum GH concentrations were 3,4±1,2 ng/ml in insulin tolerance test and 0.27±0.20 ng/ml in L-DOPA test. All patients were prepubertal. Bone ages were between 8-14 years. Recombinant GH (rhGH) treatment was administrated standard dose (0.2 mg/kg/wk), subcutaneously for six days. Patients with MPHD were receiving conventional replacement treatment. Average follow-up period was 41 months (18-100). Patients had completed a course of treatment in the chronological age of 19.7±2.27 years (17-24). At the end of the treatment a significant improvement in height was shown. The mean final height was 164,0±4.65 cm (155-171). Height SDS for chronological age -1,20±0.46, and bone age 17 years were. Difference between initial and final height SDS was significant (p<0.001).
Table1.Characteristics of patients at diagnosis and time of GH withdrawal
Diagnosis | Time of GH Withdrawal | |
Chronological Age (yr) | 16.6±1.07 | 19.7±2.27 |
Median Bone Age (yr) | 9.0 | 17 |
Height (cm) | 140.5±12.7 | 164,0±4.65* |
Height SDS | -4.60±2.06 | -1,20±0.46* |
Body Mass Index SDS | 0.2 | -0.1 |
Height velocity (cm/yr) | 1.64±1.59 | 4.5±2.56* |
*The differences were significant (p<0.01)
CONCLUSION: When factors that could have an influence on the growth response were analyzed separately in the prepubertal and pubertal children, it was shown that younger age and lower height SDS at onset of therapy seem to predict a better growth response in prepuberty, which is in compliance with published reports. On the other hand, older age, lower height SDS seems to be correlated with a better growth response in puberty. The reason why older children in the pubertal group responded better is not clear. GH deficiency was diagnosed and treated fairly late in our patients. Our all patients were prepubertal. Nevertheless, patients have reached above the third percentile of the normal Turkish population. Also, the height and chronological age of the patients at the start of the treatment significantly correlated with final height. Our data confirmed that early diagnosis and treatment is important to complete catch-up growth in patients with GH deficiency.
29 - Effect of a six-month treatment with octreotide long acting repeatable(LAR) on mean platelet volume in patients with acromegaly - 2008
Uluslararası Bildiriler 10th European Congress of Endocrinology, Berlin, Germany, 3-7 May, Endocrine Abstract Vol:16, P431, 2008
ABSTRACT
INTRODUCTION:
Mean platelet volume (MPV) is an indicator of platelet sizes, and an indirect marker of platelet function and activity. Large platelets are reported to be more active, causing microaggregations in microvascular areas. This is a risk factor for developing cardiovascular disease (CVD). Patients with acromegaly have an increased mortality from atherosclerosis and CVD when compared with the healthy population, mainly after the age of 45 years. Cellular proliferation-stimulating effect of GH directly on myocardium through insulin like growth factor-1 (IGF-1); presence of hypertension, glucose intolerance and diabetes mellitus more commonly seen in patients with acromegaly than normal population and increased fibrinogen levels possibly contribute to increased CVD. Octreotide, the first somatostatin analogue introduced for clinical use, is a more potent inhibitor of growth hormone, glucagon, and insulin than somatostatin. Treatment with Octreotide-Long-Acting Repeatable (LAR), that suppresses GH and IGF-1 levels in acromegalic patients has been shown to partially reverse the abnormalities of cardiac muscle structure and function, also markedly improving cardiovascular risk parameters. In literature, there is no study about the effect of the disease on platelet count and MPV in patients with acromegaly. Also, no data is currently available on the effect of long-term treatment with somatostatin analogues, such as Octreotide LAR, on platelet count and MPV in acromegaly. In the present study, we aimed to evaluate MPV in patients with acromegaly, and to investigate the effect of a long-acting somatostatin analogue, Octreotide LAR, on platelet counts and MPV after 6-month therapy in active acromegalic patients.
MATERIALS AND METHODS:
Study Population
Twenty-five patients with acromegaly (16 women; 9 men; mean age, 43.8±13.5 years) diagnosed and followed up in our center between the years 2002 and 2007; and a control group of 30 subjects similar for gender, mean age, mean body mass index (BMI) and co-morbid diseases (diabetes mellitus and hypertension) were included in the study. Acromegalic patients; before treated with somatostatin analogs, with known coronary artery disease, describing unstable angina pectoris, having electrocardiography (ECG) changes in favor of ischemia, rhythms other than sinus; with renal or hepatic dysfunction (creatinine >2.5 mg/mL, AST and ALT >2 times of normal upper limit); and thrombocytopenia were excluded.
Study Protocol
Acromegaly was diagnosedin keeping with typical clinical features, elevated serum GH levels during an 8 h time course, not suppressible below 2 mU/L (1 μg/L) after a 75 g oral glucose administration, and elevated plasma IGF-I levels for age. In the magnetic resonance imaging of hypophysis all patients had macroadenomas. Firstly, mean age, BMI, GH, IGF-1, total cholesterol, LDL- cholesterol, HDL- cholesterol, triglycerides, fibrinogen levels, platelet counts, and MPV values of the patients, by the time they were first diagnosed for acromegaly, were compared to the data of the control group. Eighteen patients of those had been unsuccessfully treated with surgery.
At the second stage of the study, the values of this patients with active acromegaly in postoperative period who receiving Octreotide LAR 20-30 mg/month for at least 6 months for secondary treatment, were compared to the data of the control group and
control values at 6th month of the therapy.
Statistical Analysis
Data were analyzed with the SPSS software version 13.0 for Windows. Continuous variables were reported as mean ± standard deviation, categorical variables as percentages. Differences in baseline characteristics between patients and control group were assessed by t-test for continuous variables and χ2 test for binary variables. Temporal change of parametric data was evaluated by paired sample’s t-test. All tests were two-sided with a 0.05 significance level.
RESULTS:
Comparative data of demographic data and laboratory characteristics of both patient and control groups are shown in Table 1. Total cholesterol, LDL- cholesterol, triglyceride and fibrinogen levels were higher, while HDL- cholesterol levels were lower in patients than in controls. When MPVs were compared as a marker of platelet functions, no significant difference was detected between acromegalic patients and control group (8.90±1.48 vs 8.81±1.26, p>0.05). Data of laboratory characteristics of postoperative-active 18 patients and control groups are shown in Table 2. After 6 months of treatment with Octreotide LAR, a decrease in GH, IGF-1, LDL- cholesterol, triglyceride and fibrinogen levels were observed. When pretreatment values of 18 patients receiving octreotide LAR for at least 6 months were compared with the values at month 6 of the therapy, involution rate observed in MPV (8.93±1.25 vs 8,49±1.21, p<0.05) were found statistically significant.
DISCUSSION:
The results of the present study demonstrate that no difference is observed in MPV of acromegalic patients and control group. However, following a 6-month therapy with Octreotide LAR, along with decreased GH, IGF-1, LDL-cholesterol, triglyceride and fibrinogen levels, involution in MPV was detected. Large platelets are known to be more active, contain denser granules and α-granules, produce more prothrombotic factors like thromboxane B2, and release more serotonin and β-thromboglobulin than smaller platelets, and cause microaggregations particularly in microvascular areas.. So far as we know, for the first time, we observed that acromegaly affected on neither platelet counts nor sizes at the end of our study. Besides, as a speculative outcome, we considered that treatment with Octreotide LAR could be a factor decreasing cardiovascular morbidity and mortality through indirect antiaggregant effect by shrinking MPV in acromegaly patients. We consider that this effect on platelet volume should be investigated with in vitro and in vivo studies and along with MPV, other factors affecting cardiovascular morbidity and mortality in acromegalic patients should be evaluated with multivariate analyses after long-term treatment follow-ups.
Table1.Comparative data of demographic and laboratory characteristics of patient and control groups
Patients (n=25) | CONTROLS (n=30) | p | |
Age (year) | 43.8±13.5 | 41.7±12.8 | NS |
Gender (F/M) | 16/9 | 19/11 | NS |
BMI (kg/m2) | 27.5±7.8 | 26.9±8.9 | NS |
DM | 4/25 | 6/30 | NS |
Hypertension | 9/25 | 11/30 | NS |
GH (ng/mL) | 12.7±5.2 | 0.9±0.05 | <0.001 |
IGF-1 (ng/mL) | 687.4±244.7 | 316.5±105.4 | <0.001 |
Total cholesterol (mg/dL) | 240.4±55.9 | 185.7±32.5 | <0.01 |
LDL- cholesterol (mg/dL) | 119.3±44.4 | 89.3±15.4 | <0.05 |
HDL- cholesterol (mg/dL) | 39.9±11.3 | 41.3±9.8 | NS |
Triglyceride (mg/dL) | 150.8±16.4 | 99.6±10.7 | <0.01 |
Fibrinogen (mg/dL) | 351.4±38.7 | 256±43.8 | <0.01 |
Platelet (x109/L) | 270.5±59.9 | 263±51 | NS |
MPV (fL) | 8.90±1.48 | 8.81±1.26 | NS |
Table2.Biochemical and hormonal features in postoperative- active 18 patients before and after 6 months of treatment with Octreotide LAR at the dose of 20-30 mg/month and in controls
CONTROLS (n=30) | PATIENTS (n=18) | P | ||
Before | After | |||
GH (ng/mL) | 0.9±0.05AB | 14.6±5.8 | 6.3±3.7 | <0.001 |
IGF-1 (ng/mL) | 316.5±105.4AB | 717.8±239.6 | 416.5±178.9 | <0.001 |
Total cholesterol (mg/dL) | 185.7±32.5CD | 238.7±48.7 | 229.3±35.3 | NS |
LDL- cholesterol (mg/dL) | 89.3±15.4E | 113.8±29.8 | 99.7±18.6 | <0.05 |
HDL- cholesterol (mg/dL) | 41.3±9.8 | 38.9±8.7 | 40.5±10.6 | NS |
Triglyceride (mg/dL) | 99.6±10.7ED | 141.5±14.6 | 126.4±11.8 | <0.05 |
Fibrinogen (mg/dL) | 256±43.8CD | 346.8±35.4 | 284.3±21.8 | <0.05 |
Platelet (x109/L) | 263±51 | 268.7±54.7 | 266.1±49.9 | NS |
MPV (fL) | 8.81±1.26D | 8.93±1.25 | 8.49±1.21 | 0.042 |
AP<0.001 vs. patients before Octreotide LAR treatment, BP <0.001 vs. patients after Octreotide LAR treatment,
CP <0.01 vs. patients before Octreotide LAR treatment, DP <0.05 vs. patients after Octreotide LAR treatment,
EP <0.05 vs. patients before Octreotide LAR treatment.
28 - Assesment of left ventricular functions by tissue Doppler echocardiography in patients with Cushing’s disease - 2008
Uluslararası Bildiriler 10th European Congress of Endocrinology, Berlin, Germany, 3-7 May, Endocrine Abstract Vol:16, P32, 2008
ABSTRACT
INTRODUCTION:
Cushing’s disease (CD) results from hypersecretion of ACTH by an adenoma or hyperplasia of pituitary corticotroph cells, and is the most frequent cause of endogenous hypercortisolism. Endogenous and exogenous hypercortisolism is known to be associated with an increased mortality rate for cardiovascular accidents, probably due to the obesity, hypertension, impaired glucose tolerance or diabetes mellitus, hyperlipidemia, and hypercoagulability. Until now, in limited echocardiographic studies, a high prevalence of left ventricular (LV) hypertrophy and concentric remodeling has been reported. Tissue Doppler imaging (TDI) is an echocardiographic method that allows quantitative measurements of the myocardial contraction and relaxation velocities of a selected myocardial segment. No publication was encountered in the literature investigating the TDI measurements of heart in patients with active CD. The aim of present study was to verify whether TDI could contribute to a better understanding of the natural history of cardiomyopathy in active CD, through its enhanced sensitivity to diastolic dysfunction, and identifying preliminary regional signs of systolic dysfunction, before the appearance of clinical symptoms of cardiac pathologies.
MATERIALS AND METHODS:
Study Population
Eleven women with newly diagnosed CD, and 15 control cases, purposely matched for gender, age, body mass index (BMI) and co-incidental diseases (hypertension, hyperlipidemia, impaired glucose tolerance or diabetes mellitus) were enrolled in this cross-sectional study. Patient profiles at the time of diagnosis are summarized in Table 1.
Echocardiography
Conventional echocardiography and TDI examinations were performed with Vingmed System 7 (Vivid 7 Pro; Horten, Norway) using a 2.5-to 3.5- Mz transducer, and carried out by a single experienced cardiologist. Echocardiographic measurements were taken with patient in the left lateral decubitis positing, according to the recommendations of American Society of Echocardiography.
Statistical Analysis
For the statistical analysis of the study, SPSS 13.0 packet program (SPSS Inc., Chicago, IL) was used. Values of P<0.05 were accepted as statistically significant.
RESULTS:
Demographic and laboratory data of study group with comparative results are listed in Table 2.
The results of conventional echocardiographic examinations are shown in Table 3. IVSd (10.9 ±1.4 mm v 9.4 ±1.0 mm; P=0.006) and PWd (10.4 ±1.2 mm v 9.2 ±1.3 mm; P=0.02) were higher in patients with CD than controls. TDI measurements are summarized in Table 4. E‘ml, E‘ms, E‘ml/A‘ml ratio (0.91 ±0.14 v 1.21 ±0.38; P=0.01), and E‘ms/A‘ms ratio (0.88 ±0.14 v 1.13 ±0.36; P=0.02) were significantly lower, and PCT‘ml/CT‘ml ratio and PCT‘ms/CT‘ms ratio were higher, CT‘ms were longer in patients with CD than controls. There were significant differences between patients and control group on lateral and septal annulus IVA. IVAl and IVAs were significantly lower in patients with CD than the control group. Correlation analysis showed that IVAl correlated positively with Sml (r=0.58; P=0.002) and IVAs correlated positively with S‘ms (r=0.51; P=0.008) (Figures 1 and 2), but there were no correlations between IVAl and CT‘ml, PCT‘ml/CT‘ml ratio and also IVAs and CT‘ms, PCT‘ms/CT‘ms (P>0.05).
DISCUSSION:
The present study showed that TDI might facilitate the diagnosis of myocardial abnormality in patients with CD despite a preserved global function. We also showed that as left ventricular diastolic parameters, E‘ml, E‘ms, E‘ml/A‘ml and E‘ms/A‘ms in patients with CD were found significantly lower than the control group, but RT‘ml, RT‘ms values and A‘ml, A‘ms, E/E‘m ratio were similar in both groups. This condition may be related with the long period is necessary for diastolic dysfunction to occur and the different parameters is affected in different stages of the disease. In addition, when systolic functions were assessed with TDI, IVA and PCTm/CTm ratios were found to be lower in the patient group than in the control group. However,Sm velocity was found similar in both groups’ lateral and septal walls. Sm wave is an index of the ejection phase, which is used to determine left ventricular functions. Sm wave is preload/ afterload dependent. On the other hand, IVA is a load independent parameter, which is said to be more sensitive than Sm wave in measuring LV contractility (22-24). In our study, IVA in patients with CD was clearly lower than the control group, and a positive correlation was determined between IVA and Sm velocity.
The present study is the first study evaluating left ventricular functions in patients with active CD by TDI, in literature. Our study confirms that patients with CD have impaired diastolic function. More important, we also showed that an impairment of myocardial systolic function in patients with CD by TDI. We recommend using TDI method especially IVA parameter, in addition to conventional echocardiography parameters for the cardiovascular risk assessment of patients with Cushing’ syndrome. Our study was designed prospectively, and based on presented sectional data. TDI findings are being monitored according to the response of our patient group to the treatment.
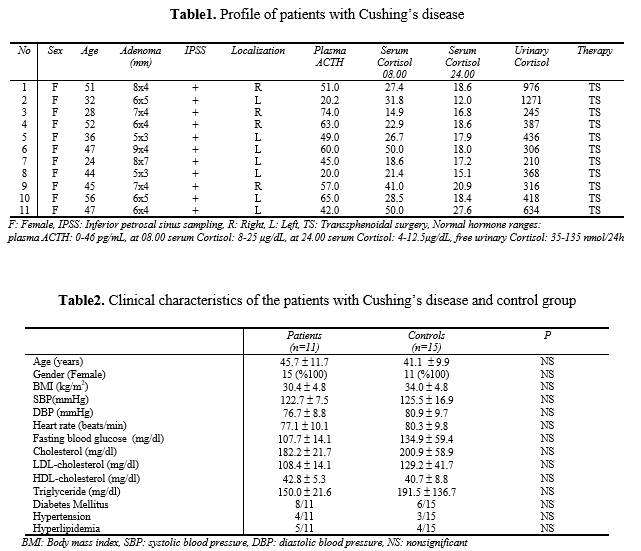
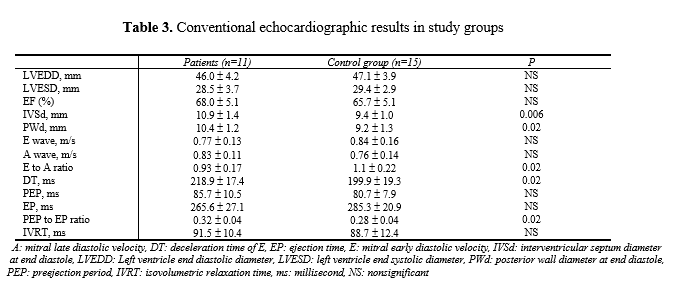
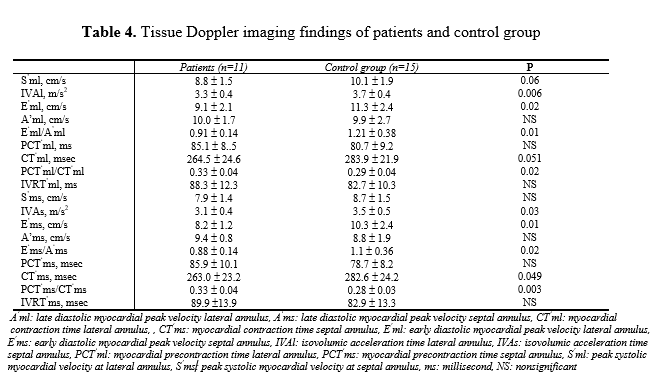
Figure 1.Peak systolic myocardial velocities at lateral annulus (S’ml) have positive correlation with isovolumic acceleration time at lateral annulus (IVAl)
Figure 2.Peak systolic myocardial velocities at septal annulus (S’ms) have positive correlation with isovolumic acceleration time at septal annulus (IVAs)
27 - Case report: subcapsular hematoma complication during percutaneous laser ablation(PLA) to a hypoactive benign solitary thyroid nodule, and literature review of PLA- related complications - 2008
Uluslararası Bildiriler 10th European Congress of Endocrinology, Berlin, Germany, 3-7 May, Endocrine Abstract Vol:16, P767, 2008
26 - Case report: percutaneous laser ablation(PLA) to a functional eutyroid autonomous thyroid nodule, and histopathologic effects of PLA on nodule after thyroidectomy at 2nd year of procedure - 2008
Uluslararası Bildiriler 10th European Congress of Endocrinology, Berlin, Germany, 3-7 May, Endocrine Abstract Vol:16, P763, 2008
25 - Panhypopituitarism after trumatic brain injury and its possible relation with insulin resistance - 2008
Uluslararası Bildiriler 13th Meeting of the European Neuroendocrine Association, Antalya, Turkey, 17-20 October, Abstract Book: PS.88, 2008
ABSTRACT
Pituitary dysfunction due to traumatic brain injury (TBI) may be partial or complete and in retrospective studies as many as 25-50% of patients have been demonstrated to have some degree of pituitary hormone deficiency. Hyperglycemia is associated with poor neuro- endocrinological outcome after TBI. Our aim in presenting this case is to scrutinize the relationship between insulin resistance and panhypopituitarism, but also call attention over the feasibility of different ways of conventional methods for reducing this resistance.
CASE: A 55 years old male was presented in emergency service with traffic accident. He had any known medical history. At the first physical examination it was noticed that he had no spontaneous respiration, but also had multiple fractures and severe cranial injury. His Glasgow coma scale score was 5. In the cranial tomography images cerebral tissues couldn’t have been detected because of general cerebral oedema. Fractures were established at the right orbital structures and temporal bones. Also it was seen that he had bilateral hematothorax, liver and splenic lacerations confirmed by tomographic images. The other fractures existed allover his body were localized at right humerus and ulna, left radius and ulna, right femur and tibia. The patient, consulted to our department for ketonuria and glucosuria observed in urine analysis, was then taken under prosecution in reanimation unit after undergoing tracheostomy and gastrostomy procedures for he was at risk of cerebral herniation. 1 U/h of insulin infusion was initiated for blood glucose regulation. He underwent one session of all operations required for fracture stabilization by orthopedy department at posttraumatic second day. After the fifth day, despite insulin doses were redounded, blood glucose levels progressed high. By the evaluation of hypophyseal and target hormones, he was diagnosed as posttraumatic panhypopituitarism; thereafter glucocorticoid and L-thyroxine replacements were initiated. Laboratory tests of patient showed in table.
Table. Laboratory tests of patient
A.G | ||
Age | 55 | |
Glasgow Coma Scale Score | 5 | |
Hormonal, Biochemical and Hematological Status | ||
GH (0-10 ng/mL) | 0.01 | |
TSH (0.4-4.0 uIU/mL ) | 0.13 | |
LH (1.1-14.7 mIU/mL ) | 0.62 | |
FSH (2.8-11.3 mIU/mL) | 0.33 | |
PRL (19.5-25 ng/mL) | 1.91 | |
FT4 (0.85-1.78 ng/dL) | 1.31 | |
Cortisol (8-25 μg/dL) | 4.87 | |
Free Testosterone | 5.15 | |
Glucose (70- 100 mg/dl) | 330 | |
Na (135-140 mEq/l) | 158 | |
K (3.5-4.5 mEq/l) | 5 | |
BUN (mg/dL) | 110 | |
Cre(mg/dL) | 1.8 | |
ALT (IU/L) | 85 | |
AST (IU/L) | 125 | |
WBC | 25.000 | |
Haemoglobin | 11 | |
Haematocrit (%) | 30 | |
PLT | 120 |
In order to obtain normoglisemic status, 40 U/h of insulin infusion (960U/d) was applied to patient having total parenteral nutrition. With aim to reduce insulin resistance, squeezed 8 mg rosiglitasone in 50 cc SF was given during 24 hours by gastrostomy. Under this treatment, his needs for insulin regressed to 6-8 U/h at the end of three days. During the follow up, his conscious status vanished, tracheostomy and gastrostomy was closed, and he started to take nourishment orally. Having any history of diabetes before the accident, patients’ blood glucose levels were stabilized by 28 U/d Novomix 30® applications. At posttraumatic 12th month, hypophyseal and target hormone levels were reevaluated and is was decided that he has permanent panhypopituitarism. Our patient is still under glucocorticoid, L-thyroxine, testosterone and recombinant growth hormone replacement therapy.
CONCLUSION: In recent reports showed that both of the blood glucose and insulin concentration increases markedly following severe TBI. In spite of elevated insulin levels, insulin resistance at the receptor and postreceptor levels may contribute to hyperglycemia, even in non-diabetic persons like our patient, particularly when stress hormones that promote glycogenolysis are released, including catecholamines and cortisol. Normoglycaemia with intensive insulin treatment in critically ill patients decreases morbidity and mortality. In resistant cases like our patient, PPAR γ agonists may be helpful maintaining normoglycaemia.
24 - Case report: a case of diffuse large B-cell lymphoma presented by instantaneous enlargement in a known thyroid nodule and diagnosed by fine needle aspiration biopsy - 2008
Uluslararası Bildiriler 10th European Congress of Endocrinology, Berlin, Germany, 3-7 May, Endocrine Abstract Vol:16, P762, 2008
ABSTRACT
Primary thyroid lymphoma is an uncommon malignancy; it accounts for < 2% of all extranodal lymphomas and < 5% of all thyroid malignancies. Differentiation of thyroid lymphoma from anaplastic carcinoma by cytomorphological analysis is difficult. However, thyroid lymphoma can be diagnosed up to 80% by immunohistochemical analysis.
CASE: A 52 year old male patient who was known to have a nodule in his thyroid gland for many years presented with instantaneous enlargement of his existing nodule and with appearance of ipsilateral cervical lymphadenopathy. The patient had complaints of shortness of breath and difficulty in swallowing. On thyroid ultasonography, a giant nodule of 38.4x31.6x45.5 mm size and 28.9 ml volume, containing macro and microcalcifical areas was detected in the left lobe. In the ipsilateral anterior cervical region, a lymphadenopathy with ultrasonographically malign appearance, in size of 23.4x15.6x32 mm was observed. The nodule defined in the left lobe was hypoactive in thyroid scintigraphy. The patient was euthyroid in laboratory findings and his thyroglobulin and calcitonin values were in normal ranges. As cytomorphological appearance was consistent with anaplastic carcinoma in ultrasonography-guided aspiration biopsies of thyroid nodule and lymphadenopathy, immunohistochemical staining was performed for differential diagnosis of lymphoma. Diffuse large B-cell lymphoma cells showing CD20 involvement were seen in cytological specimens (Figure 1).
Figure 1.Diffuse large B-cell lymphoma cells showing CD20 involvement
.png)
Because the patient’s ventilation distress was severe and the density of his thyroid nodule was very hard, total thyroidectomy was urgently planned in order to relieve the pressure symptom. The histological specimens of the patient who underwent total thyroidectomy and cervical neck dissection were examined. While normal thyrocytes were detected in thyroid gland, atypical lymphoid cells showing diffuse infiltration in thyroid tissue were observed in the nodule, which were stained diffuse, strongly positive for CD20 and BcL and negative for cd45 RO. In the lymph node, diffusely infiltrating atypical lymphoid cells with similar immunohistochemical staining properties were observed. According to Revised European-American Classification of Lymphoid Neoplasms, the diagnosis was diffuse large B-cell lymphoma. The patient was accepted as stage I-EB. Rituximab, Doxorubucin, cyclophosphamide, vinciristine, and prednisone chemotherapy was started. The patient still remains asymptomatic with 150 mcg L-Thyroxine and no further recurrence or metastasis has been noted in the postoperative course of eight months. We introduce the case in order to emphasize that infiltration of diffuse large B-cell lymphoma should be recalled with instantaneous enlargement of nodules known to be benign previously, and when cytological specimen is uncertain, immunohistochemical staining should be performed for differential diagnosis.
23 - Clinical and ultrasonographic dilemma: Are what we palpate on thyroid examination and what we see on ultrasonography the same? - 2007
Uluslararası Bildiriler 32 th Annual Meeting of the European Thyroid Association, Leipzig, Germany, September 1-5, 2007. Horm Res 2007; 68(suppl 3): 86
ABSTRACT
INTRODUCTION: Clinical examination is the primary diagnostic test used to determine the thyroid pathologies. Although its employability in the purpose of screening to demonstrate the degree of iodine deficiency in the areas of endemic goiter where our country is included, the sensitivity of palpation in assessing the size of thyroid and detecting thyroid nodules is reported to be low. After clinical examination, thyroid ultrasonography is utilized as the basic imaging method in the evaluation of patients. According to AACM/AME guideline, routine ultrasonographic evaluation of patients, assessed normally by thyroid examination with thyroid function tests in normal ranges, those describe no symptoms such as hoarseness, dyspnea, dysphagia, and those in low risk group for thyroid cancer, is not recommended. This superiority of palpation known as a method of low sensitivity in detecting thyroid nodules to ultrasonography is controversial. Because nonpalpable nodules were reported to have similar malignancy risk compared to palpable nodules.In this study we aimed to compare findings of thyroid examination with findings of ultrasonography in patient attended to our thyroid outpatient clinic and to determine the limits of examination and ultrasonography in general practice.
MATERIAL AND METHOD:
Patients
We evaluated 6835 patients aged over 15 who attended to the thyroid outpatient clinic of our center between January 2006-December 2006, whose thyroid ultrasonographies were requested after their first examination and thyroid function tests. Considering that it would affect the palpation findings, patients who previously underwent an operation to neck region, pregnant women, and who received drugs affecting thyroid functions were excluded. We included 1157 patients who previously had no history of any known thyroid disease, who attended with symptoms such as swelling in the neck, pain feeling of tickle in the throat, palpitation, sweating, hoarseness, tremor, nervousness, fatigue, weight gain or weight loss, and/or those who were detected to have impairment in thyroid function tests.
Clinical examination of thyroid gland
Thyroid examinations of the patients were performed on the same day by two experienced clinicians (R.E and O.T), who were blind to findings of each other. On the examination, the thyroid gland was evaluated by inspection and palpation. Findings were classified according to World Health Organization (WHO) criteria. Nodules detected in examination were recorded for their sizes. Nodule sizes were categorized as <1 cm, 1- 2 cm, 2- 3 cm, >3 cm.
Ultrasonography of thyroid
Thyroid ultrasonography was performed on the same day using the same device (Esaote Technos- MPX, Geneva, Italy) with a multi- frequency probe by two experts (B.C and M.G) experienced on thyroid ultrasonography who were blind to findings of each other. Thyroid gland was examined in three dimensions. Thyroid volume for each lobe was calculated using the ellipsoid formula.Thyroid parenchyma was assessed as homogeneous or heterogeneous in various degrees (mild, moderate, and severe). Numbers and localizations of nodules detected on ultrasonography were measured and recorded. The nodules were categorized as <1 cm, 1- 2 cm, 2- 3 cm, >3 cm. Clinical diagnoses were determined by another clinician (K.G) in the light of thyroid function tests and the thyroid ultrasonography data of the patients.
Statistics
For the statistical analysis of the study, SPSS 11.5 packet program (SPSS Inc., Chicago, IL) was used. Results with p<0.05 were accepted as statistically significant.
RESULTS: Of 1157 patients included in the study, 987 (85.3%) were women and 170 (14.7%) were men, and mean age was 41.16 ±14.13 years (16-80 years). Clinicians who examined thyroid (P1, P2) primarily classified thyroid glands in their sizes according to WHO criteria. Findings of the observers in regard to this classification and the comparative data are shown in Table 1. As to this assessment, no significant difference was determined between the findings of the observers who performed palpation (p=0.461). When inter-observer consistency was evaluated, Kappa value was determined as k= 0.82 (82%), and this consistency was found statistically significant (p<0.001).
Table 1.Findings of the observers (P1 and P2) in regard to WHO classification and the comparative data
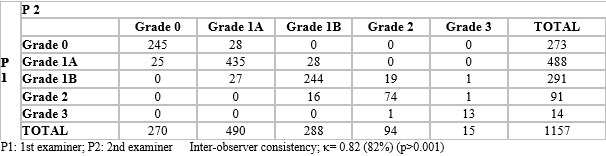
Using WHO classification is recommended to detect thyroid size in areas with endemic iodine deficiency. When the clinical examination and ultrasonographic findings were compared for thyroid sizes, palpation and ultrasonography findings were 86-92.5 % correlated in the assessment of thyroid size. If no nodule was detected in clinical examination of thyroid gland, this result is 76.7-77.4 % correct. Sensitivity of palpation in detecting the absence of nodule is 87.3-89 % (Table 2). Compared to ultrasonography, sensitivity of palpation in detecting thyroid nodules is 56.1-56.7 % (Table 2). If a single nodule is detected by palpation, there are 44.3-50.4 % accompanying one or more nodules (Table 2). Different from other studies, an important result we determined was that the rate of detecting one or more nodules by palpation, even though there was no nodule on ultrasonography, was 11-12.7 %, and that 87.4-91.2 % of these clinically diagnosed cases had thyroiditis confirmed by laboratory. As conclusion, palpation is not only ineffective in diagnosing parenchyma disease, but also may misguide the clinician. Table 3 shows kvalues indicating variation of detecting nodules between the findings of observers, who performed examination and ultrasonographic evaluation. The consistency of detecting thyroid nodules between observers who performed palpation and the ultrasonography was 30-38 %.
Table 2. Thyroid nodularity assessed clinically vs ultrasonically
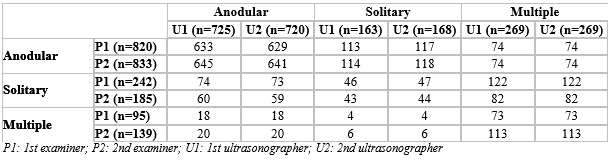
Table 3. The consistency of detecting thyroid nodules between observers who performed palpation and the ultrasonography
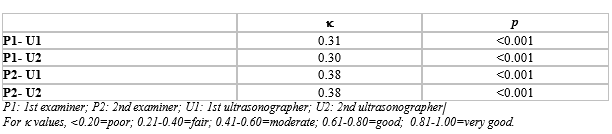
CONCLUSION: We think that high sensitivity of ultrasonography should always be preferred in spite of the experience of the clinician who perform palpation. Although evaluated normally, all thyroid examinations should certainly be completed by thyroid ultrasonography.
22 - Case report: Ultrasound-guided percutaneous laser ablation treatment in inoperabl aggressive course anaplastic thyroid carcinoma: The introduction of a novel alternative palliative therapy-second experience in the literature - 2007
Uluslararası Bildiriler 32 th Annual Meeting of the European Thyroid Association, Leipzig, Germany, September 1-5, 2007. Horm Res ; 68(suppl 3): 40, 2007
21 - The relationship between diurnal variation of TSH and thyroid blood flow with Doppler ultrasonography in healthy adults - 2007
Uluslararası Bildiriler 32 th Annual Meeting of the European Thyroid Association, Leipzig, Germany, September 1-5, 2007. Horm Res 2007; 68(suppl 3): 56
ABSTRACT
INTRODUCTION: Thyroid stimulating hormone (TSH) shows pulsatile and circadian variation. In normal adult men and women, TSH levels are low throughout the daytime and begin to increase in the late afternoon or early evening. Maximal TSH levels occur shortly before sleep. During sleep, TSH levels generally decline slowly. A further decrease occurs in the morning hours. Thyroid gland is highly vascular, and TSH is known to alter the blood flow of the thyroid. It has been reported that measurement of blood flow at the inferior thyroid artery (ITA), a major feeding artery in the thyroid, is a useful method of differentiating between various thyroid diseases. However, there is no detailed study in the literature on the associations between the Doppler parameters of thyroid blood flow and diurnal rhythm of TSH. The aim of present study was to determine the presence of a correlation between the Doppler parameters of thyroid blood flow and TSH levels in the morning, late afternoon and at midnight in healthy adults.
SUBJECTS AND METHODS: We prospectively examined 30 non- smoker healthy adults (15 men (50%) and 15 women (50%), 24- 54 years old). The sex, age, body weight, height and body mass index (BMI) were determined. Blood samples were taken from individuals at 08.00 for measuring thyroid hormones [free triiodothyronin (FT3) and free thyroxine (FT4)], thyroid antibodies [anti thyroid peroxidase antibody (anti-TPO) and anti thyroglobulin antibody (anti-Tg)]and TSH levels. Thyroid hormones and TSH levels also were measured at 16.00 and 24.00. Subjects were required to collect 24-hour urine samples after discarding first urine sample in the morning. Daily iodine excretion was calculated from urine samples. Normal values in our laboratory are as follows: FT4, 0.61- 1.12 ng/dL; FT3, 1.57- 4,71 pg/mL; TSH, 0.4- 4.0 uIU/mL; anti-Tg <30 U/mL; anti-TPO <10 U/mL and Urine iodine 10- 20 mg/dL.
Conventional and Power Doppler Ultrasonography
Thyroid ultrasonography and Doppler ultrasonography was performed at 08.00, 16.00 and 24.00. In each individual, a preliminary ultrasonography examination was performed to identify any abnormalities such as parenchymal heterogeneity or nodule. All participants were examined after a 10- min rest period to minimize the changes in blood pressure and heart rate to avoid influencing the Doppler parameters. All Doppler and gray-scale measurements were performed by the same experienced radiologist (M.G) using the same Doppler ultrasonography device (LogicO9 Doppler System, General Electric Medical Systems, Milwaukee, WI, USA) with a 10 MHz broadband linear transducer in thyroid mode. Thyroid gland was scanned in three dimensions. Thickness, width (in transverse plan), and length (in longitudinal plan) of each lobe were measured by longitudinal and transverse scans. Volume for each lobe was calculated using the ellipsoid formula. After the gray- scale ultrasonography examination, each individual underwent Doppler ultrasonography examination. Thyroid blood flow measured at the ITA, because of its major contribution to thyroid blood flow, ease of identification, and low coefficient of variation of less than 5.2%. The color gain was adjusted so that artifacts were prevented. The angle was kept between 45°and 60°, and the angle correction cursor was parallel to the direction of flow. The velocity waveform was displayedabove the baseline to indicate the arterial blood flow, and the peak systolic velocity (PSV) and resistance index (RI) were obtained from both ITAs, and the mean values were recorded (Figure 1).
Statistical analysis
For the statistical analysis of the study, SPSS 11.5 packet program (SPSS Inc., Chicago, IL) was used. Values of P< 0.05 were accepted as statistically significant.
Figure 1. The velocity waveform is displayed above the baseline to indicate the arterial blood flow. The figure shows the measurement of the blood flow velocity in the inferior thyroid artery (left).
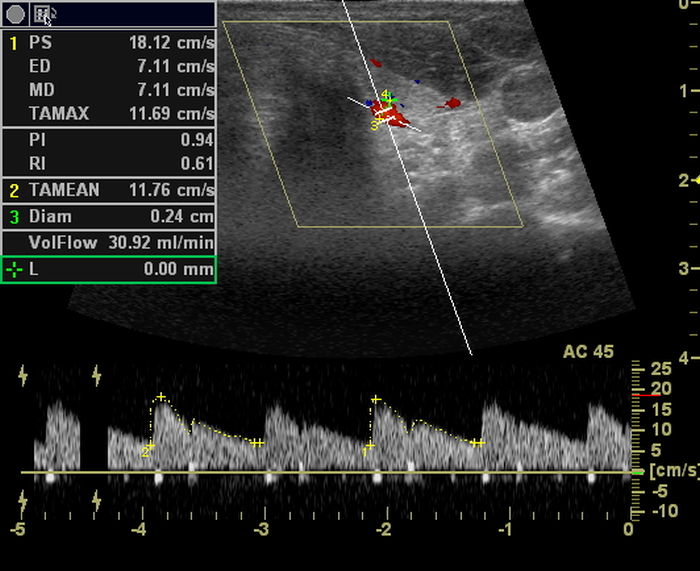 |
RESULTS: Thirty individual were included in the study between 24 and 54 years of age. There were 15 female (50%) and 15 male (50%) patients with a mean age of 32.20 ±7.39 years. Mean BMI 24.70 ±3.80 kg/m2, and the mean urinary iodide excretion 14.07 ±2.53 mg/dL were. Demographic and laboratory data of study group with comparative results according to sex were listed in Table I. No statistically significant difference was detected between groups according to age, BMI, thyroid function tests, and urinary iodine excretion (p>0.05).
Data of mean age, body mass index, FT3, FT4 and TSH levels, thyroid volumes, peak systolic velocity and resistance index at 08.00, 16.00 and 24.00 were showed in Table II. Diurnal serum TSH concentrations were evaluated and significant difference between morning, afternoon, and night TSH levels was detected. TSH levels measured at 24.00 were significantly high compared to those at 08.00 and 16.00 (p<0.001 and p<0.001, respectively). TSH levels measured at 16.00 were also significantly higher than those at 08.00 (p<0.001).
Diurnal thyroid volume changes were evaluated. There was no meaningful difference between thyroid volumes calculated from morning and afternoon measurements (p=807). However, thyroid volumes at night were significantly higher compared to morning and afternoon levels (p<0.001).
Mean PSV levels were evaluated and an increase during daytime was observed. However, no statistically significant difference was present between PSV values measured at 08.00 and 16.00 (p=0.113). PSV values measured at 24.00 were significantly high compared to morning and afternoon measurements (p<0.01, and p<0.05, respectively). In contrast to PSV, RI values tended to decrease during daytime. RI values measured at night were significantly low compared to morning and afternoon values (p<0.001). The difference between morning and afternoon RI levels were also statistically significant.
CONCLUSION: Unique feature of our study is that it is the first study showing thyroid blood flow variations by quantitative Doppler parameters in relation to diurnal changes of TSH levels. In this study, we investigated the correlation between ITA blood flow parameters and thyroid volume, thyroid hormones, and TSH in three different times of day. We observed that PSV increased and RI decreased in night times when TSH peaked, which means increased thyroid blood flow. Again, we observed an increase in thyroid volume at night compared to daytime. Our study constitutes the beginning of the hypothesis that blood flow pattern in thyroid gland pathologies may show diurnal variation as in healthy individuals. For this reason, we think that thyroid blood flow should be evaluated diurnally by power Doppler in TSH dependent thyroid pathologies, autoimmune diseases affecting TSH receptor, or thyroid nodules considered to develop independently from TSH.
Table I. Demographic and laboratory data of study group with comparative results according to sex
Male N=15 | Female N=15 | P | |
Age (year) | 33 ±8.5 | 31.3 ±6.0 | >0.05 |
BMI (kg/m2) | 25.5 ±3.0 | 23.8 ±4.4 | >0.05 |
Urine iodine (mg/dL) | 16.36 ±3.01 | 15.04 ±2.74 | >0.05 |
FT3 | 3.24 ±0.26 | 3.05 ±0.85 | >0.05 |
FT4 | 0.81 ±0.07 | 0.79 ±0.05 | >0.05 |
TSH | 1.18 ±0.64 | 1.32 ±0.69 | >0.05 |
Anti TPO (U/mL) | <10 | <10 | - |
Anti Tg (U/mL) | <30 | <30 | - |
Table II. Data of FT3, FT4 and TSH levels, thyroid volumes, peak systolic velocity and resistance index at 08.00, 16.00 and 24.00
08.00 | 16.00 | 24.00 | |
FT3 (pg/mL) | 3.11 ±0.59 | 3.00 ±0.43 | 3.33 ±0.63 |
FT4 (ng/dL) | 0.77 ±0.09 | 0.83 ±0.08 | 0.86 ±0.09 |
TSH (uIU/mL) | 1.29 ±0.55 | 1.88 ±1.08 | 3.09 ±1.52 |
Thyroid volume (mL) | 10.46 ±3.71 | 10.43 ±3.75 | 12.02 ±5.03 |
PSV (cm/s) | 24.90 ±8.51 | 25.88 ±9.82 | 27.75 ±9.54 |
RI | 0.57 ±0.07 | 0.56 ±0.05 | 0.53 ±0.07 |
20 - Metastatic breast cancer presenting with panhypopituitarism: A case report - 2006
Uluslararası Bildiriler 12th Meeting of the European NeuroEndocrine Association, Hormones Vol. 5 (Suppl, 1), P151, 104. Athens, Greece, October 21-24, 2006
ABSTRACT INTRODUCTION: Secondary neoplasm of the pituitary most often are found incidentally at autopsy and are not associated with clinical symptoms or biochemical abnormalities. On large autopsy series the incidence of metastases to the pituitary gland is between 1% and 3.6% in patients with malignant tumors. Breast carcinoma is the most common primary lesion that metastasis to the pituitary gland; its frequency is followed by that of lung cancer. Pituitary metastases have been reported to occur in approximately 6% to 29% of patients with breast carcinoma. In pituitary metastases, the most commonly observed endocrine abnormality is diabetes insipidus. The presentation with a hypofunction of the anterior and posterior lobe of the pituitary gland is a rare condition. We report on a patient with panhypopituitarism and diabetes insipidus centralis that developed due to a metastasis of a breast carcinoma in the pituitary gland. CASE REPORT: The patient, a 55-year-old woman was admitted to endocrinology clinic with a history of polydipsia, approximately 20 liters per day, polyuria, malaise, weight loss and vision loss. Her past medical history was significant for stage III estrogen receptor positive infiltrating ductal carcinoma of the left breast treated with modified radical mastectomy and following the operation application of radiotherapy and adjuvant chemotherapy with cyclophosphamide, 5-fluorouracil, and methotrexate. In follow- up period a mass occupying the right breast had been determined. She had been under anastrozole during 4 years after radiotherapy and protective surgery of right breast. Physical examination was remarkable for a blood pressure of 90/50 mmHg and scarce axillary and pubic hair. Laboratory investigations revealed hypofunction of the anterior lobe of the pituitary gland and diabetes insipidus centralis. The response of fluid deprivation test and administration of exogenous vasopressin confirmed diabetes insipidus centralis. GHRH, LHRH, TRH and CRH tests showed no response. The patient had been diagnosed with panhypopituitarism and diabetes insipidus, and has been under treatment with hydrocortisone (30 mg /day), thyroxin (50 mg/day) and intranasally desmopressin 20 μg/day. MRI demonstrated an intrasellar mass 28x18x10 mm in diameter occupying suprasellar region and also compressing the optic chiasm (Figure 1). In ophthalmologic examination bitemporal hemianopsia was demonstrated. The mass appeared hyperintense on the T1- weighted images and overall hypointense with hyperintense areas on the T2- weight images. PET with 18F- FDG was applied to the patient. It revealed pathologically increased 18F- FDG encampment in the mass occupying suprasellar region, right breast and right axilla (Figure 2, 3). The patient underwent partial hypophysectomy by transcranial route. Final pathology confirmed metastatic breast carcinoma (Figure 4). For pituitary metastasis control, she underwent gamma knife surgery in doses of 16 Gy. In early period following radio- surgery, tumor shrinkage was achieved. But in the sixth month progression of the disease was observed. Although hormone replacement therapy was given, the patient’s general status couldn’t be stabilized for chemotherapy. She deteriorated gradually and died approximately 12 months after the demonstration of hypophyseal tumor. DISCUSSION: When literature is reviewed, it appears that posterior pituitary metastasis was seen more frequently than anterior pituitary, with an incidence of 69% and 79% of cases, respectively in two series, presumably because the posterior lobe has a rich direct arterial blood supply as to the anterior lobe. Metastatic tumor deposits usually occur first in the pituitary stalk or posterior lobe and permeate the anterior lobe, either by direct extension from the pituitary stalk or posterior lobe, or through the portal circulation by portal vessels. However, isolated metastases may occur in the anterior lobe. Max et al. reported that 79% of patients had involvement of the posterior lobe alone or in combination with anterior lobe involvement, and 21% of patients had solitary anterior lobe disease, in a series of 178 cases. Pituitary metastases are usually asymptomatic, with only 7% reported to be symptomatic. Symptoms of diabetes insipidus frequently occur with pituitary metastases. Visual field defects, headache, compressive optic neuropathy and anterior pituitary dysfunction are the most commonly reported symptoms. Differentiation of pituitary metastases from other pituitary tumors based on neuroimaging alone can be difficult, although certain features, such as thickening of the pituitary stalk, invasion of the cavernous sinus, and sclerosis of the surrounding sella turcica, can indicate metastasis to the pituitary gland. CT and MRI are used as imaging techniques. Mayr et al. reported that MRI findings of pituitary involvement are more useful than CT findings to differentiate between benign adenomas and malignant processes. It is obvious that these imaging techniques are not enough in differential diagnosis of disease if they are not supported by the biopsies. As a radionuclide imaging techniques, 18F-FDG- PET is an established method in the detection of primary tumor or metastases of various cancer types. The accumulation of 18F-FDG in malignant tissue is well known; it is influenced by the grade of malignancy, related to glycolysis. 18F-FDG- PET is a sensitive (69%) and specific (80%) method in following treated breast cancer patients, as previous study has suggested. Also, we have not met any submitted case report or study emphasizing sensitivity or specificity of this technique in pituitary metastasis imaging in the literature. Treatment for pituitary metastases is often multidisciplinary and includes surgery, radiotherapy and chemotherapy. Surgical series have not shown any significant survival benefit between patients who underwent surgery and who did not. However, large randomized studies evaluating the treatment of pituitary metastases have not been performed yet. The prognosis of pituitary metastases is poor, and mean length of survival is reported to range between 6 and 22 months, independent of the treatment strategy. We have reported a patient with symptomatic anterior and posterior pituitary involvement from metastatic breast carcinoma. Metastatic disease of the pituitary was confirmed with MRI, PET/CT imaging with 18F- FDG and hypophyseal biopsy. This case illustrates that pituitary metastases are an uncommon but important cause of panhypopituitarism and diabetes insipidus, and may be the initial sign of widely metastatic cancer, and we suggest that 18F-FDG- PET is a useful method for the detection of pituitary metastases and pituitary malignant tumor. Figure 1. Intrasellar mass occupying suprasellar region Figure 2. 18F- FDG encampment in the mass occupying suprasellar region Figure 3. 18F- FDG encampment in the mass occupying suprasellar region Figure 4. Immunohistochemical profile of the pituitary
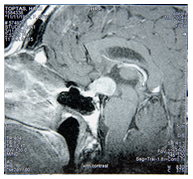
Figure 1. Intrasellar mass occupying suprasellar region
Figure 2. 18F- FDG encampment in the mass occupying suprasellar region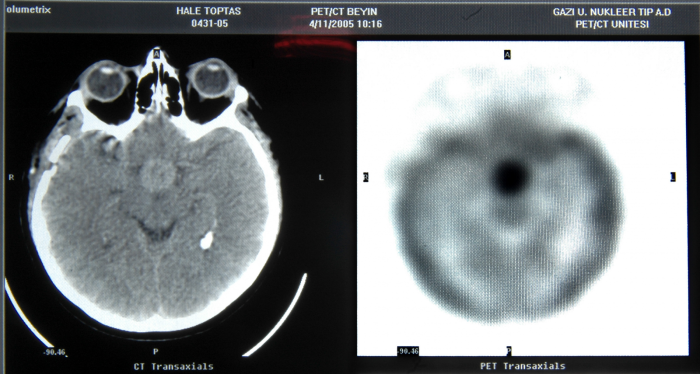
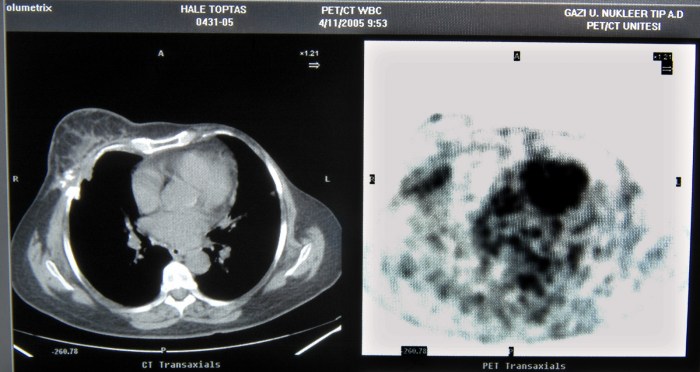
Figure 3. 18F- FDG encampment in the mass occupying suprasellar region
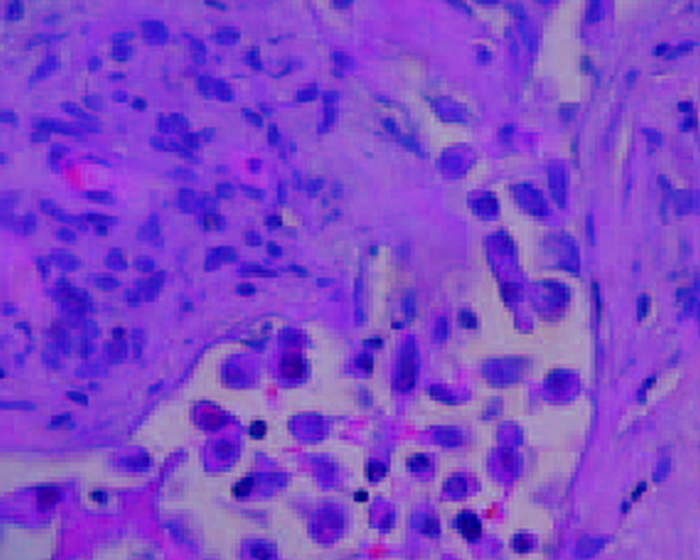
Figure 4. Immunohistochemical profile of the pituitary
19 - A macroprolactinoma and growth hormone deficiency in an adolescent patient: Clinical presentation, treatment and follow-up - 2006
Uluslararası Bildiriler 12th Meeting of the European NeuroEndocrine Association, Hormones Vol. 5 (Suppl, 1), P139, 101. Athens, Greece, October 21-24, 2006
ABSTRACT
INTRODUCTION: Pituitary adenomas constitute between 1.1 and 6% of all intracranial tumors in pediatric and adolescent age. Prolactin (PRL) secreting pituitary adenomas rarely occurs in this age group, with various incidences reported to range from 0.6 to 6.2% of pituitary adenomas in all age groups, and from 19.7 to 72.2% of pituitary adenomas in pediatric/ adolescent patients. PRL secreting pituitary adenomas frequently are macroadenomas in the prepubertal and postpubertal ages. Their mass effect frequently cause delayed puberty and growth hormone deficiency (GHD). We report a male adolescent patient with macroprolactinoma and GHD was treated by cabergoline and recombinant human GH (rhGH).
CASE REPORT: A macroprolactinoma with isolated Growth Hormone Deficiency (lack of Growth Hormone response to stimuli after testosterone priming) and symptomatic chiasmal compression was diagnosed in a 15 year- old boy. Height: 141,5 cm, Bone age: 12 years 6 months, Height SDS: -5.079 and Pubertal stage: P 1 were. Magnetic resonance imaging demonstrated a mass 25x25x18 in diameter occupying suprasellar region and also compressing optic chiasm. Bromocriptine 10 mg per day was used for 3 months without any response in terms of PRL level (>150 ng/ mL) or tumor shrinkage, so cabergoline was initiated in an incremental regimen up to a maintenance dose of 2 mg per week. After 9 months of cabergoline treatment PRL levels decreased in normal range and major tumor shrinkage was observed. After 20 months of cabergoline treatment there was only a 3x2 mm thick tumor remnant in the sellar floor was observed. The patient was asymptomatic, visual field was normal, insulin tolerance test and L-DOPA test were repeated and Growth Hormone treatment 0.2 mg/ kg/ weekly was added to the therapy. GH therapy improved the growth rate, and no expansion of the macroadenoma was observed during the combined treatment.
COMMENT: Prolactinomas are rare in children and adolescent, and GHD is a common finding in young patients with macroprolactinoma. However, normalization of GH secretion after therapy has also been reported. Treatment with dopamine agonists (bromocriptine and cabergoline) is effective in normalizing PRL levels and in shrinking tumor mass in the majority of adult patients with prolactinoma. In children and adolescents, dopamine agonists, especially cabergoline, have been used successfully be several investigators, such as our patient. In addition, the combined treatment with cabergoline and rhGH seems to be safe and highly effective in patients with GHD. Nevertheless, careful monitoring and on-going evaluation are necessary.
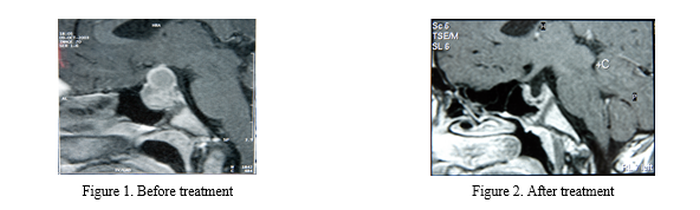
18 - Craniocerebral imaging in adolescents with growth hormone deficiency and short stature:A descriptive study - 2006
Uluslararası Bildiriler 12th Meeting of the European NeuroEndocrine Association, Hormones Vol. 5 (Suppl, 1), P52, 76. Athens, Greece, October 21-24, 2006
ABSTRACT
INTRODUCTION: Growth Hormone Deficiency (GHD) is an important cause of growth retardation and short stature. The rate of occurrence has been reported in the literature between 1/3480 and 1/30.000. GHD may be idiopathic or associated with organic causes, such as tumor, surgery, trauma or irradiation of the sellar area, and it may be with or without multipl pituitary hormone deficiency. The anterior pituitary and stalk are well defined, and the posterior pituitary is easily identifiable as a hyperintense bright spot on imaging studies. Magnetic Resonance Imaging (MRI) can show characteristic anatomic pituitary abnormalities in patients with GHD, including a small to absent anterior pituitary gland, a small or truncated stalk, and an ectopic posterior pituitary hyperintensity located at the base of the hypothalamus or at the inferior end of the truncated pituitary stalk. In the present report we aimed to analyze the type and frequency of cranial MRI anomalies in patients with GHD, and also to investigate the relationship between craniocerebral images and the presence of isolated GH or multiple pituitary hormone deficiency.
PATIENTS AND METHODS: We evaluated 35 patients who were subsequently diagnosed to have GHD in the endocrinology department of our hospital between October 2002 and June 2006 retrospectively. The diagnosis of GHD was based on auxological and biological criteria; exclusion of other diseases, and a GH peak level of <10 μg/dl in at least two stimulation tests, usually the insulin tolerance test and L-DOPA test done by standard methods. Sex steroid priming was applied for boys and girls if they had pubertal development < genital stage 2 or breast stage < 2, independently of bone age. Hypothyroidism was defined as low or low- normal serum TSH concentration and free T3 concentrations. Plasma ACTH and serum cortisol values were measured in the morning. ACTH deficiency was defined as either a morning serum cortisol concentration of less than 3.6 μg/dl or an impaired cortisol serum concentration rise inferior to 20 μg/dl during insulin- induced hypoglycemia. Hypogonadism was confirmed in both sexes by lack of puberty and no increase in FSH and LH in response to gonadotropin releasing hormone. Cranial imaging studies, with special emphasis on the hypothalamo- pituitary region, were performed in all patients using MRI and were all assessed by the same radiologist. Size of pituitary fossa, pituitary gland, localization of the pituitary gland, homogeneity, enhancement and changes of parasellar structures were evaluated.
RESULTS: Thirty- five adolescents with a mean age of 18.04 ± 3.02 Years (14,5- 23), 22 boys and 13 girls were evaluated. All patients had severe GHD. After studying the pituitary function and determination of karyotype in the girls, the patient classified in to four groups: Isolated GHD (n= 10), Multiple pituitary hormone deficiency (MPHD) (n=23), neurosecretory dysfunction (NSD) (n= 1) and Turner Syndrome (n= 1). Of the 35 patients studied the MRI was abnormal in 30 (85.7 %). In MRI evaluation, 10 (28.6 %) of 35 patients had Empty Sella, 10 (28.6 %) had Partial Empty Sella, 6 (17.1 %) had tumor involving the hypothalamic- pituitary axis, 3 (8.6 %) had Partial Empty Sella, hypoplastic pituitary and ectopic neurohypophysis, and 1 (2.85 %) had small sella and hypoplastic pituitary. 5 of 6 patients with tumor had craniopharyngioma and other one had macroprolactinoma. MRI findings and hormonal status of our patients are presented in a Table 1.
Table 1.MRI findings and hormonal status: ES (Empty Sella), PES (Partial Empty Sella), EN (Ectopic Neurohypophysis), HH (Hipoplazik Hipofiz), SS (Small Sella), IGHD (Isolated pituitary hormone deficiency), MPHD (Multiple pituitary hormone deficiency), NSD (Neurosecretory Dysfunction)
ES | PES | PES+EN+HP | SS+HP | Tumor | Normal | |
IGHD | 4 | 4 | - | 1 | 1 | 1 |
MPHD | 6 | 6 | 3 | - | 5 | 2 |
NSD | - | - | - | - | - | 1 |
Turner | - | - | - | - | - | 1 |
Total | 10 (28.6 %) | 10(28.6 %) | 3 (8.6 %) | 1 (2.5 %) | 6 (17.1%) | 5 (14.3) |
CONCLUSION: Anomalies of the pituitary- hypothalamic region may be manifested in the stalk, the neurohypophysis, and/or adenohypophysis. The stalk usually categorized as normal or abnormal; in most of the published studies, abnormal includes invisible, truncated, and thin stalks as a single group. The neurohypophysis is generally described as normally located or ectopic. The pathogenesis of GHD is still unclear, but much experience has been gained in recognizing the spectrum of the imaging findings and their clinical implications. It is our impression that nonvisualition of the anterior hypophysis is indicative of MPHD and IGHD, and we also suggest that GHD potentially associated with the primary empty sella syndrome in children.
Figure 1. 16 years old boy with IGHD. Ectopic neurohypophysis, Small sella and an absent stalk
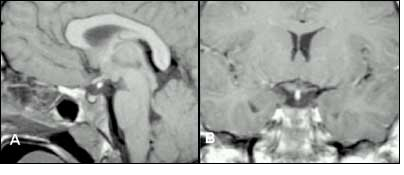
Figure 2. 19 years old girl with MPHD and Empty Sella
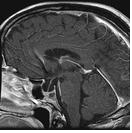
Figure 3. 16, 5 years old boy with IGHD and Partially Empty Sella
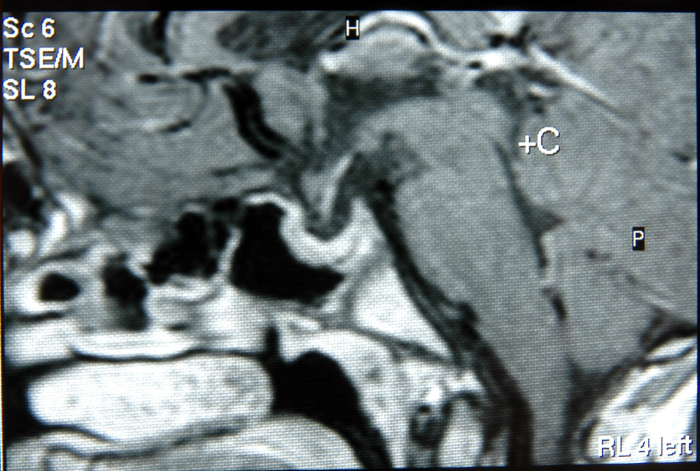
Figure 4. 15 years old boy with IGHD and macroprolactinoma
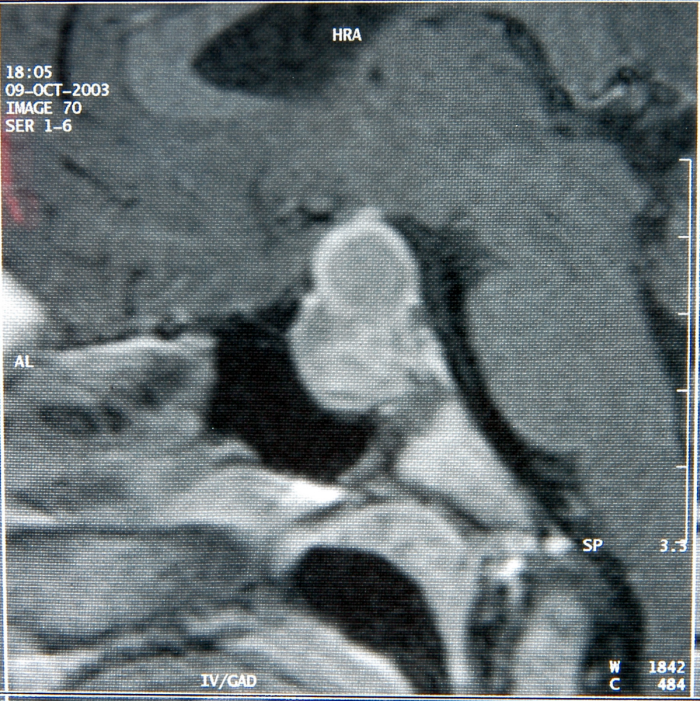
ABSTRACT
INTRODUCTION: Growth Hormone Deficiency (GHD) is an important cause of growth retardation and short stature. The rate of occurrence has been reported in the literature between 1/3480 and 1/30.000. GHD may be idiopathic or associated with organic causes, such as tumor, surgery, trauma or irradiation of the sellar area, and it may be with or without multipl pituitary hormone deficiency. The anterior pituitary and stalk are well defined, and the posterior pituitary is easily identifiable as a hyperintense bright spot on imaging studies. Magnetic Resonance Imaging (MRI) can show characteristic anatomic pituitary abnormalities in patients with GHD, including a small to absent anterior pituitary gland, a small or truncated stalk, and an ectopic posterior pituitary hyperintensity located at the base of the hypothalamus or at the inferior end of the truncated pituitary stalk. In the present report we aimed to analyze the type and frequency of cranial MRI anomalies in patients with GHD, and also to investigate the relationship between craniocerebral images and the presence of isolated GH or multiple pituitary hormone deficiency.
PATIENTS AND METHODS: We evaluated 35 patients who were subsequently diagnosed to have GHD in the endocrinology department of our hospital between October 2002 and June 2006 retrospectively. The diagnosis of GHD was based on auxological and biological criteria; exclusion of other diseases, and a GH peak level of <10 μg/dl in at least two stimulation tests, usually the insulin tolerance test and L-DOPA test done by standard methods. Sex steroid priming was applied for boys and girls if they had pubertal development < genital stage 2 or breast stage < 2, independently of bone age. Hypothyroidism was defined as low or low- normal serum TSH concentration and free T3 concentrations. Plasma ACTH and serum cortisol values were measured in the morning. ACTH deficiency was defined as either a morning serum cortisol concentration of less than 3.6 μg/dl or an impaired cortisol serum concentration rise inferior to 20 μg/dl during insulin- induced hypoglycemia. Hypogonadism was confirmed in both sexes by lack of puberty and no increase in FSH and LH in response to gonadotropin releasing hormone. Cranial imaging studies, with special emphasis on the hypothalamo- pituitary region, were performed in all patients using MRI and were all assessed by the same radiologist. Size of pituitary fossa, pituitary gland, localization of the pituitary gland, homogeneity, enhancement and changes of parasellar structures were evaluated.
RESULTS: Thirty- five adolescents with a mean age of 18.04 ± 3.02 Years (14,5- 23), 22 boys and 13 girls were evaluated. All patients had severe GHD. After studying the pituitary function and determination of karyotype in the girls, the patient classified in to four groups: Isolated GHD (n= 10), Multiple pituitary hormone deficiency (MPHD) (n=23), neurosecretory dysfunction (NSD) (n= 1) and Turner Syndrome (n= 1). Of the 35 patients studied the MRI was abnormal in 30 (85.7 %). In MRI evaluation, 10 (28.6 %) of 35 patients had Empty Sella, 10 (28.6 %) had Partial Empty Sella, 6 (17.1 %) had tumor involving the hypothalamic- pituitary axis, 3 (8.6 %) had Partial Empty Sella, hypoplastic pituitary and ectopic neurohypophysis, and 1 (2.85 %) had small sella and hypoplastic pituitary. 5 of 6 patients with tumor had craniopharyngioma and other one had macroprolactinoma. MRI findings and hormonal status of our patients are presented in a Table 1.
Table 1.MRI findings and hormonal status: ES (Empty Sella), PES (Partial Empty Sella), EN (Ectopic Neurohypophysis), HH (Hipoplazik Hipofiz), SS (Small Sella), IGHD (Isolated pituitary hormone deficiency), MPHD (Multiple pituitary hormone deficiency), NSD (Neurosecretory Dysfunction)
ES
PES
PES+EN+HP
SS+HP
Tumor
Normal
IGHD
4
4
-
1
1
1
MPHD
6
6
3
-
5
2
NSD
-
-
-
-
-
1
Turner
-
-
-
-
-
1
Total
10 (28.6 %)
10(28.6 %)
3 (8.6 %)
1 (2.5 %)
6 (17.1%)
5 (14.3)
CONCLUSION: Anomalies of the pituitary- hypothalamic region may be manifested in the stalk, the neurohypophysis, and/or adenohypophysis. The stalk usually categorized as normal or abnormal; in most of the published studies, abnormal includes invisible, truncated, and thin stalks as a single group. The neurohypophysis is generally described as normally located or ectopic. The pathogenesis of GHD is still unclear, but much experience has been gained in recognizing the spectrum of the imaging findings and their clinical implications. It is our impression that nonvisualition of the anterior hypophysis is indicative of MPHD and IGHD, and we also suggest that GHD potentially associated with the primary empty sella syndrome in children.
Figure 1. 16 years old boy with IGHD. Ectopic neurohypophysis, Small sella and an absent stalk

Figure 2. 19 years old girl with MPHD and Empty Sella

Figure 3. 16, 5 years old boy with IGHD and Partially Empty Sella

Figure 4. 15 years old boy with IGHD and macroprolactinoma

17 - Effects of percutaneous laser ablation treatment in benign solitary thyroid nodules on nodule volume, thyroglobulin and antithyroglobulin levels, and cytopathology of nodule in 1 year follow-up - 2006
Uluslararası Bildiriler 31st Annual Meeting of the European Thyroid Association, Naples, Italy P 203 September 2-6 2006
17. Effects of percutaneous laser ablation treatment in benign solitary thyroid nodules on nodule volume, thyroglobulin and antithyroglobulin levels, and cytopathology of nodule in 1 year follow-up
Author(s): Cakir, B (Cakir, B.); Topaloglu, O (Topaloglu, O.); Gul, K (Gul, K.); Agac, T (Agac,
T.); Aydin, C (Aydin, C.); Dirikoc, A (Dirikoc, A.); Gumus, M (Gumus, M.); Yazicioglu, K
(Yazicioglu, K.); Ersoy, RU (Ersoy, R. U.); Ugras, S (Ugras, S.)
Source: JOURNAL OF ENDOCRINOLOGICAL INVESTIGATION
Volume: 29 Issue: 10 Pages: 876-884
DOI: 10.1007/BF03349190
Published: NOV 2006
Times Cited: 37
35. STATEMENT AND RECOMMENDATIONS ON INTERVENTIONAL ULTRASOUND
AS ATHYROID DIAGNOSTIC AND TREATMENT PROCEDURE
Author(s): Dietrich, CF (Dietrich, Christoph F.); Muller, T (Mueller, Thomas); Bojunga, J
(Bojunga, Joerg); Dong, Y (Dong, Yi); Mauri, G (Mauri, Giovanni); Radzina, M (Radzina,
Maija); Dighe, M (Dighe, Manjiri); Cui, XW (Cui, Xin-Wu); Grunwald, F (Gruenwald, Frank);
Schuler, A (Schuler, Andreas); Ignee, A (Ignee, Andre); Korkusuz, H (Korkusuz, Huedayi)
Source: ULTRASOUND IN MEDICINE AND BIOLOGY
Volume: 44 Issue: 1 Pages: 14-36
Published: JAN 2018
34. Percutaneous laser ablation for benign thyroid nodules: a meta-analysis
Author(s): Sui, WF (Sui, Wei Fan); Li, JY (Li, Jian Yun); Fu, JH (Fu, Jian Hua)
Source: ONCOTARGET
Volume: 8 Issue: 47 Pages: 83225-83236
Published: OCT 10 2017
33. Image-guided thermal ablation of benign thyroid nodules
Author(s): Mainini, AP (Mainini, Anna Pisani); Monaco, C (Monaco, Cristian); Pescatori, LC
(Pescatori, Lorenzo Carlo); De Angelis, C (De Angelis, Chiara); Sardanelli, F (Sardanelli,
Francesco); Sconfienza, LM (Sconfienza, Luca Maria); Mauri, G (Mauri, Giovanni)
Source: JOURNAL OF ULTRASOUND
Volume: 20 Issue: 1 Pages: 11-22
Published: MAR 2017
32. The percentage of serum thyroglobulin rise in the first-week did not predict the eventual
success of high-intensity focussed ablation (HIFU) for benign thyroid nodules
Author(s): Lang, BHH (Lang, Brian H. H.); Woo, YC (Woo, Yu Cho); Chiu, KWH (Chiu,
Keith W. H.)
Source: INTERNATIONAL JOURNAL OF HYPERTHERMIA
Volume: 33 Issue: 8 Pages: 882-887
Published: 2017
31. A comparison of laser with radiofrequency ablation for the treatment of benign thyroid
nodules: a propensity score matching analysis
Author(s): Pacella, CM (Pacella, Claudio Maurizio); Mauri, G (Mauri, Giovanni); Cesareo, R
(Cesareo, Roberto); Paqualini, V (Paqualini, Valerio); Cianni, R (Cianni, Roberto); De Feo, P
(De Feo, Pierpaolo); Gambelunghe, G (Gambelunghe, Giovanni); Raggiunti, B (Raggiunti,
Bruno); Tina, D (Tina, Doris); Deandrea, M (Deandrea, Maurilio); Limone, PP (Limone, Pier
Paolo); Mormile, A (Mormile, Alberto); Giusti, M (Giusti, Massimo); Oddo, S (Oddo, Silvia);
Achille, G (Achille, Gaetano); Di Stasio, E (Di Stasio, Enrico); Misischi, I (Misischi, Irene);
Papini, E (Papini, Enrico)
Source: INTERNATIONAL JOURNAL OF HYPERTHERMIA
Volume: 33 Issue: 8 Pages: 911-919
Published: 2017
30. Laser, radiofrequency, and ethanol ablation for the management of thyroid nodules
Author(s): Papini, E (Papini, Enrico); Gugliemi, R (Gugliemi, Rinaldo); Pacella, CM (Pacella,
Claudio Maurizio)
Source: CURRENT OPINION IN ENDOCRINOLOGY DIABETES AND OBESITY
Volume: 23 Issue: 5 Pages: 400-406
Published: OCT 2016
29. Ultrasound-guided percutaneous laser ablation in treating symptomatic solid benign thyroid
nodules: Our experience in 45 patients
Author(s): Achille, G (Achille, Gaetano); Zizzi, S (Zizzi, Stefania); Di Stasio, E (Di Stasio,
Enrico); Grammatica, A (Grammatica, Alberto); Grammatica, L (Grammatica, Luciano)
Source: HEAD AND NECK-JOURNAL FOR THE SCIENCES AND SPECIALTIES OF THE
HEAD AND NECK Volume: 38 Issue: 5 Pages: 677-
682 DOI: 10.1002/hed.23957 Published: MAY 2016
28. Outcomes and Risk Factors for Complications of Laser Ablation for Thyroid Nodules: A
Multicenter Study on 1531 Patients
Author(s): Pacella, CM (Pacella, C. M.); Mauri, G (Mauri, G.); Achille, G (Achille, G.);
Barbaro, D (Barbaro, D.); Bizzarri, G (Bizzarri, G.); De Feo, P (De Feo, P.); Di Stasio, E (Di
Stasio, E.); Esposito, R (Esposito, R.); Gambelunghe, G (Gambelunghe, G.); Misischi, I
(Misischi, I.); Raggiunti, B (Raggiunti, B.); Rago, T (Rago, T.); Patelli, GL (Patelli, G. L.);
D'Este, S (D'Este, S.); Vitti, P (Vitti, P.); Papini, E (Papini, E.)
Source: JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM
Volume: 100 Issue: 10 Pages: 3903-3910
Published: OCT 2015
27. Laser Thermal Ablation of Thyroid Benign Nodules
Author(s): Shahrzad, MK (Shahrzad, Mohammad Karim)
Source: JOURNAL OF LASERS IN MEDICAL SCIENCES
Volume: 6 Issue: 4 Pages: 151-156
Published: FAL 2015
26. Prospective Study of Effectiveness of Ultrasound-Guided Radiofrequency Ablation Versus
Control Group in Patients Affected by Benign Thyroid Nodules
Author(s): Cesareo, R (Cesareo, Roberto); Pasqualini, V (Pasqualini, Valerio); Simeoni, C
(Simeoni, Carla); Sacchi, M (Sacchi, Marco); Saralli, E (Saralli, Erminio); Campagna, G
(Campagna, Giuseppe); Cianni, R (Cianni, Roberto)
Source: JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM
Volume: 100 Issue: 2 Pages: 460-466
Published: FEB 2015
25. Thyroid nodule morphology affects the efficacy of ultrasound-guided interstitial laser
ablation: A nested case-control study
Author(s): Gambelunghe, G (Gambelunghe, Giovanni); Bini, V (Bini, Vittorio); Stefanetti, E
(Stefanetti, Elisa); Colella, R (Colella, Renato); Monacelli, M (Monacelli, Massimo); Avenia, N
(Avenia, Nicola); De Feo, P (De Feo, Pierpaolo)
Source: INTERNATIONAL JOURNAL OF HYPERTHERMIA
Volume: 30 Issue: 7 Pages: 486-489
Published: NOV 2014
24. Long-term Efficacy of Ultrasound-Guided Laser Ablation for Benign Solid Thyroid
Nodules. Results of a Three-Year Multicenter Prospective Randomized Trial
Author(s): Papini, E (Papini, E.); Rago, T (Rago, T.); Gambelunghe, G (Gambelunghe, G.);
Valcavi, R (Valcavi, R.); Bizzarri, G (Bizzarri, G.); Vitti, P (Vitti, P.); De Feo, P (De Feo, P.);
Riganti, F (Riganti, F.); Misischi, I (Misischi, I.); Di Stasio, E (Di Stasio, E.); Pacella, CM
(Pacella, C. M.)
Source: JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM
Volume: 99 Issue: 10 Pages: 3653-3659
Published: OCT 2014
23. The advent of ultrasound-guided ablation techniques in nodular thyroid disease: Towards a
patient-tailored approach
Author(s): Papini, E (Papini, Enrico); Pacella, CM (Pacella, Claudio M.); Misischi, I (Misischi,
Irene); Guglielmi, R (Guglielmi, Rinaldo); Bizzarri, G (Bizzarri, Giancarlo); Dossing, H
(Dossing, Helle); Hegedus, L (Hegedus, Laszlo)
Source: BEST PRACTICE & RESEARCH CLINICAL ENDOCRINOLOGY &
METABOLISM
Volume: 28 Issue: 4 Pages: 601-618
Published: AUG 2014
22. Microwave ablation of benign thyroid nodules
Author(s): Yang, YL (Yang, Yin-Long); Chen, CZ (Chen, Cheng-Ze); Zhang, XH (Zhang,
Xiao-Hua)
Source: FUTURE ONCOLOGY
Volume: 10 Issue: 6 Pages: 1007-1014
Published: MAY 2014
21. DIAGNOSIS OF ENDOCRINE DISEASE Thyroid ultrasound ( US) and US-assisted
procedures: from the shadows into an array of applications
Author(s): Papini, E (Papini, Enrico); Pacella, CM (Pacella, Claudio M.); Hegedus, L
(Hegedus, Laszlo)
Source: EUROPEAN JOURNAL OF ENDOCRINOLOGY
Volume: 170 Issue: 4 Pages: R133-R146
Published: APR 2014
20. Nonsurgical, Image-Guided, Minimally Invasive Therapy for Thyroid Nodules
Author(s): Gharib, H (Gharib, Hossein); Hegedus, L (Hegedues, Laszlo); Pacella, CM (Pacella,
Claudio Maurizio); Baek, JH (Baek, Jung Hwan); Papini, E (Papini, Enrico)
Source: JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM
Volume: 98 Issue: 10 Pages: 3949-3957
Published: OCT 2013
19. Ultrasound-Guided Interstitial Laser Ablation for Thyroid Nodules Is Effective Only at
High Total Amounts of Energy: Results From a Three-Year Pilot Study
Author(s): Gambelunghe, G (Gambelunghe, Giovanni); Fede, R (Fede, Raffaela); Bini, V (Bini,
Vittorio); Monacelli, M (Monacelli, Massimo); Avenia, N (Avenia, Nicola); D'Ajello, M
(D'Ajello, Michele); Colella, R (Colella, Renato); Nasini, G (Nasini, Giovanni); De Feo, P (De
Feo, Pierpaolo)
Source: SURGICAL INNOVATION
Volume: 20 Issue: 4 Pages: 345-350
Published: AUG 2013
18. Use of Radiofrequency Ablation in Benign Thyroid Nodules: A Literature Review and
Updates
Author(s): Wong, KP (Wong, Kai-Pun); Lang, BHH (Lang, Brian Hung-Hin)
Source: INTERNATIONAL JOURNAL OF ENDOCRINOLOGY
Article Number: 428363
Published: 2013
17. Image-guided percutaneous ablation therapies for local recurrences of thyroid tumors
Author(s): Pacella, CM (Pacella, C. M.); Papini, E (Papini, E.)
Source: JOURNAL OF ENDOCRINOLOGICAL INVESTIGATION
Volume: 36 Issue: 1 Pages: 61-70
Published: JAN 2013
16. The administration of anesthetic in the thyroid pericapsular region increases the possibility
of side effects during percutaneous laser photocoagulation of thyroid nodules
Author(s): Gambelunghe, G (Gambelunghe, Giovanni); Bini, V (Bini, Vittorio); Monacelli, M
(Monacelli, Massimo); Avenia, N (Avenia, Nicola); D'Ajello, M (D'Ajello, Michele); Colella, R
(Colella, Renato); De Feo, P (De Feo, Pierpaolo)
Source: LASERS IN SURGERY AND MEDICINE
Volume: 45 Issue: 1 Pages: 34-37
Published: JAN 2013
15. Pathological Findings of Thyroid Nodules After Percutaneous Laser Ablation
Author(s): Piana, S (Piana, Simonetta); Riganti, F (Riganti, Fabrizio); Froio, E (Froio,
Elisabetta); Andrioli, M (Andrioli, Massimiliano); Pacella, CM (Pacella, Claudio M.); Valcavi,
R (Valcavi, Roberto)
Source: ENDOCRINE PATHOLOGY
Volume: 23 Issue: 2 Pages: 94-100
Published: JUN 2012
14. Tracheal laceration after laser ablation of nodular goitre
Author(s): Di Rienzo, G (Di Rienzo, Gaetano); Surrente, C (Surrente, Corrado); Lopez, C
(Lopez, Camillo); Quercia, R (Quercia, Rosatea)
Source: INTERACTIVE CARDIOVASCULAR AND THORACIC SURGERY
Volume: 14 Issue: 1 Pages: 115-116
Published: JAN 2012
13. Interstitial Laser Photocoagulation for Benign Thyroid Nodules: Time to Treat Large
Nodules
Author(s): Amabile, G (Amabile, Gerardo); Rotondi, M (Rotondi, Mario); Pirali, B (Pirali,
Barbara); Dionisio, R (Dionisio, Rosa); Agozzino, L (Agozzino, Lucio); Lanza, M (Lanza,
Michele); Buonanno, L (Buonanno, Luciano); Di Filippo, B (Di Filippo, Bruno); Fonte, R
(Fonte, Rodolfo); Chiovato, L (Chiovato, Luca)
Source: LASERS IN SURGERY AND MEDICINE
Volume: 43 Issue: 8 Pages: 797-803
Published: SEP 2011
12. Thermal Ablation for Benign Thyroid Nodules: Radiofrequency and Laser
Author(s): Baek, JH (Baek, Jung Hwan); Lee, JH (Lee, Jeong Hyun); Valcavi, R (Valcavi,
Roberto); Pacella, CM (Pacella, Claudio M.); Rhim, H (Rhim, Hyunchul); Na, DG (Na, Dong
Gyu)
Source: KOREAN JOURNAL OF RADIOLOGY
Volume: 12 Issue: 5 Pages: 525-540
Published: SEP-OCT 2011
11. Long-term outcome following interstitial laser photocoagulation of benign cold thyroid
nodules
Author(s): Dossing, H (Dossing, Helle); Bennedbk, FN (Bennedbk, Finn Noe); Hegedus, L
(Hegedus, Laszlo)
Source: EUROPEAN JOURNAL OF ENDOCRINOLOGY
Volume: 165 Issue: 1 Pages: 123-128
Published: JUL 2011
10. Minimally Invasive Ablation of a Toxic Thyroid Nodule by High-Intensity Focused
Ultrasound
Author(s): Esnault, O (Esnault, O.); Rouxel, A (Rouxel, A.); Le Nestour, E (Le Nestour, E.);
Gheron, G (Gheron, G.); Leenhardt, L (Leenhardt, L.)
Source: AMERICAN JOURNAL OF NEURORADIOLOGY
Volume: 31 Issue: 10 Pages: 1967-1968
Published: NOV-DEC 2010
9. Percutaneous Laser Ablation of Cold Benign Thyroid Nodules: A 3-Year Follow-Up Study
in 122 Patients
Author(s): Valcavi, R (Valcavi, Roberto); Riganti, F (Riganti, Fabrizio); Bertani, A (Bertani,
Angelo); Formisano, D (Formisano, Debora); Pacella, CM (Pacella, Claudio M.)
Source: THYROID
Volume: 20 Issue: 11 Pages: 1253-1261
Published: NOV 2010
8. Initial Report of the Results of Percutaneous Laser Ablation of Benign Cold Thyroid
Nodules: Evaluation of Histopathological Changes After 2 Years
Author(s): Cakir, B (Cakir, Bekir); Ugras, NS (Ugras, Nevzat Serdar); Gul, K (Gul, Kamile);
Ersoy, R (Ersoy, Reyhan); Korukluoglu, B (Korukluoglu, Birol)
Source: ENDOCRINE PATHOLOGY
Volume: 20 Issue: 3 Pages: 170-176
Published: SEP 2009
7. Cold Benign Thyroid Nodule Volume Reduction Predictability After Percutaneous Ethanol
Injection
Author(s): Nirchio, V (Nirchio, Vincenzo); Nirchio, F (Nirchio, Francesco); Crocetti, U
(Crocetti, Umberto); Tizzani, P (Tizzani, Paola); Trischitta, V (Trischitta, Vincenzo); Zingrillo,
M (Zingrillo, Matteo)
Source: ACTA CYTOLOGICA
Volume: 53 Issue: 3 Pages: 292-296
Published: MAY-JUN 2009
6. HISTOLOGICAL CHANGES IN BENIGN SOLITARY THYROID NODULES - A
PROSPECTIVE MORPHOLOGICAL STUDY
Author(s): Gheorghisan-Galateanu, A (Gheorghisan-Galateanu, A.); Ioachim, D (Ioachim, D.)
Source: ACTA ENDOCRINOLOGICA-BUCHAREST
Volume: 5 Issue: 2 Pages: 221-231
Published: APR-JUN 2009
5. Percutaneous laser ablation of benign and malignant thyroid nodules
Author(s): Papini, E (Papini, Enrico); Bizzarri, G (Bizzarri, Giancarlo); Pacella, CM (Pacella,
Claudio M.)
Source: CURRENT OPINION IN ENDOCRINOLOGY DIABETES AND OBESITY
Volume: 15 Issue: 5 Pages: 434-439
Published: OCT 2008
4. Subcapsular hematoma complication during percutaneous laser ablation to a hypoactive
benign solitary thyroid nodule
Author(s): Cakir, B (Cakir, Bekir); Gul, K (Gul, Kamile); Ersoy, R (Ersoy, Reyhan); Topaloglu,
O (Topaloglu, Oya); Korukluoglu, B (Korukluoglu, Birol)
Source: THYROID
Volume: 18 Issue: 8 Pages: 917-918
Published: AUG 2008
3. Percutaneous laser ablation of an autonomous thyroid nodule: Effects on nodule size and
histopathology of the nodule 2 years after the procedure
Author(s): Cakir, B (Cakir, Bekir); Gul, K (Gul, Kamile); Ugras, S (Ugras, Serdar); Ersoy, R
(Ersoy, Reyhan); Topaloglu, O (Topaloglu, Oya); Agac, T (Agac, Tuba); Aydin, C (Aydin,
Cevdet); Dirikoc, A (Dirikoc, Ahmet); Gumus, M (Gumus, Mehmet); Korukluoglu, B
(Korukluoglu, Birol); Kusdemir, A (Kusdemir, Ahmet)
Source: THYROID
Volume: 18 Issue: 7 Pages: 803-805
Published: JUL 2008
2. Randomized prospective study comparing a single radioiodine dose and a single laser
therapy session in autonomously functioning thyroid nodules
Author(s): Dossin, H (Dossin, Helle); Bennedbwk, FN (Bennedbaek, Finn Noe); Bonnema, SJ
(Bonnema, Steen Joop); Grupe, P (Grupe, Peter); Hegedus, L (Hegedues, Laszlo)
Source: EUROPEAN JOURNAL OF ENDOCRINOLOGY
Volume: 157 Issue: 1 Pages: 95-100
Published: JUL 2007
1. Ultrasound-guided percutaneous laser ablation treatment in inoperable aggressive course
anaplastic thyroid carcinoma: The introduction of a novel alternative palliative therapy - Second
experience in the literature
Author(s): Cakir, B (Cakir, B.); Topaloglu, O (Topaloglu, O.); Gul, K (Gul, K.); Agac, T
(Agac, T.); Aydin, C (Aydin, C.); Dirikoc, A (Dirikoc, A.); Ersoy, RU (Ersoy, R. U.); Gumus,
M (Gumus, M.); Yazicioglu, K (Yazicioglu, K.); Yalcin, B (Yalcin, B.); Demirkazik, A
(Demirkazik, A.); Icli, F (Icli, F.); Ceyhan, K (Ceyhan, K.)
Source: JOURNAL OF ENDOCRINOLOGICAL INVESTIGATION
Volume: 30 Issue: 7 Pages: 624-625
Published: JUL-AUG 2007
16 - Treatment of euthyroid benign solid thyroid nodules by ultrasound-guided low power Interstitial Laser Photocoagulation procedure- Initial results from Turkey - 2005
Uluslararası Bildiriler 13th International Thyroid Congress, Buenos Aires, Argentina P 210, October 30- November 5, 2005
ABSTRACT
Aim:To evaluate the effects of ultrasonography (US)-guided low power interstitial laser photocoagulation (ILP) therapy on the volume of benign solid thyroid nodules, thyroid function tests and any nodule-related symptoms of patients.
Materials and methods:The criteria for entry into the study were presence of hypofunctioning and benign thyroid nodules also causing local compression symptoms and cosmetic problems. Twelve patients (4 men and 8 women; mean age, 49.20±16.10 years) fulfilling the entry criteria were enrolled in the study. ILP procedure was performed to fifteen thyroid nodules and followed for three months. Low power ILP was performed with use of a 810 nm diode electronic laser with continous 7.5 mHz linear probe US guidance. Patients were treated for 130-2080 seconds with an output power of 3-5 W. The energy given was 389-10398 Joule, The protocol was approved by the local ethics committee. Prior to procedure the patients all gave signed informed consent. Comparison of results was performed by Wilcoxon signed ranks test.
Results:Although the mean initial nodule volume measured with US was 11,97 ± 8.78 ml, 3 months after the procedure the average volume was established as 5.88±5.66 ml. 51% nodule volume reduction was significant( p = 0.001). All of the patients were euthyroid biochemically. Before and 3 months after the procedure no significant changes were established in TSH, free T3 and free T4 levels (p = 0.460). Local compression symptoms and cosmetic problems were decreased 3 months after the procedure. No serious complications were encountered during the procedure. Of the 12 study patients, 4 (33.33%) complained of pain spreading toward the ear during the procedure but disappeared after the termination of the procedure.
Conclusion::US-guided low power ILP is a successful nonsurgical alternative for the treatment of benign solid thyroid nodules in patients who are not candidates for surgical treatment or who refuse to undergo a surgical procedure.
15 - Bone Mineral Density and Urinary N-Telopeptide Levels in Premenopausal Women with Thyrotoxicosis - 2001
Uluslararası Bildiriler 24th Congress of Endocrinology and Metabolic Diseases of Turkey Joint Meeting with the American Association of Clinical Endocrinologists, İstanbul, Endocrine Practice Supplement for September/October, P 69, 2001
ABSTRACT
Aim:Thyrotoxicosis causes increases in bone resorption due to increased osteoblastic activity and indirect effects of osteoblasts, sometimes leading to secondary osteoporosis. Our aim was to evaluate the relation of urinary N-telopeptide (NTx) levels with changes in bone and mineral metabolism in premenopausal women with thyrotoxicosis.
Methods:20 premenopausal patients With thyrotoxicosis are involved in the study. Age-matched 20 euthyroid premenopausal healthy women served as the controls. Serum TSH, free T3 and free T4 levels are measured on fasting morning venous blood sample. NTx level is measured on 24 hour urine sample. Bone mineral densities of lumbar vertebrae and hip are measured in lumbar and hip region.
Results: Thyrotoxic patients had lower lumbar and hip mineral densities (1.025 ± 0.04 vs. 1.185 ± 0.03. p<0.001; and 0.890 ± 0.04 vs. 1.031 ± 0.03 gr/cm² P<0.01, respectively), and higher urinary NTx level ( 113.00 ± 12.97 vs. 32.94±3.25 nmolBCE/mmol CR, respectively, P<0.01) than the controls. Urinary NTx level was correlated with free T3 ands free T4 levels in thyrotoxic patients (r = 0.74, P<0.01. and r=0.63, p=0.03, respectively). But. there was no relation between BMD and NTx.
Conclusions:Our results suggest that bone resorption is increased, and NTx, a marker of bone resorption, is directlv related to the severity of thyrotoxicosis in premenopausal patients with thyrotoxicosis. Determination of urinary NTx levels together with BMD may be helpful for the early diagnosis and taking proper measures.
14 - The effect of Metformin and Gliclazide on the Relation Between Beta Cell Function and Leptin in Type 2 Diabetes Mellitus - 2001
Uluslararası Bildiriler 61. Scientific Session of American Diabetes Association, Philadelphia, Vol. 50, Suppl 2, A420, 1747PO, Diabetes, 2001
ABSTRACT
Leptin is an adipose tissue homone. Leptin has an acute inhibitory effect on insulin synthesis, and the synthesis and secretion of leptin is regulated by insulin. Although ob/ob mice are characterized by obesity and diabetes mellitus, leptin levels in men with type 2 diabetes mellitus are not different from healthy humans. In addition, there are few studies in the literature that investigated the relation between oral antidiabetic agents, leptin, and beta cell function. In this study we tried to find out the effect of metformin and gliclazide on the interaction relation between leptin and beta cell function in patients with type 2 diabetes mellitus. Twenty female patients receiving only metformin (MET) therapy and 20 female patients receiving only gliclazide (GLC) therapy for at least 6 months are involved in the study. Twenty age matched nondiabetic healthy female subjects formed the control group. All patients received 300 kilocalories of standard diet after 12 hours of fasting and venous blood samples are obtained at 0,60, and 120 minutes for plasma glucose, serum insulin, c-peptide and insulin assays. The HOMA-IR was significantly higher (6.4±4.9 vs. 7.9±3.8 vs. 3.3±1.7, respectively) and HOMA-BETA was significantly lower (110.7±174.1 vs. 92.7±117.8 vs. 577.6±1165.5, respectively) in the MET and the GLC groups than the control group. The area under the curve of leptin (AUC-leptin), and AUC-c-peptide were similar between the three groups. The AUC-insulin was greater in GLC group than the MET group (4491.0±3620.9 vs. 2983.1±1353.7, respectively; p<0.05); the difference between the control group and the two diabetic groups was not significant. There was a significant correlation between HOMA-BETA and AUC-leptin in the control (r=0.49, p=0.03), and in the MET (r=0.71, p<0.001) groups, but not in the GLC (r=0.35, p=0.13) group. In conclusion, our data indicate that the interaction between leptin and beta cell function is maintained by metformin, but disrupted by gliclazide treatment.
13 - Relation of Urinary N-Telopeptide Levels with Age, Duration of Menopause and Bone Mineral Density in Patients with Postmenopausal Osteoporosis - 2001
Uluslararası Bildiriler 11th Balkan Congress of Endocrinology, İstanbul, P 56, 2001
ABSTRACT
It is well known that menopause is associated with increase in bone loss, and early menopause causes further increases and shortens this process. The aim of this study was to investigate the relation between urinary N-telopeptide (NTx), age, bodv mass index (BMI), waist/hip ratio, duration of menopause, and bone mineral density (BMD) in patients with postmenopausal osteoporosis. 15 patients with postmenopausal osteoporosis formed the patients group. 15 nonosteoporotic postmenopausal patients matched for age. BMI. and duration of menopause with the patients formed the control group. Patients had higher urinary NTx levels than the controls (90.83±7.17 vs. 33.27±3.92 nmolBCE/mmol CR. respectively. p< 0.001). In the patient group, urinary NTx levels showed positive correlation with the patient's age and the durastion of menopause (r = 0.64, p<0.01. and r = 0.70, p<0.01, respectively). Our results show that urinary NTx may be used a sensitive marker of bone resorption in the diagnosis and the follow-up of treatment in postmenopausal osteoporosis, supporting the results of previous studies.
12 - Cholestatic Hepatitis Due to Propylthiouracil - 2001
Uluslararası Bildiriler 24th Congress of Endocrinology and Metabolic Diseases of Turkey Joint Meeting with the American Association of Clinical Endocrinologists, İstanbul, Endocrine Practice Supplement for September/October, P 6, 2001
ABSTRACT
Objectives:Hepatotoxcity due to proplythiouracyl (PTU) is reported seldom. Here we present a 21 years old female patient with cholestatic hepatitis due to PTU.
Case:The patient had history of 150 mg/day PTU usage for 1 month. She had noticed nausea. itching. and jaundice for 1 week Thyroid gland was grade la palpable and there was prominent jaundice on the sclera and skin physical exammation. Laboratory analysis yielded the following: Total bilirubin: 18.5 mg/dl. direct bilirubin 12.7 mg/dl. SGOT:101 U/L. SGPT: 129 mg/dl. alkaline phosphatase: 147 U/L g-glutamyl transpeptidase 76 U/L. INR 1.74 s. TSH: 0.829 mIU/L. free T3: 1.94 pg/ml. free T4: 1.02 ng/dl. Thyroid I131-uptake eas 21.2% at 4 hours and 55.2% at 24 hours. Ultrasonographv revealed an 8x4 mm nodule at the right and an 8x7 mm nodule the left lobes of the thvroid. Uptake was diffuse and homogenous on the thyroid scintigraphy. Serologic analysis for hepatitis A. B. and C. Toxoplasmosis, rubella, cytomegalovirus, herpes simplex, and Ebslem-Barr were negative. Antinuclear, antimitochondrial, M2 tvpe antimitochondrial, anti smooth muscle, and liver kidney microsomal (LKM-1 ) antibodies were also negative. Serum ferritin level was normal. Urinar copper level was 67 µg/ 24 saat (3-35). serum cerruloplasmin level was 77 mg/dl. and a-1 antitripsin level was 211 mg/dl (80-200). Cytologic examination of the needle aspiration of the liver revealed chronic intrahepatic cholestasis compatible with drug hepatotoxicity 10 mCi radioactive iodine is administered for thyrotoxicosis. Then, the patient is started on 80 mg/d prednisone and 500 mg/d ursodeoxycholic acid for the treatment of intrahepatic cholestasis. Total and direct bilirubin levels tell down to 12. 3 and 8.8 mg/dl at the first month and to 3.4 and 2.2 mg/dl at the end of the second month. Respectively. The patients is still on follow-up.
Conclusion:Wc presented this case due to rarity of intrahepatic cholestasis due to PTU toxicity. Glucocorticoid and ursodeoxycholic acid seems, to be beneficial in the treatment of Ptu induced cholestatic hepatitis.
11 - Serum C-Peptide Levels in Type 2 Diabetic Patients with Macroangiopathy - 2001
Uluslararası Bildiriler 24th Congress of Endocrinology and Metabolic Diseases of Turkey Joint Meeting with the American Association of Clinical Endocrinologists, İstanbul, Endocrine Practice Supplement for September/October, P 45, 2001
ABSTRACT
Objectives:It is know that hyperglycemia predisposes to micro- and macro-vascular disease. Although fasting insulin levels are used in the calculation of insulin resistance. because c-peptide is not metabolized in the liver and has a longer half-life its levels are more reliable in reflecting insulin secretion. Recent studies yielded controversial results about the role of c-peptide levels in the development of macroangiopathy in patients with type 2 diabetes mellitus (DM). In this study we aimed to investigate he relation between macroangiopathy and serum c-peptide levels in patients with type 2 DM.
Methods:Twenty-six female type 2 diabetic patients with coronary artery disease are included in the study. Twenty-five age-matched type 2 diabetic patients without any macrovascular disease served as the control group. Plasma total and HDL cholesterol, triglyceride, c-peptide and insulin levels are measured.
Results:Two groups were comparable with regard to age, HbAlc, and disease duration. Type 2 DM patients with coronary artery disease had higher plasma c-peptide 8.7±8.2 vs. 2.4± 1.2 ng/ml, respectively: p < 0.01). and insulin levels (41.2 ± 56.7 vs. 17.9 ± 10.7 microlU/ml, respectively; p<0.05), and lower serum HDL-cholesterol levels (38.6 ± 10.6 vs. 46.8 ± 12.7 mg/dl, respectively; p<0.01) than the controls. There were positive correlations between HbAlc and total-cholesterol (r=39; p=0.48) and HDL-cholesterol (r=0.4; p = 0.42) in patients with coronary artery disease but not in patients without macroangiopathy.
Conclusions:Our results indicate that type 2 DM patients with macroangiopathy have higher c-peptide levels even when fasting plasma glucose and HbAlc levels are similar. Whether higher c-peptide levels may be a predictor or an indicator of coronary artery disease remains to be determined.
10 - The Effect of Alendronat on Lipid Levels - 2001
Uluslararası Bildiriler 24th Congress of Endocrinology and Metabolic Diseases of Turkey Joint Meeting with the American Association of Clinical Endocrinologists, İstanbul, Endocrine Practice Supplement for September/October, P 71, 2001
ABSTRACT
Aims:Aminobiphosphonates are known to inhibit squalene synthase. But whether they influence serum lipid levels is not known. In this study we investigated the effects of an aminobiphosphonate, alendronate, on serum lipid levels.
Materials and methods:Thirty three patients with postmenopausal osteoporosis formed the patient group. Twenty nine healthy postmenopausal subjects formed the control group. Patient group has been administered alendronate 10 mg/day. Apolipoprotein A (ApoA), Apolioprotein B (ApoB), Lp(a), trigleceride. total and HDL-cholesterol levels are measured before and at the end of 1 year alendronate treatment.
Results:Serum total and LDL cholesterol, Lp(a), triglyceride did not change significantly in either groups. We observed significant decreases in ApoA, and HDL-cholesterol levels and an increase in ApoB levels with treatment in both the patient (from 165.9±18.4 to 157.2±16.0 mg/dl, p=0.027; from 49.7±6.5 to 46.5±6.8 mg/dl, p=0.001: and from 88.8±17.8 to 103.4±15.0 mg/dl, p<0.001, respectively) and the control groups (from 163.3±26.6 to 151.6±23.5 mg/dl p=0.006; from 46.6±6.6 to 43.1±4.6 mg/dl, p=0.001; and from 90.8±20.2 to 103.7±20.2 mg/dl, p=0.001, respectively). The differences in the change in these parameters were not significant between the two groups.
Conclusions:Oral alendronate treatment does not influence serum lipid levels significantly.
9 - The Effect of Different Therapy Regimens on Bone Mineral Density in Postmenopausal Women: A Retrospective Study - 2001
Uluslararası Bildiriler 24th Congress of Endocrinology and Metabolic Diseases of Turkey Joint Meeting with the American Association of Clinical Endocrinologists, İstanbul, Endocrine Practice Supplement for September/October, P 70, 2001
ABSTRACT
Aim:Our aim was to investigate the effects of one year treatment with alendronate or etidronate or calcitonin on bone mineral density (BMD) in postmenopausal women with osteoporosis.
Materials and methods:184 postmenopausal women with osteoporosis whose diagnosis had been made with BMD received different therapv regimens. Among these 184 patients with postmenopausal osteoporosis 128 had received 10 mg alendronate. 27 had received 400 mg cyclic ethidronate, and 29 had received 100 U calcitonin daily for one year. The pre- and post-treatment BMD values of the patients are investigated retrospectively.
Results:Pretreatment BMD values were 0.719±0.09 gr/cm², 0.800±0.09 gr/cm², and 0.763±0.09 gr/cm² in the alendronate, ethidtronate, and calcitonin groups, respectively. Posttreatment BMD values were 0.758±0.10 gr/cm², 0.829±0.06 gr/cm², and 0.753±0.08 gr/cm² in the alendronate, ethidronate and calcitonin groups. Respectively. While there were significant increases in BMD in the alendronate (p<0.001 ) and the ethidronate (p=0.002) groups, there was an insignificant decrease in BMD in patients who had received group used calcitonin (p>0.05).
Conclusions:Our results show that alcndronate and etidronate are more effective than calcitonin in the treatment of postmenopausal osteoporosis.
8 - Plasma Tumor Necrosis Factor-alpha Levels and Insulin Resistance in Nondiabetic Hypertensive Subjects - 2001
Uluslararası Bildiriler 37th EASD Annual Meeting, Glasgow, United Kingdom, P 39, 2001
ABSTRACT
Aims:Recent studies have shown that tumor necrosis factor-alpha(TNF-alpha) is associated with insulin resistance. However, whether TNF-alpha is related to insulin resistance in hypertensive subjects is still controversial. The aim of this study was to the determine the status of TNF-alpha and insulin resistance in hypertension.
Materials and Methods:Newly diagnosed nondiabetic 17 essentially hypertensive (6 men, 11 women) patients, and 11 conrol healthy subjects (5 men, 6 women) are involved in the study. Body mass index (BMI), waist/hip ratio (WHR), insulin, subcutaneous fat dssue tissue thickness, fasting blood glucose, cholesterol, triglyceride, and TNF-alpha levels were measured. Insulin resistance is assessed according to homeostasis of assessment (HOMA-IR).
Results:Serum insulin (8.4±2.7 vs. 6.1±1.4 mIU/ml; p<0.01), triglyceride (245.0±39.9 vs 193.0±22.8 mg/dl; p<0.01), and TNF-alpha (4.1±1.4 vs. 1.7±1.7 pg/ml; p<0.001) levels, and HOMA-IR (2.0±0.8 vs. 1.3±0.3; p<0.001) were significantly higher in the hypertensive patietts compared to the normotensive control group. There were positive correlations between TNF-alpha levels and body mass index (r=0.5, p<0.01), subcutaneous fat tissue thickness (r=0.56, p=0.002), cholesterol (r=0.51, p=0.006) and triglyceride (r=0.57, p=0.002) levels, and positive correlations between HOMA and subcutaneous fat tissue thickness (r=0.43, p<0.03) in the whole study group. However were no correlation of either TNF-alpha or HOMA-R with any of the study parameters when hypertensive and normotensive groups are analyzed separately.
Conclusions:Our data revealed that hypertensive patients have insulin resistance and higher TNF-alpha levels, but is no relation between TNF-alpha levels and insulin resistance.
7 - Effects of Flutamide and Ethynilestradiol on Plasma Lipids in Patients with Polycystic Ovary Disease - 2000
Uluslararası Bildiriler 23rd Congress of Endocrinology and Metabolic Diseases of Turkey Joint Meeting with the Europan Federation of Endocrine Societies, Ankara, A133, 71, Journal of Endocrinologıcal Investigation Vol. 23 (Suppl. To no. 7) 2000
ABSTRACT
Although the effects of estrogens on plasma lipid levels are clearly understood, the effects of androgens and antiandrogens are not studied well. In this study, we tried to find out whether plasma lipid levels change with ethynilestradiol plus cyproterone-acetate and flutamide in patients with PCO A total of 29 patients with PCO are included in the study. Sixteen of the patients received ethynilestradiol plus ethynilestradiol (E group), and 13 patients received flutamide (F group) for 6 months. The E and the F groups had similar age, body mass indices (BMI), and waist/hip (W/H) ratios, hirsutism scores, LH, estradiol, testesterone, free testosterone, cortisol, 17-0H-progesterone, total-, HDL- and LDL- cholesterol levels before the treatment period. Pretreatment serum triglyceride level was lower in the F goup then the E group (68.2 ± 20.1 vs. 133.3 ± 52.8 mg/dL, respectively; p <0.001). Treatment resulted in significant increases in BMI (p = 0.01), and serum triglyceride levels (p = 0.02); and significant decline in hirsutism score (p < 0.001), LH (p < 0.003), testosterone (p = 0.008), free testosterone (p < 0.001), and cholesterol levels (p = 0.004) in the E group. There occurred a significant decline in hirsutism score (p = 0.005), and cholesterol levels (p < 0.02), but no significant change in the other study parameters in the F group. The changes in hormonal parameters were not correlated with the changes in lipid parameters in any of the groups. The decline in hirsutism scores was similar between the two groups (p = 0.56). No side effects were observed in either of the treatment groups. In conclusion our data indicate that (1) flutamide is as effective as ethynilestradiol in the treatment of hirsutism, (2) flutamide lowers serum cholesterol levels as does ethynilestradiol.
6 - Type 2 Diabetes Mellitus and Postmenopausal Osteoporosis - 2000
Uluslararası Bildiriler 23rd Congress of Endocrinology and Metabolic Diseases of Turkey Joint Meeting with the Europan Federation of Endocrine Societies, Ankara, A107, 58, Journal of Endocrinologıcal Investigation Vol. 23 (Suppl. To no. 7) 2000
ABSTRACT
Diabetes melitus is a chronic disease that affects all organ systems in human body. Whether the presence of type II diabetes mellitus has any effect on bone mineral density is not known. This study is performed in order to find out the effect of type II diabetes mellitus on bone mineral density (BMD) before and after antiresorptive therapy in postmenopausal patients. Twenty postmenopausal osteoporotic patients with type II diabetes mellitus, and 131 age-matched control patients are involved in the study. After establishment of osteoporosis, all of the diabetic and nondiabetic patients are put on antiresorptive treatment with biphosphonates and calcium. Pre- and post-treatment BMD levels are compared within and between the two goups. Diabetic patients had a mean diabetes duration of 7.9 ± 6.5 years. Patients with diabetes mellitus were comparable to nondiabetic patients with regard to age (62.7 ± 8.6 vs. 60.8 ± 6.0 years, respectively; p > 0.05), age at menopause (45.7 ± 6.6 vs. 46.8 ± 5.2 years, respectively; p > 0.05), duration of menopause (17.1 ± 8.6 vs. 14.0 ± 6.5 years, respectively; p > 0.05), and pretreatment BMD (0.762 ± 0.10 vs. 0.768 ± 0.11,respectively; p > 0.05). Antiresorptive treatment resulted in 5.4 % increase in BMD (∆ BMD) in the diabetic patients goup (from 0.762 ± 0.10 to 0.801 ± 0.10; p < 0.001), and 6.4 % increase in BMD in the nondiabetic group (from 0.768 ± 0.11 to 0.811 ± 0.12; p <0.001). The ∆ BMD was not different between the two goups (p < 0.05). There was a strong correlation between ∆ BMD and duration of diabetes (r = 0.64; p = 0.008). In conclusion, our data reveal that the presence of diabetes mellitus does not affect the severity of osteoporosis in postmenopausal patients. Also, the efficacy of antiresorptive treatment is not influenced by diabetes mellitus. The relation between the duration of diabetes and the change in BMD needs further clarification
5 - Relation Between Dehydroepiandrosterone Sulfate and Spinal Bone Mineral Density in Postmenopausal Women - 2000
Uluslararası Bildiriler 23rd Congress of Endocrinology and Metabolic Diseases of Turkey Joint Meeting with 88the Europan Federation of Endocrine Societies, Ankara, A106, 57, Journal of Endocrinologıcal Investigation Vol. 23 (Suppl. To no. 7) 2000
ABSTRACT
Osteoporosis is one of the most important causes of morbidity and mortality in postmenopausal women. Because osteoporosis is preventable it is important to predict the development of osteoporosis. One of the hypothesized predictors of postmenopausal osteoporosis is dehydroepiandrosterone sulfate (DHEA-S). Whether DHEA-S levels are different in osteoporotic women than those without osteoporosis is still controversial. The aim of this study was to investigate whether DHEA-S levels are related to osteoporosis in postmenopausal women. Thirty-three women with postmenopausal osteoporosis are involved in the study. Twenty-nine age and BMI matched women without osteoporosis formed the control group. After detailed physical examination, morning fasting blood samples are obtained from each subject for the measurement of DHEA-S levels. Mann Whitney U test and bivariate correlation analysis according to Spearman are performed for the statistical analysis, using SPSS software. Data are expressed as means ± S.D., and a probability value < 0.05 is considered as statistically significant. Lumbar spinal bone mineral density was significantly lower in the osteoporotic patients (0.672 ± 0.58 vs. 1.014 ± 0.73, respectively; p < 0.001). The difference of DHEA-S levels between the osteoporotic patients and the control group was not statistically significant (76.0 ± 53.7 vs. 92.0 ± 65.2, respectively, p > 0.05). Bone mineral density was significantly related to weight (r = 0.58; p < 0.001) and BMI (r = 0.40; p = 0.019) in the patient group, but not in the control group. DHEA-S showed no significant correlation. Our results show that DHEA-S levels are not different in postmenopausal women with and without osteoporosis. The significant relation between BMI and bone mineral density reflects the preventive role of high body weight against osteoporosis, compatible with the previous reports.
4 - Effects of Granulocyte-colony Stimulating Factor in the Treatment of Diabetic Foot Infection - 2000
Uluslararası Bildiriler 23rd Congress of Endocrinology and Metabolic Diseases of Turkey Joint Meeting with the Europan Federation of Endocrine Societies, Ankara, A87, 48, Journal of Endocrinologıcal Investigation Vol. 23 (Suppl. To no. 7) 2000
ABSTRACT
Foot infections are prevalent and cause substantial morbidity and mortality in patients with diabetes mellitus. The aim of this study was to investigate the effects of Granulocyte-colony stimulating factor (G-CSF) in the treatment of foot infections in diabetic patients. Thirty diabetic patients with pedal cellulitis or Wagner's grade 2 or less lesion on their feet were included in the study. The first group (6 females and 9 males) received classical treatment, consisting of local wound care and parenteral antibiotherapy in combination, while the second group (7 females and 8 males) received recombinant human G-CSF in addition to classical therapy. Time to resolution of infection, time to hospital discharge, need for surgical intervention and effects of G-CSF on the neutrophil functions (phagocytosis and oxidative burst) were the study objectives. Treatment with G-CSF led to significantly higher neutrophil counts at the 5.th and 10th days, and at the end of treatment in the G-CSF treated group compared to the standard goup. Respiratory burst of neutrophils increased significantly in both the G-CSF group (from 1.6±0.3 to 2.3±0.5, p=0.001) and the standard goup (from 2.0±0.4 to 2.3±0.4, p=0.02) with treatment. But, while phagocytosis of neutrophils increased significantly in the G-CSF group (from 70.4±2.0 to 74.5±1.9, p=0.004), it did not change significantly in the standard goup (from 68.1±0.2 to 69.4±1.9, p=0.3) with treatment. Duration of hospitalisation (26.9±2.0 vs. 28.3 days, p<0.05), duration of parenteral antibiotic administration (22.9±2.0 vs. 23.3±1.9 days, p<0.05), time to resolution of infection (23.6±1.8 vs. 22.3±1.7 days, p<0.05), and need for amputation (13.3% vs. 20%, p>0.05) were similar between the G-CSF and the standard groups. In conclusion, although G-CSF improves neutrophil function besides increasing the absolute numbers, this improvement is not associated with shortening of duration of antibiotic administration, duration of hospital stay or need for amputation in diabetic foot infection.
4. Effects of Granulocyte-colony Stimulating Factor in the Treatment of Diabetic Foot Infection
Author(s): Yonem, A (Yonem, A); Cakir, B (Cakir, B); Guler, S (Guler, S); Azal, O (Azal, O);
Corakci, A (Corakci, A)
Source: DIABETES OBESITY & METABOLISM
Volume: 3 Issue: 5 Pages: 332-337
Published: OCT 2001
Times Cited: 42
38. Interventions in the management of infection in the foot in diabetes: a systematic review
Author(s): Peters, EJ (Peters, E. J.); Lipsky, BA (Lipsky, B. A.); Aragon-Sanchez, J (Aragon-
Sanchez, J.); Boyko, EJ (Boyko, E. J.); Diggle, M (Diggle, M.); Embil, JM (Embil, J. M.);
Kono, S (Kono, S.); Lavery, LA (Lavery, L. A.); Senneville, E (Senneville, E.); Urbancic-
Rovan, V (Urbancic-Rovan, V.); Van Asten, SA (Van Asten, S. A.); Jeffcoate, WJ (Jeffcoate,
W. J.)
Group Author(s): Int Working Grp Diabet Foot
Source: DIABETES-METABOLISM RESEARCH AND REVIEWS
Volume: 32 Pages: 145-153
Supplement: 1
Published: JAN 2016
37. Effectiveness of interventions to enhance healing of chronic ulcers of the foot in diabetes: a
systematic review
Author(s): Game, FL (Game, F. L.); Apelqvist, J (Apelqvist, J.); Attinger, C (Attinger, C.);
Hartemann, A (Hartemann, A.); Hinchliffe, RJ (Hinchliffe, R. J.); Londahl, M (Londahl, M.);
Price, PE (Price, P. E.); Jeffcoate, WJ (Jeffcoate, W. J.)
Group Author(s): Int Working Grp Diabet Foot IWGDF
Source: DIABETES-METABOLISM RESEARCH AND REVIEWS
Volume: 32 Pages: 154-168
Supplement: 1
Published: JAN 2016
36. A pilot study evaluating non-contact low-frequency ultrasound and underlying molecular
mechanism on diabetic foot ulcers
Author(s): Yao, M (Yao, Min); Hasturk, H (Hasturk, Hatice); Kantarci, A (Kantarci, Alpdogan);
Gu, GS (Gu, Guosheng); Garcia-Lavin, S (Garcia-Lavin, Silvia); Fabbi, M (Fabbi, Matteo);
Park, N (Park, Nanjin); Hayashi, H (Hayashi, Hisae); Attala, K (Attala, Khaled); French, MA
(French, Michael A.); Driver, VR (Driver, Vickie R.)
Source: INTERNATIONAL WOUND JOURNAL
Volume: 11 Issue: 6 Pages: 586-593
Published: DEC 2014
35. Diagnosis and Management of Infection in the Diabetic Foot
Author(s): Peters, EJG (Peters, Edgar J. G.); Lipsky, BA (Lipsky, Benjamin A.)
Source: MEDICAL CLINICS OF NORTH AMERICA
Volume: 97 Issue: 5 Pages: 911-+
Published: SEP 2013
34. Granulocyte-colony stimulating factors as adjunctive therapy for diabetic foot infections
Author(s): Cruciani, M (Cruciani, Mario); Lipsky, BA (Lipsky, Benjamin A.); Mengoli, C
(Mengoli, Carlo); de Lalla, F (de Lalla, Fausto)
Source: COCHRANE DATABASE OF SYSTEMATIC REVIEWS
Issue: 8 Article Number: CD006810
Published: 2013
33. From Ulcer to Infection: An Update on Clinical Practice and Adjunctive Treatments of
Diabetic Foot Ulcers
Author(s): Abad, C (Abad, C.); Safdar, N (Safdar, N.)
Source: CURRENT INFECTIOUS DISEASE REPORTS
Volume: 14 Issue: 5 Pages: 540-550
Published: OCT 2012
32. 2012 Infectious Diseases Society of America Clinical Practice Guideline for the Diagnosis
and Treatment of Diabetic Foot Infections
Author(s): Lipsky, BA (Lipsky, Benjamin A.); Berendt, AR (Berendt, Anthony R.); Cornia, PB
(Cornia, Paul B.); Pile, JC (Pile, James C.); Peters, EJG (Peters, Edgar J. G.); Armstrong, DG
(Armstrong, David G.); Deery, HG (Deery, H. Gunner); Embil, JM (Embil, John M.); Joseph,
WS (Joseph, Warren S.); Karchmer, AW (Karchmer, Adolf W.); Pinzur, MS (Pinzur, Michael
S.); Senneville, E (Senneville, Eric)
Source: CLINICAL INFECTIOUS DISEASES
Volume: 54 Issue: 12 Pages: E132-U232
Published: JUN 15 2012
31. Diagnostics and treatment of the diabetic foot
Author(s): Apelqvist, J (Apelqvist, Jan)
Source: ENDOCRINE
Volume: 41 Issue: 3 Pages: 384-397
Published: JUN 2012
30. A systematic review of the effectiveness of interventions in the management of infection in
the diabetic foot
Author(s): Peters, EJG (Peters, E. J. G.); Lipsky, BA (Lipsky, B. A.); Berendt, AR (Berendt, A.
R.); Embil, JM (Embil, J. M.); Lavery, LA (Lavery, L. A.); Senneville, E (Senneville, E.);
Urbancic-Rovan, V (Urbancic-Rovan, V.); Bakker, K (Bakker, K.); Jeffcoate, WJ (Jeffcoate, W.
J.)
Source: DIABETES-METABOLISM RESEARCH AND REVIEWS
Volume: 28 Pages: 142-162 DOI: 10.1002/dmrr.2247
Supplement: 1
Published: FEB 2012
29. Consensus document on treatment of infections in diabetic foot
Author(s): Mompo, JIB (Blanes Mompo, Jose Ignacio)
Source: REVISTA ESPANOLA DE QUIMIOTERAPIA
Volume: 24 Issue: 4 Pages: 233-262
Published: DEC 2011
28. Standardization of Wound Photography Using the Wound Electronic Medical Record
Author(s): Rennert, R (Rennert, Robert); Golinko, M (Golinko, Michael); Kaplan, D (Kaplan,
Dave); Flattau, A (Flattau, Anna); Brem, H (Brem, Harold)
Source: ADVANCES IN SKIN & WOUND CARE
Volume: 22 Issue: 1 Pages: 32-38
Published: JAN 2009
27. Granulocyte-colony stimulating factors as adjunctive therapy for diabetic foot infections
Author(s): Cruciani, M (Cruciani, M.); Lipsky, BA (Lipsky, B. A.); Mengoli, C (Mengoli, C.);
de Lalla, F (de Lalla, F.)
Source: COCHRANE DATABASE OF SYSTEMATIC REVIEWS
Issue: 3 Article Number: CD006810
Published: 2009
26. Probiotics for patients with liver cirrhosis: Reply
Author(s): Stadlbauer, V (Stadlbauer, Vanessa); Mookerjee, RP (Mookerjee, Rajeshwar P.);
Jalan, R (Jalan, Rajiv)
Source: JOURNAL OF HEPATOLOGY
Volume: 49 Issue: 6 Pages: 1081-1082
Published: DEC 2008
25. Growth factors and cytokines in wound healing
Author(s): Barrientos, S (Barrientos, Stephan); Stojadinovic, O (Stojadinovic, Olivera);
Golinko, MS (Golinko, Michael S.); Brem, H (Brem, Harold); Tomic-Canic, M (Tomic-Canic,
Marjana)
Source: WOUND REPAIR AND REGENERATION
Volume: 16 Issue: 5 Pages: 585-601
Published: SEP-OCT 2008
24. A systematic review of the effectiveness of interventions to enhance the healing of chronic
ulcers of the foot in diabetes
Author(s): Hinchliffe, RJ (Hinchliffe, R. J.); Valk, GD (Valk, G. D.); Apelqvist, J (Apelqvist,
J.); Armstrong, DG (Armstrong, D. G.); Bakker, K (Bakker, K.); Game, FL (Game, F. L.);
Hartemann-Heurtier, A (Hartemann-Heurtier, A.); Londahl, M (Londahl, M.); Price, PE (Price,
P. E.); van Houtum, WH (van Houtum, W. H.); Jeffcoate, WJ (Jeffcoate, W. J.)
Source: DIABETES-METABOLISM RESEARCH AND REVIEWS
Volume: 24 Pages: S119-S144
Supplement: 1
Published: MAY-JUN 2008
23. Overview of diabetic foot; novel treatments in diabetic foot ulcer
Author(s): Larijani, B (Larijani, B.); Hasani, RS (Hasani, Ranjbar S.)
Source: DARU-JOURNAL OF FACULTY OF PHARMACY
Volume: 16 Pages: 1-6
Supplement: 1
Published: FEB 2008
22. Infections in diabetes mellitus and hyperglycemia
Author(s): Gupta, S (Gupta, Smita); Koirala, J (Koirala, Janak); Khardori, R (Khardori,
Romesh); Khardori, N (Khardori, Nancy)
Source: INFECTIOUS DISEASE CLINICS OF NORTH AMERICA
Volume: 21 Issue: 3 Pages: 617-+
Published: SEP 2007
21. Perioperative prophylaxis with granulocyte colony-stimulating factor (G-CSF) in high-risk
colorectal cancer patients for an improved recovery: A randomized, controlled trial
Author(s): Bauhofer, A (Bauhofer, Artur); Plaul, U (Plaul, Ulrike); Torossian, A (Torossian,
Alexander); Koller, M (Koller, Michael); Stinner, B (Stinner, Benno); Celik, I (Celik, Ilhan);
Sitter, H (Sitter, Helmut); Greger, B (Greger, Bernd); Middeke, M (Middeke, Martin); Schein,
M (Schein, Moshe); Wyatt, J (Wyatt, Jeremy); Nystrom, PO (Nystrom, Per-Olof); Hartung, T
(Hartung, Thomas); Rothmund, M (Rothmund, Matthias); Lorenz, W (Lorenz, Wilfried)
Source: SURGERY
Volume: 141 Issue: 4 Pages: 501-510
Published: APR 2007
20. Polymorphonuclear leucocyte respiratory burst activity correlates with serum zinc level in
type 2 diabetic patients with foot ulcers
Author(s): Larijani, B (Larijani, B.); Shooshtarizadeh, P (Shooshtarizadeh, P.); Mosaffa, N
(Mosaffa, N.); Heshmat, R (Heshmat, R.)
Source: BRITISH JOURNAL OF BIOMEDICAL SCIENCE
Volume: 64 Issue: 1 Pages: 13-17
Published: 2007
19. Common infections in diabetes: pathogenesis, management and relationship to glycaemic
control
Author(s): Peleg, AY (Peleg, Anton Y.); Weerarathna, T (Weerarathna, Thilak); McCarthy, JS
(McCarthy, James S.); Davis, TME (Davis, Timothy M. E.)
Source: DIABETES-METABOLISM RESEARCH AND REVIEWS
Volume: 23 Issue: 1 Pages: 3-13
Published: JAN 2007
18. Optimising antimicrobial therapy in diabetic foot infections
Author(s): Rao, N (Rao, Nalini); Lipsky, BA (Lipsky, Benjamin A.)
Source: DRUGS
Volume: 67 Issue: 2 Pages: 195-214
Published: 2007
17. Management of diabetic foot infections. Long text
Author(s): Stahl, JP (Stahl, Jean-Paul)
Source: MEDECINE ET MALADIES INFECTIEUSES
Volume: 37 Issue: 1 Pages: 26-50
Published: JAN 2007
16. Topical granulocyte colony-stimulating factor for the treatment of oral and genital ulcers of
patients with Behcet's disease
Author(s): Bacanli, A (Bacanli, A.); Dicle, OY (Dicle, O. Yerebakan); Parmaksizoglu, B
(Parmaksizoglu, B.); Yilmaz, E (Yilmaz, E.); Alpsoy, E (Alpsoy, E.)
Source: JOURNAL OF THE EUROPEAN ACADEMY OF DERMATOLOGY AND
VENEREOLOGY
Volume: 20 Issue: 8 Pages: 931-935
Published: SEP 2006
15. Systematic review of antimicrobial treatments for diabetic foot ulcers
Author(s): Nelson, EA (Nelson, EA); O'Meara, S (O'Meara, S); Golder, S (Golder, S); Dalton, J
(Dalton, J); Craig, D (Craig, D); Iglesias, C (Iglesias, C)
Source: DIABETIC MEDICINE
Volume: 23 Issue: 4 Pages: 348-359
Published: APR 2006
14. A series of systematic reviews to inform a decision analysis for sampling and treating
infected diabetic foot ulcers
Author(s): Nelson, EA (Nelson, EA); O'Meara, S (O'Meara, S); Craig, D (Craig, D); Iglesias, C
(Iglesias, C); Golder, S (Golder, S); Dalton, J (Dalton, J); Claxton, K (Claxton, K); Bell-Syer,
SEM (Bell-Syer, SEM); Jude, E (Jude, E); Dowson, C (Dowson, C); Gadsby, R (Gadsby, R);
O'Hare, P (O'Hare, P); Powell, J (Powell, J)
Source: HEALTH TECHNOLOGY ASSESSMENT
Volume: 10 Issue: 12 Pages: 1-+
Published: APR 2006
13. Granulocyte colony-stimulating factor prophylaxis improves survival and inflammation in a
two-hit model of hemorrhage and sepsis
Author(s): Bauhofer, A (Bauhofer, A); Lorenz, W (Lorenz, W); Kohlert, F (Kohlert, F);
Torossian, A (Torossian, A)
Source: CRITICAL CARE MEDICINE
Volume: 34 Issue: 3 Pages: 778-784
Published: MAR 2006
12. A systematic approach to diabetic foot infections
Author(s): Zgonis, T (Zgonis, T); Roukis, TS (Roukis, TS)
Source: ADVANCES IN THERAPY
Volume: 22 Issue: 3 Pages: 244-262
Published: MAY-JUN 2005
11. Are granulocyte colony-stimulating factors beneficial in treating diabetic foot infections? A
meta-analysis
Author(s): Cruciani, M (Cruciani, M); Mengoli, C (Mengoli, C); Lipsky, BA (Lipsky, BA); De
Lalla, F (De Lalla, F)
Source: DIABETES CARE
Volume: 28 Issue: 2 Pages: 454-460
Published: FEB 2005
10. The effects of granulocyte colony-stimulating factor in preclinical models of infection and
acute inflammation
Author(s): Marshall, JC (Marshall, JC)
Source: SHOCK Volume: 24 Pages: 120-129
Supplement: 1
Published: 2005
9. Adjunctive granulocyte colony-stimulating factor therapy for diabetic foot infections
Author(s): Reed, KS (Reed, KS); Pai, MP (Pai, MP)
Source: ANNALS OF PHARMACOTHERAPY
Volume: 38 Issue: 12 Pages: 2150-2153
Published: DEC 2004
8. New and experimental approaches to treatment of diabetic foot ulcers: a comprehensive
review of emerging treatment strategies
Author(s): Eldor, R (Eldor, R); Raz, I (Raz, I); Ben Yehuda, A (Ben Yehuda, A); Boulton, AJM
(Boulton, AJM)
Source: DIABETIC MEDICINE
Volume: 21 Issue: 11 Pages: 1161-1173
Published: NOV 2004
7. Diagnosing and treating diabetic foot infections
Author(s): Lipsky, BA (Lipsky, BA); Berendt, AR (Berendt, AR); Embil, J (Embil, J); de Lalla,
F (de Lalla, F)
Source: DIABETES-METABOLISM RESEARCH AND REVIEWS
Volume: 20 Pages: S56-S64
Supplement: 1
Published: MAY-JUN 2004
6. A report from the international consensus on diagnosing and treating the infected diabetic
foot
Author(s): Lipsky, BA (Lipsky, BA)
Source: DIABETES-METABOLISM RESEARCH AND REVIEWS
Volume: 20 Pages: S68-S77
Supplement: 1
Published: MAY-JUN 2004
5. Is there a place for granulocyte colony-stimulating factor in non-neutropenic critically ill
patients?
Author(s): Azoulay, E (Azoulay, E); Delclaux, C (Delclaux, C)
Source: INTENSIVE CARE MEDICINE
Volume: 30 Issue: 1 Pages: 10-17
Published: JAN 2004
4. Diabetic foot ulcers
Author(s): Jeffcoate, WJ (Jeffcoate, WJ); Harding, KG (Harding, KG)
Source: LANCET
Volume: 361 Issue: 9368 Pages: 1545-1551
Published: MAY 3 2003
3. Growth factors in the treatment of diabetic foot ulcers
Author(s): Bennett, SP (Bennett, SP); Griffiths, GD (Griffiths, GD); Schor, AM (Schor, AM);
Leese, GP (Leese, GP); Schor, SL (Schor, SL)
Source: BRITISH JOURNAL OF SURGERY
Volume: 90 Issue: 2 Pages: 133-146
Published: FEB 2003
2. Evaluation of granulocyte-colony stimulating factor (Filgrastim) in infected diabetic foot
ulcers
Author(s): Kastenbauer, T (Kastenbauer, T); Hornlein, B (Hornlein, B); Sokol, G (Sokol, G);
Irsigler, K (Irsigler, K)
Source: DIABETOLOGIA
Volume: 46 Issue: 1 Pages: 27-30
Published: JAN 2003
1. Induction and regulation of endogenous granulocyte colony-stimulating factor formation
Author(s): Hareng, L (Hareng, L); Hartung, T (Hartung, T)
Source: BIOLOGICAL CHEMISTRY
Volume: 383 Issue: 10 Pages: 1501-1517
Published: OCT 2002
3 - Circadian change in thyroid volume in healthy individuals - 1999
Uluslararası Bildiriler European Thyroid Association Annual Meeting, Absracts, 99, P-129, Scotland, UK
ABSTRACT
Aim:To evaluate thyroid volume at the circadian nadir and peak of TSH levels.
Materials and Methods: Serum TSH, fT3 and fT4 levels and thyroid volumes are measured at 09.00 AM and 24.00 in 55 (20 M, 35 F) euthyroid healthy individuals.
Results:Mean TSH level was significantly lower at 09.00 AM than at 24.00 (1.95±1.29 vs. 2.52±1.5 µIU/ml, p<0.001). Mean thyroid volume was also significantly lower at 09.00 AM than at 24.00 (15.09±4.97 vs. 17.38±3.49, p<0.001 ). There was no relation between TSH level and thyroid volume at any time points.
Conclusion:Although thyroid volume and TSH levels increase at midnight compared to 09.00 AM there is no relation between the increase in these two parameters.
2 - Relatıon of Leptin with Metabolic Parameters in Female Patients with Non-insulin Dependent Diabetes Mellitus - 1999
Uluslararası Bildiriler 35th Annual Meeting of European association for the study of diabetes, Brussels, A 192, 721 Diabetologia Volume 42. Supplement 1. 1999
ABSTRACT
Aim:To evaluate the relation of leptin with metabolic control parameters and the effect of 14 days of diet or diet-oral antidiabetic therapy on leptin concentration in female patients with non-insulin dependet diabetes mellitus (NIDDM).
Materyals and Methods:51 female patients with NIDDM are treated with diet alone or diet oplus glipizide-GITS, or gliclazide or metformin for 14 days. Plasma leptin is mesaured in basal and post-treatment period along with the metabolic markers. 35 healthy female subjects formed the control group.
Results:Leptin levels were similar both at baseline (15.9±7.4 vs 18.3±17.7 respectively) and after treatment (15.4±7.5 vs 18.3±17.7 respectively) in diabetic and control groups. NIDDM patients with basal fasting plasma glucose (FPG)<180 mg/dL had significantly higher leptin levels than NIDDM patients with basal FPG>=180 mg/dL (19.6±8.7 vs. 13.65±5.4 respectively; p<0.05). Patients with basal PPPG<250 mg/dL also showed higher leptin levels than those with basal postprandial plasma glucose PPPG>=250 mg/dL (20.2±7.9 vs 12.9±5.2, respectively; p<0.05). Mode of treatment did not influence leptin levels ∆ leptin showed a weak correlation with basal FPG (r=0.346; p<0.05), basal and post-treatment PPPG (r=0.335, p<0.05 and r=0.325, p<0.05, respectively) and a moderate correlation with post-treatment FPG levels (r=0.391, p<0.01) in patients with NIDDM.
Conclustions:Leptin levels are similar between female patients with NIDDM and healthy females: 27 improvement in FPG and PPPG levels do not influence leptin levels in short term out; 3 change in leptin level by treatment is positively correiated to FPG and PPPG levels. We conclude that leptin level is not affected by the presence of NIDDM and by short term treatment with diet alone or diet plus different oral antidiabetes out directly related to metabolic control in female patients with NIDDM.
1 - Case report Werner’s syndrome - 1997
Uluslararası Bildiriler 16th IDF Congress, Helsinki , A 172 , 674, Helsinki, 1997